
Abstract
Objective
To investigate the association between different classes of hypoglycemic agents and the occurrence of contrast-induced acute kidney injury (CIAKI) in patients with type 2 diabetes mellitus (T2DM) undergoing coronary angiography (CAG) or percutaneous coronary intervention (PCI).
Methods
This retrospective cohort study included 2082 patients with T2DM who underwent CAG or PCI at two tertiary hospitals between January 2020 and December 2022. Patients were categorized into CIAKI and non-CIAKI groups, and baseline characteristics and short-term in-hospital outcomes were compared. The effects of sodium–glucose cotransporter-2 inhibitors (SGLT2i) use and other classes of glucose-lowering agents on the incidence of CIAKI were evaluated. Multivariable logistic regression analysis was performed to identify factors associated with the occurrence of CIAKI. Propensity score matching was further applied to assess the associations between different glucose-lowering agents and CIAKI as well as adverse cardiovascular outcomes.
Results
The incidence of CIAKI was 11.7% (244/2082). Patients with CIAKI had significantly worse short-term in-hospital outcomