
Abstract
Objective
Digestive system tumors (DST) remain a major contributor to the global cancer burden. This study aimed to characterize the adverse events (AEs) spectrum, identify potential safety signals, and explore subgroup-specific reporting patterns and time-to-onset features of immune checkpoint and targeted inhibitors in DST using the FDA Adverse Event Reporting System (FAERS).
Methods
This was a retrospective observational pharmacovigilance study based on spontaneous reports submitted to FAERS from 2004Q1 to 2024Q4. The study population comprised FAERS reports involving patients with DST who received PD-1, PD-L1, CTLA-4, HER2, EGFR, VEGF, or VEGFR inhibitors. Reports were retrieved through OpenVigil 2.1 and coded using Medical Dictionary for Regulatory Activities preferred terms. After data cleaning, disproportionality analyses were performed using the reporting odds ratio and information component, with signal thresholds defined as ROR025 >1, IC025 >0, and at least three reports. Descriptive analyses, temporal trend analyses, subgroup analyses, and Weibull time-to-onset analyses were also conducted.
Results
A total of 41,168 eligible reports were included. Most reports involved male patients and individuals weighing 50–100 kg. VEGFR inhibitors accounted for the largest number of AE reports, whereas CTLA-4 inhibitors accounted for the fewest. Reporting trends generally increased over time, although fluctuations were observed across drug classes. At the preferred-term level, 131, 372, 38, 114, 274, 382, and 320 valid safety signals were identified for PD-1, PD-L1, CTLA-4, HER2, EGFR, VEGF, and VEGFR inhibitors, respectively. Frequently detected signals included disease progression, off-label use, and death. Stratified analyses suggested age- and sex-related differences in the reporting patterns of selected AEs across drug classes. Time-to-onset analysis showed an early-failure pattern for all investigated inhibitors, with the hazard of AE occurrence decreasing over time.
Conclusions
This FAERS-based retrospective pharmacovigilance study comprehensively characterized the AE reporting profiles of immune checkpoint and targeted inhibitors in DST. Multiple potential safety signals, subgroup-specific reporting patterns, and early-onset AE features were identified. These findings may support clinical risk monitoring, pharmacovigilance surveillance, and individualized safety assessment in patients with DST receiving immune checkpoint or targeted inhibitors.
1. Introduction
In many countries around the world, cancer remains a leading cause of premature death and reduced life expectancy, and it represents a significant burden on public health. 1 The digestive system, comprising the gastrointestinal tract and its accessory organs, represents a major anatomical and functional unit involved in digestion and nutrient absorption. Tumors arising from this system, collectively referred to as digestive system tumors (DST), constitute one of the leading causes of cancer-related morbidity and mortality worldwide.2,3 Recent global data indicate that there are over 4.8 million new cases of digestive system malignancies each year, including esophageal, liver, pancreatic, gastric, and colorectal cancers. 4 These have led to approximately 3.2 million deaths, accounting for nearly one-third of all cancer-related fatalities worldwide. 5 Most digestive system malignancies are diagnosed at locally advanced or metastatic stages, which are associated with a poor prognosis, making them one of the most pressing public health concerns. 6 Traditional oncologic interventions, including surgery, chemotherapy, radiotherapy, and targeted therapy, often fail to produce satisfactory outcomes in patients with advanced or metastatic digestive cancers. Beyond suboptimal therapeutic efficacy, these patients and long-term survivors increasingly encounter multifactorial challenges arising from both the disease itself and treatment-related sequelae. 7 These include not only physical and psychological impairments, but also medical, behavioral, and socioeconomic burdens that collectively compromise quality of life and impede sustained survival improvements. Accordingly, there is a growing need to explore alternative or combinatorial therapeutic strategies that can both prolong survival and mitigate these multidimensional consequences.8,9
Immune checkpoint inhibitors (ICIs) have emerged as a major class of anticancer agents by restoring antitumor immunity through blockade of inhibitory signaling pathways involved in T-cell activation. Owing to their broad biological activity across multiple tumor types, durable responses, and clinical efficacy even in metastatic or treatment-refractory settings, ICIs have become an important therapeutic cornerstone in contemporary oncology. 10 In digestive system tumors (DST), multiple ICIs, including programmed death-1 (PD-1) inhibitors, programmed death-ligand 1 (PD-L1) inhibitors, and cytotoxic T-lymphocyte-associated antigen-4 (CTLA-4) inhibitors, have been approved by the U.S. Food and Drug Administration (FDA) and incorporated into the treatment paradigm of several malignancies.11–15 At the same time, targeted therapies, including HER2-, EGFR-, VEGF-, and VEGFR-directed inhibitors, have also become integral components of systemic treatment for selected DST, either as monotherapy or in combination with immunotherapy and chemotherapy.16,17 With the continuing expansion of indications and the increasing use of combination regimens, both immune checkpoint inhibitors and targeted agents now occupy a central position in the comprehensive management of DST.
Despite their therapeutic benefits, these agents are associated with a broad spectrum of treatment-related adverse events that may substantially affect treatment continuity, quality of life, and clinical outcomes. For ICIs, immune-related adverse events (irAEs) arise from distinct immunologic mechanisms and may involve nearly any organ system, with variable onset and sometimes prolonged duration.18,19 Common toxicities include skin reactions, colitis, hepatitis, pneumonitis, nephritis, and endocrine dysfunction, particularly thyroid abnormalities. 20 Less frequent but potentially life-threatening toxicities, such as encephalitis, myocarditis, and hematologic complications, may present atypically and therefore be recognized late, resulting in severe consequences. 21 In parallel, targeted inhibitors used in DST are also associated with clinically important toxicities, including dermatologic reactions, hypertension, gastrointestinal symptoms, pulmonary events, and other organ-specific adverse effects, which may differ according to therapeutic class and treatment context. These issues deserve particular attention in DST because of the marked heterogeneity of tumor types, baseline organ dysfunction, nutritional impairment, and frequent use of multimodal treatment strategies. Moreover, symptoms such as diarrhea, abnormal liver function, malnutrition, and infection may overlap with disease-related manifestations or treatment-related toxicities, thereby complicating the recognition, differential diagnosis, and attribution of adverse events in routine practice.22–24
Although randomized controlled trials and some real-world studies have provided important information on the safety of ICIs and targeted therapies, the available evidence still has significant limitations. 25 Clinical trials usually enroll relatively selected populations under strict inclusion and exclusion criteria, and often lack sufficient sample size and follow-up duration to adequately identify rare, serious, or delayed adverse events. In real-world settings, however, patients with DST frequently present with underlying liver disease, malnutrition, organ dysfunction, polypharmacy, and exposure to combined treatment regimens, all of which may alter the actual safety profile observed in practice. In addition, adverse-event patterns may vary substantially across immune checkpoint inhibitors, targeted inhibitors, and their combinations, while low-frequency but clinically meaningful safety signals may remain underrecognized in conventional clinical studies. 26 Therefore, pharmacovigilance analyses based on large postmarketing spontaneous reporting systems are important for complementing trial-based evidence, identifying potential safety signals, and improving real-world safety management. 27 The FDA Adverse Event Reporting System (FAERS), one of the most widely used global pharmacovigilance databases, compiles large-scale real-world adverse event reports across multiple centers and long periods of observation, and thus provides a valuable resource for signal detection and characterization of drug safety profiles. 28
Although reports of adverse events associated with immune checkpoint and targeted inhibitors in DST have increased, systematic pharmacovigilance evidence remains limited, particularly with regard to comprehensive assessment of the adverse-event spectrum using large real-world databases. 29 Given the heterogeneity of the DST population, the diversity of treatment modalities, and the challenges in detecting and attributing adverse reactions, clarifying the real-world safety profile of these agents is of substantial clinical importance. To address this gap, we used the FAERS database to perform a systematic pharmacovigilance analysis of adverse events reported in patients with DST who received immune checkpoint or targeted inhibitors. Our aims were to identify potential safety signals, characterize the adverse-event spectrum, explore subgroup-specific risk patterns, and provide evidence to support clinical risk monitoring, early detection, and more rational use of these therapies in DST.
2. Materials and methods
2.1. Data extraction and screening
This retrospective study utilized the FAERS database (https://fis.fda.gov/extensions/FPD-QDE-FAERS/FPD-QDE-FAERS.html), which was analyzed ADEs associated with PD-1, PD-L1, CTLA-4, HER2, EGFR, VEGF, and VEGFR inhibitors in DST using the FDA Adverse FAERS database (2004-2024). 30 Data were extracted via OpenVigil 2.1, processed in SAS, and categorized using MedDRA Preferred Terms. Since this is a secondary data analysis, the reports were not consecutively, randomly, or selectively chosen from a patient cohort, but rather based on specific adverse event reports involving the mentioned therapies. Based on the References 31 and 32, the following data exclusion criteria were established to ensure the integrity and accuracy of the dataset. First, adverse event reports related to DST involving PD-1, PD-L1, CTLA-4, HER2, EGFR, VEGF, and VEGFR inhibitors were screened against FDA records, and reports associated with case identifiers that had been officially deleted, reused, or were missing were excluded to minimize errors caused by invalid or nontraceable case records. Second, reports with unreliable key variables were excluded according to predefined data-cleaning criteria. Specifically, reports were removed if demographic or clinical fields contained missing, contradictory, nonstandard, or noninterpretable information, including sex, age, reporter identity, serious outcome, and reported result. For example, records were excluded when age information was absent, recorded in an unrecognizable format or unit that could not be standardized, or was internally inconsistent; when sex was missing or contradictory within the same report; or when reporter type, serious outcome, or event result fields were incomplete, ambiguous, or inconsistently coded. These exclusion criteria were applied to improve data transparency, consistency, and reliability prior to signal detection. By doing so, we aimed to enhance the reliability of the data for subsequent analysis (Table S1). This study was conducted in accordance with the principles of the Declaration of Helsinki (1975, as revised in 2024). The reporting of this study conforms to the relevant Equator Network guidelines. Specifically, we followed the STROBE guidelines for observational studies. 33 No individual-level identifiable patient information was accessed, and no intervention involving human participants or animals was performed. Therefore, ethical approval was not required, and the requirement for informed consent was waived.
2.2. Data mining
This study employed disproportionality analysis using the reporting odds ratio (ROR) and lower limit of the information component (IC025) to detect safety signals of PD-1/PD-L1/CTLA-4/HER2/EGFR/VEGF/VEGFR inhibitors in DST-related adverse events. The method compares the observed-to-expected frequency of drug-event pairs against background data using a 2×2 contingency table (Tables S2-3).
Signal Detection Criteria:
ROR025: (lower limit of ROR 95% CI) >1.
IC025: (lower limit of IC 95% CI) >0.
Higher values indicate stronger signals (drug-ADE association). To enhance reliability, dual criteria (ROR+IC) were applied with a minimum report threshold (≥3 cases) to reduce false positives.
This study employed disproportionality analysis (ROR and IC025) for signal detection, with the criteria set as: lower bound of ROR 95% CI >1 and lower bound of IC 95% CI > 0, along with a minimum report threshold of ≥3 cases to enhance reliability, where higher values indicate stronger drug-event associations.
2.3. Statistical analysis
In this study, Microsoft Excel was used to screen the extracted data and summarize the basic characteristics of ADE reports and ADE signals. Categorical variables, such as sex and age, were presented as percentages (%). Data processing, data mining, and statistical analyses were performed using OpenVigil 2.1, SAS 9.4, R version 4.5.2, MySQL Community Server 8.0.45, Navicat Premium version 17.3.6, and GraphPad Prism version 10.1.2.
3. Results
3.1. Clinical characteristics and distribution of drug treatments for digestive system tumors (DST)
Baseline characteristics of FAERS reports included in the study for drugs used in DST (PD-1, PD-L1, CTLA-4, HER2, EGFR, VEGF, and VEGFR inhibitors).

HP=Health experts, MD=Doctors, CN=Consumers, PH=Pharmacist, OT=Other health-professional, LW=Lawyer.
3.2. Temporal trends in ICI therapy for DST
The results indicate that during the period from 2004 to 2024, the number of ADE reports associated with PD-1 and DST was relatively low, yet it exhibited a gradual upward trend, with a slight dip observed from 2019 to 2020. Likewise, the overall numbers of ADE reports for PD-1, HER2, and CTLA-4 were relatively small and demonstrated a slow upward tendency as well. In contrast, the overall quantities of ADE reports regarding VEGF and EGFR were relatively higher, yet they fluctuated over time. Among these target drugs, VEGFR had the largest number of ADE reports. Furthermore, the number of ADE reports related to DST witnessed an upward trend from 2004 to 2019, with a temporary decline from 2015 to 2016. Subsequently, it showed a downward trend from 2019 to 2024. Specifically for PD-L1, the number of ADE reports associated with DST displayed an upward trend from 2004 to 2022, but then shifted to a downward trend from 2022 to 2024. Overall, among all the investigated drugs, VEGFR stands out with the highest number of ADE reports, whereas CTLA-4 has the lowest number of such reports (Figure 1(a)–(b)). (a) shows the distribution of ADE reports related to different target drugs (PD-1, HER2, CTLA-4, VEGF, EGFR, PD-L1) from 2004 to 2024. It presents the initial distribution characteristics of ADE reports related to different target drugs in terms of case association and time dimension. It clearly shows that the number of VEGF-related ADE reports is the highest, while the number of CTLA-4-related ADE reports is the lowest. This provides basic data support for subsequent analysis of the time trend of ADE reports related to each target drug. (b) shows the time trend of the number of ADE reports related to different target drugs and their association with drug intervention. It displays the time trend of the number of ADE reports related to different target drugs during the period from 2004 to 2024, as well as their association with drug intervention. It can be clearly observed that the number of PD-1, HER2, and CTLA-4-related ADE reports is generally low and shows a slow upward trend. Among them, the number of PD-1 combined with DST-related ADE reports slightly decreased in 2019-2020; the number of VEGF and EGFR-related ADE reports is relatively higher but fluctuates over time; the number of DST-related ADE reports shows an upward trend from 2004 to 2019 (with a brief decrease in 2015-2016), and then turns to a downward trend from 2019 to 2024. The number of PD-L1 combined with DST-related ADE reports increases from 2004 to 2022 and then decreases from 2022 to 2024. At the same time, it can be clearly seen that the number of VEGFR-related ADE reports is the highest among all target drugs, and CTLA-4 has the lowest. This provides a visual basis for comprehensively evaluating the time trend of the safety of different target drugs and the impact of DST intervention on the number of ADE reports.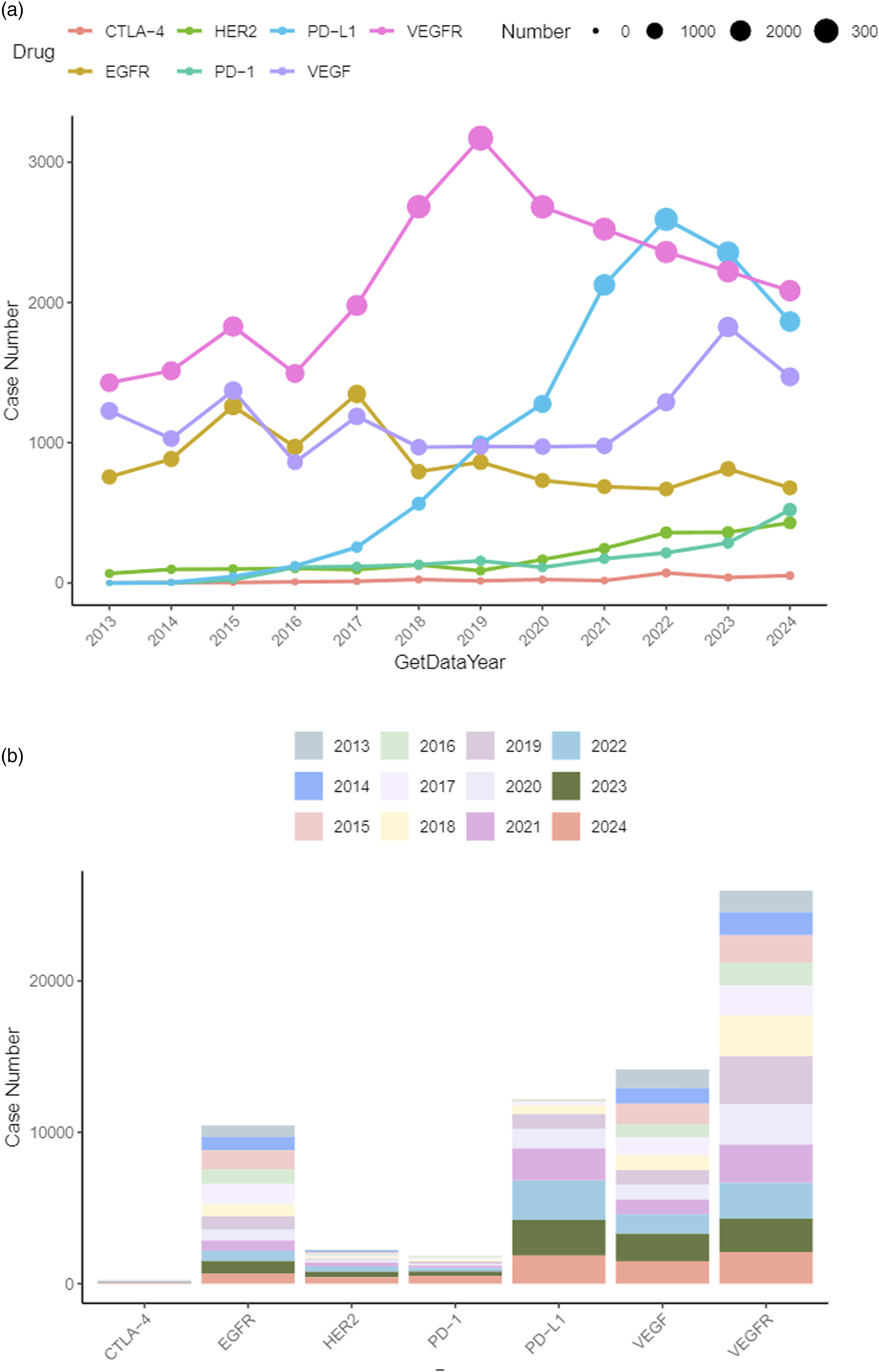
Figure 1(a) shows the distribution of ADE reports related to different target drugs (PD-1, HER2, CTLA-4, VEGF, EGFR, PD-L1) from 2004 to 2024. It presents the initial distribution characteristics of ADE reports related to different target drugs in terms of case association and time dimension. It clearly shows that the number of VEGF-related ADE reports is the highest, while the number of CTLA-4-related ADE reports is the lowest. This provides basic data support for subsequent analysis of the time trend of ADE reports related to each target drug.
Figure 1(b) shows the time trend of the number of ADE reports related to different target drugs and their association with drug intervention. It displays the time trend of the number of ADE reports related to different target drugs during the period from 2004 to 2024, as well as their association with drug intervention. It can be clearly observed that the number of PD-1, HER2, and CTLA-4-related ADE reports is generally low and shows a slow upward trend. Among them, the number of PD-1 combined with DST-related ADE reports slightly decreased in 2019-2020; the number of VEGF and EGFR-related ADE reports is relatively higher but fluctuates over time; the number of DST-related ADE reports shows an upward trend from 2004 to 2019 (with a brief decrease in 2015-2016), and then turns to a downward trend from 2019 to 2024. The number of PD-L1 combined with DST-related ADE reports increases from 2004 to 2022 and then decreases from 2022 to 2024. At the same time, it can be clearly seen that the number of VEGFR-related ADE reports is the highest among all target drugs, and CTLA-4 has the lowest. This provides a visual basis for comprehensively evaluating the time trend of the safety of different target drugs and the impact of DST intervention on the number of ADE reports.
3.3. ADE analysis from the perspective of the preferred term (PT) level in drug treatment for DST
Overview of PT-level adverse event signals for drugs used in DST based on FAERS.

This table summarizes, for each drug class used in DST, the total number of MedDRA Preferred Terms (PTs) detected (i.e., PTs with at least one DST-related FAERS report for the corresponding drug class) and the number and proportion of effective PT-level signals. Signal rate (%) was calculated as Effective signals/Total PT detected × 100.
Top 3 effective PT-level adverse event signals for drugs used in DST in FAERS.

The table lists the top 3 effective adverse event signals at the MedDRA Preferred Term (PT) level for each drug class/target used in DST. Signals are annotated by MedDRA System Organ Class (SOC), reporting counts, and signal-detection metrics from disproportionality and Bayesian approaches. A indicates the number of DST-related FAERS reports containing both the target drug class/target and the corresponding PT. Disproportionality metrics include the reporting odds ratio (ROR) with 95% confidence interval (CI) and the proportional reporting ratio (PRR) with chi-square statistic (χ2). Bayesian metrics include the empirical Bayes geometric mean (EBGM) from the Multi-item Gamma Poisson Shrinker (MGPS) method, where EBGM05 denotes the lower one-sided 95% credible bound, and the information component (IC) from the Bayesian Confidence Propagation Neural Network (BCPNN) method, where IC025 denotes the lower 95% credible bound. A PT was considered positive by each method if it met the following criteria: ROR signal: ROR lower 95% CI limit (RORL) > 1 and a ≥ 3; PRR signal: PRR ≥ 2, χ2 ≥ 4, and a ≥ 3; MGPS signal: EBGM05 > 2; BCPNN signal: IC025 > 0. Effective signal was defined as a PT positive in at least two of the four methods. PTs were ranked within each drug class/target by descending RORL (i.e., the lower bound of the 95% CI of ROR).
3.4. Risk stratified analysis
Through the stratified subgroup analysis according to age and gender, different potential high-risk situations were identified when various drugs were used for the treatment of DST. At the gender subgroup level, for PD-1, there might be a higher risk of treating DST at the PT level of “ANXIETY”; for PD-L1, a higher risk might exist at the PT level of “ENCEPHALOPATHY”; for VEGF, there could be a higher risk at the PT level of “BLOOD PRESSURE INCREASED”; for VEGFR, a higher risk might be present at the PT level of “ALOPECIA”; for HER2, a higher risk might occur at the PT level of “HEADACHE”; for EGFR, a higher risk might be seen at the PT level of “ALOPECIA”; and for CTLA-4, a higher risk might appear at the PT level of “ABDOMINAL PAIN”. At the age subgroup level, for PD-1, there might be a relatively high risk of treating DST at the PT level of “PRURITUS”; for PD-L1, a higher risk might exist at the PT level of “MUSCULAR weakness”; for VEGF, a relatively high risk could be present at the PT level of “INTERSTITIAL LUNG DISEASE”; for VEGFR, a higher risk might occur at the PT level of “FALL”; for HER2, a higher risk might be seen at the PT level of “OXYGEN SATURATION DECREASED”; for EGFR, a relatively high risk might appear at the PT level of “INTERSTITIAL LUNG DISEASE”; and for CTLA-4, a higher risk might exist at the PT level of “immune-mediated ENTEROCOLITIS”. In general, different drugs exhibit their respective potential risk characteristics when treating DST at specific PT levels within the two stratified dimensions of age and gender. These findings can provide a reference for subsequent risk assessment and rational drug use when applying corresponding drugs to different populations for the treatment of DST (Figure 2). . A stratified subgroup analysis by age and gender was conducted to explore the potential high-risk situations when multiple adverse reactions occurred during the use of different drugs (including 14 figures: (A-N). (a). CTLA-4 age-group, (b). CTLA-4 sex-group, (c). EGFR age-group, (d). EGFR sex-group, (e). HER2 age-group, (f). HER2 sex-group, (G). PD-1 age-group, (h). PD-1 sex-group, (i). PD-L1 age-group, (j). PD-L1 sex-group, (k). VEGF age-group, (l). VEGF sex-group, (m). VEGFR age-group, (n). VEGFR sex-group.
3.5. Time-trade-off (TTO) analysis
TTO analysis and WSP classification of ADEs associated with PD-1, PD-L1, CTLA-4, HER2, EGFR, VEGF, and VEGFR inhibitors in DST treatment based on FAERS.

4. Discussion
In this study, leveraging the FAERS database (2004–2024), we conducted a comprehensive assessment of ADEs associated with immune checkpoint inhibitors (PD-1, PD-L1, and CTLA-4 inhibitors) and targeted therapies, including HER2, EGFR, VEGF, and VEGFR inhibitors. By integrating drug-specific safety profiles with population-level risk heterogeneity and time-dependent toxicity patterns, our findings delineate distinct pharmacovigilance signals across therapeutic classes. These results not only enhance current understanding of safety characteristics in real-world practice but also provide evidence-based insights that may inform more rational treatment selection, individualized risk mitigation, and clinically optimized medication strategies in the management of digestive malignancies.
Previous studies indicate that long-term immunosuppressed populations, such as organ transplant recipients, exhibit a higher incidence of digestive tract malignancies, including colorectal and gastric cancers, compared to the general population.34,35 This suggests that continuous immune surveillance suppression weakens the body’s ability to eliminate heterologous clones, fostering an environment conducive to tumor development. Similarly, digestive tract tumors often exist in an “immunosuppressive” microenvironment. The KEYNOTE-966 study highlighted that most advanced biliary tract tumors respond poorly to single-agent PD-1 inhibitors, necessitating a combination of gemcitabine/cisplatin chemotherapy with pembrolizumab to enhance survival. However, this approach also increases the incidence of grade 3-4 adverse reactions, illustrating the compounded effects of immune activation and chemotherapy toxicity.
36
A network meta-analysis by Han et al. further demonstrated that the combination of ICIs with platinum- and fluorouracil-based regimens markedly increases the risk of hematological toxicities, including anemia, neutropenia, and thrombocytopenia. These adverse events are likely driven by excessive T-cell activation and cytokine-mediated disruption of the bone marrow microenvironment, which collectively impair hematopoietic function and precipitate treatment-related blood abnormalities.
37
Mechanistically, Sangro et al. noted that ICIs enhance effector T cell function and reverse the “exhaustion” phenotype by blocking PD-1/PD-L1 or CTLA-4 signals, while also disrupting the physiological immune tolerance of the liver-gut axis. This disruption induces inflammatory infiltration in hepatic sinusoids and portal areas, bile duct epithelial injury, and immune-mediated inflammation of the colonic mucosa, leading to irAEs such as hepatitis, colitis, and upper gastrointestinal symptoms.
30
The overall incidence of irAEs in patients with digestive system tumors ranges from 2% to 40%, influenced by factors like underlying liver diseases, intestinal flora, and combined treatment methods30,38
Digestive tract tumors are prevalent worldwide, representing about a quarter of all new cancer cases, and their incidence notably rises with age, classifying them as typical “age-related malignant tumors”.39,40 In childhood and adolescence, these tumors are rare due to limited exposure time, robust cell repair capabilities, and effective immune surveillance. However, after reaching middle age, particularly beyond 50, the incidence of gastric, esophageal, and colorectal cancers escalates sharply, peaking between ages 60 and 70. This trend is linked to the accumulation of risk factors, including “inflammatory aging,” chronic infection with Helicobacter pylori or hepatitis viruses, prolonged smoking and drinking, and an unbalanced diet.41,42 Such epidemiological characteristics are likely to shape the occurrence patterns of ADEs associated with ICIs and targeted therapies. Based on FAERS data from 2004–2024, our analysis focusing on seven agents commonly used in the treatment of digestive system tumors—including PD-1, PD-L1, CTLA-4, and multiple targeted inhibitors—revealed that age, sex, and body weight are key population determinants influencing ADE risk. The following discussion integrates mechanistic insights with clinical evidence to further elucidate how these patient-specific factors contribute to differential toxicity profiles and guide risk-adapted therapeutic decision-making.
Although immune checkpoint inhibitors (PD-1, PD-L1, and CTLA-4 inhibitors) and targeted agents (HER2, EGFR, VEGF, and VEGFR inhibitors) differ substantially in their mechanisms of action and toxicity profiles, they were included within the same pharmacovigilance framework in the present study because all of these agents are major systemic therapies widely used in the management of digestive system tumors, often in overlapping clinical settings and, in some cases, as part of combination or sequential treatment strategies. Importantly, our intention was not to treat these agents as a biologically homogeneous group or to generate a single pooled safety estimate across all drugs. Rather, we used a common disease context (DST) and a unified pharmacovigilance framework to characterize and compare class-specific adverse-event patterns in real-world practice. In the actual analyses, signal detection, PT-level evaluation, subgroup stratification, and time-to-onset assessment were conducted separately for each drug class, thereby preserving their mechanistic and clinical distinctions. Nevertheless, because these therapies are used in different treatment settings and patient populations, cross-class comparisons should be interpreted with caution. Therefore, the present study should be understood primarily as a comparative and stratified pharmacovigilance assessment of multiple major therapeutic classes used in DST, rather than as a pooled analysis assuming equivalence among them.
Based on FAERS data, this study further confirms that, compared with patients aged 18–64.9 years, those aged 65 years and older exhibit significantly higher RORs for several serious ADEs, including complete atrioventricular block and heart failure. The risk of adverse outcomes is further increased in elderly patients with comorbidities such as hypertension and diabetes. This can be attributed to two main factors. First, immunosenescence in older adults, characterized by reduced T-cell function and an imbalance in regulatory T-cell populations, makes ICI-induced immune activation more prone to dysregulation, increasing the likelihood of organ-specific inflammatory damage. 43 Second, age-related declines in hepatic and renal function, combined with comorbid conditions, reduce drug metabolism capacity, for example through decreased CYP450 enzyme activity, thereby amplifying ICI-associated cardiotoxic and hepatotoxic effects.44,45 Together with our TTO analysis showing an early onset pattern of ADEs, these findings emphasize the importance of close monitoring of cardiac biomarkers, such as troponin, and liver function, including ALT and AST, during the initial phase of ICI therapy, particularly within the first 30 days, to prevent severe adverse outcomes in elderly patients. Sex-based differences constitute another critical determinant in ADE risk stratification.
In this study, male patients exhibited a higher overall likelihood of ADEs, with high-risk events predominantly involving the hepatobiliary and cardiovascular systems, such as hypertension associated with VEGF inhibitors and encephalopathy linked to PD-L1 inhibitors. In contrast, although the overall ADE incidence was lower among female patients, the RORs of autoimmune-related toxicities were markedly higher, particularly in the endocrine system (e.g., thyroid dysfunction) and the musculoskeletal/connective tissue system (e.g., arthralgia). These findings are consistent with established epidemiological patterns, as the incidence of several digestive system tumors, including esophageal and liver cancer, is significantly higher in men. Moreover, the lifetime risk of gastric cancer in men is nearly twice that of women, and this disparity has been linked to higher rates of central obesity, smoking, heavy alcohol consumption, metabolic syndrome, and fatty liver disease in male populations.46,47 Consequently, men have greater real-world exposure to ICIs, contributing to a larger proportion of ADE reports. In addition, biological sex differences in immune function further modulate toxicity susceptibility. Women generally exhibit stronger inflammatory immune responses and a higher prevalence of autoimmune diseases, whereas men are more prone to developing digestive system malignancies, which also influences distinct toxicity patterns during ICI treatment.48,49 These sex-related disparities indicate that differences in tumor epidemiology and immune biology are closely linked to variations in real-world ICI exposure and toxicity susceptibility. Accordingly, clinical management should incorporate sex-specific risk profiles, with closer surveillance of blood pressure and hepatobiliary function in male patients, while female patients require targeted monitoring for thyroid dysfunction and musculoskeletal symptoms. Such an approach provides a more individualized and biologically informed framework for optimizing immunotherapy safety.
In our FAERS-based analysis, VEGFR inhibitors represented one of the drug classes with the highest volume of ADE reports, particularly in male patients and in individuals with a body weight between 50–100 kg. This reporting pattern is closely aligned with the real-world therapeutic characteristics of VEGFR inhibitors. As anti-angiogenic “foundation drugs,” VEGFR-targeting agents have been broadly incorporated across multiple lines of therapy for digestive tract malignancies. In gastric and colorectal cancers, bevacizumab is routinely used in first-line treatment, ramucirumab is commonly applied as a second-line anti–VEGFR-2 option, and oral TKIs such as regorafenib, apatinib, fruquintinib, and rivoceranib are widely deployed in later lines.50–52 Their application has further expanded through combination strategies, including ICIs or platinum–fluoropyrimidine chemotherapy, exemplified by perioperative camrelizumab + rivoceranib + SOX regimens that enhance pCR rates in locally advanced disease. 53 These broad indications, multi-line use, and prolonged cumulative exposure collectively contribute to the higher frequency of VEGFR-related ADE reporting. In addition, the particularly high proportion of ADEs among patients weighing 50–100 kg suggests a pharmacokinetic component. Although dosing in this weight range typically relies on fixed or BSA-based regimens, higher body fat percentages and interindividual variability in metabolic enzymes such as CYP3A4 may alter drug clearance and promote drug accumulation,54,55 thereby increasing toxicity risk. These observations indicate that weight—similar to sex, age, and treatment stage—should be regarded as a dynamic, modifiable risk factor, and weight-adapted dosing or monitoring strategies may help optimize the safe use of VEGFR inhibitors. From a toxicity standpoint, VEGFR inhibitors exhibit a typical and readily recognizable adverse reaction profile, which substantially contributes to their prominent ADE signals in pharmacovigilance systems. Previous clinical and real-world evidence has consistently shown that VEGFR-TKIs markedly increase the risk of cardiovascular–renal and vascular toxicities, including hypertension, proteinuria, renal impairment, and bleeding/thrombosis.56,57 Our findings further indicate population-specific manifestations of these toxicities: in sex-based analyses, the risk of alopecia was notably elevated, whereas in age-based analyses, falling emerged as a prominent concern. These observations are mechanistically aligned with excessive VEGF/VEGFR pathway inhibition, which leads to microvascular rarefaction and endothelial dysfunction—changes that raise peripheral vascular resistance, impair the glomerular filtration barrier, reduce blood supply to hair follicles, and diminish tissue oxygenation and muscular stability, thereby predisposing older patients to falls.58,59 In addition, the long clinical history and well-established toxicity spectrum of VEGFR inhibitors enhance clinician awareness and facilitate the attribution of relevant events to drug exposure, thereby increasing the likelihood of ADE reporting. For gastrointestinal malignancies—chronic diseases that often require long-term or maintenance VEGFR inhibitor therapy—cumulative exposure also enables the identification of insidious laboratory abnormalities and chronic organ function decline. 60 Collectively, the widespread use of VEGFR inhibitors in digestive tract cancers, their distinctive toxicity profile, and heightened reporting vigilance jointly account for their high ADE reporting frequency observed in this study.
In summary, this study systematically evaluated the adverse drug event profiles of PD-1, PD-L1, CTLA-4, HER2, EGFR, VEGF, and VEGFR inhibitors in the treatment of digestive system tumors based on the FAERS data from 2004 to 2024. Through disproportionality analyses such as ROR, PRR, and IC, we not only depicted the characteristic safety signals of different targeted drugs at the organ-system and PT levels but also found that male patients and those with a body weight of 50-100 kg had a higher risk of ADEs. Most events were concentrated in the early stage of treatment, suggesting an “early failure” pattern. These results supplement the safety evidence of immunotherapy and targeted therapy from the real-world perspective, supporting the implementation of stratified monitoring and individualized treatment decisions according to characteristics such as gender, age, and body weight in DST management to maximize efficacy while minimizing the risk of toxicity.
The biological heterogeneity of digestive system tumors should also be taken into account when interpreting the variability in adverse-event signals observed across therapeutic classes and patient subgroups. Digestive malignancies are highly heterogeneous at both the intertumoral and intratumoral levels, and such heterogeneity may alter molecular target expression, treatment sensitivity, and toxicity presentation in real-world settings. This is particularly evident in HER2-positive gastric cancer. Satală et al. highlighted the marked heterogeneity of HER2 expression in gastric cancer and suggested that at least 3–4 slides should be evaluated by immunohistochemistry before classifying a tumor as HER2-negative. 61 Consistently, previous studies have reported that intratumoral HER2 heterogeneity is frequently observed in gastric cancer and may influence trastuzumab efficacy, while gastric cancer heterogeneity more broadly may impair responses to HER2-, FGFR-, and EGFR-directed therapies.62,63 Accordingly, some of the differential safety signals identified in our study may be partly attributable to differences in tumor biology and target heterogeneity rather than to drug effects alone. Since FAERS lacks detailed molecular and pathological annotation, we were unable to directly account for this source of heterogeneity, which should be recognized as an important limitation of the present study. Future pharmacovigilance studies integrating molecular profiling and biomarker-resolved clinical data are needed to better clarify the relationship between tumor heterogeneity, treatment response, and adverse-event patterns.
In addition, several limitations of this study should be acknowledged. First, as a spontaneous reporting system, the FAERS database is inherently subject to reporting bias and underreporting. Mild, transient, or clinically manageable ADEs may be less likely to be reported, whereas severe, rare, or highly publicized events are more likely to attract attention and be submitted. Therefore, the observed disproportionality signals, as well as differences in signal rates across drug classes, may have been influenced not only by true safety profiles but also by differential reporting practices, clinical awareness, media attention, and regulatory concern. Second, FAERS lacks reliable denominator data, such as the total number of patients exposed to each drug, treatment duration, and person-time at risk. Consequently, the present analysis cannot be used to estimate the actual incidence, prevalence, or absolute risk of ADEs, and the detected signals should be interpreted as statistical associations rather than evidence of causality. Third, although data cleaning procedures were applied, FAERS reports may still contain duplicate, incomplete, inaccurate, or inconsistently coded information. Important clinical details, including disease severity, treatment line, dosage, duration of exposure, comorbidities, and concomitant medications, are often missing or insufficiently recorded, which may affect the robustness of signal detection. Also, the results may also be influenced by confounding by indication and other clinical heterogeneity. Differences in tumor type, disease stage, baseline health status, prior therapies, and coexisting conditions may all affect the reporting patterns of ADEs and complicate comparisons across drugs or drug classes. Therefore, the findings of this study should be interpreted with caution and regarded primarily as hypothesis-generating. Future research should validate these signals using prospective multicenter cohorts, electronic health records, or claims-based pharmacoepidemiologic studies with more complete clinical information and denominator data. Further analyses stratified by tumor subtype, treatment regimen, and patient characteristics would also help to better clarify the safety profile of immune checkpoint and targeted inhibitors in digestive system tumors.
5. Conclusion
Using the FAERS database, this study systematically characterized the adverse-event spectrum of immune checkpoint and targeted inhibitors in patients with digestive system tumors, identified potential safety signals, and revealed subgroup-specific risk patterns and time-to-onset characteristics. These findings provide real-world evidence to support clinical risk assessment, early detection of adverse events, and more rational and individualized treatment strategies in DST.
Supplemental material
Supplemental material - Real-world pharmacovigilance of adverse events associated with immune checkpoint and targeted inhibitors in digestive system tumors: A FAERS database study
Supplemental material for Real-world pharmacovigilance of adverse events associated with immune checkpoint and targeted inhibitors in digestive system tumors: A FAERS database study by Yinling Li, Zongsheng Sun, Hui Ma, Yuan Gao, Jilin Hu and Longbo Zheng in Science Progress.
Supplemental material
Supplemental material - Real-world pharmacovigilance of adverse events associated with immune checkpoint and targeted inhibitors in digestive system tumors: A FAERS database study
Supplemental material for Real-world pharmacovigilance of adverse events associated with immune checkpoint and targeted inhibitors in digestive system tumors: A FAERS database study by Yinling Li, Zongsheng Sun, Hui Ma, Yuan Gao, Jilin Hu and Longbo Zheng in Science Progress.
Supplemental material
Supplemental material - Real-world pharmacovigilance of adverse events associated with immune checkpoint and targeted inhibitors in digestive system tumors: A FAERS database study
Supplemental material for Real-world pharmacovigilance of adverse events associated with immune checkpoint and targeted inhibitors in digestive system tumors: A FAERS database study by Yinling Li, Zongsheng Sun, Hui Ma, Yuan Gao, Jilin Hu and Longbo Zheng in Science Progress.
Footnotes
Acknowledgments
We wish to cordially thank all medical gastrointestinal surgeons, office staff and nurse practitioners from the two centers for their support and cooperation. Conducting this study project would have been impossible without them.
Author contributions
YLL & ZSS: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Validation, Writing – original draft. HM: Data curation, Investigation, Methodology, Validation, Writing – review & editing. YG: Data curation, Software, Validation, Writing – review & editing. JLH: Data curation, Validation, Writing – review & editing. LBZ: Data curation, Investigation, Methodology, Validation, Writing – review & editing. All authors have read and agreed to the published version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data of this study were used under license for the current study, and were publicly available by the FAERS database.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.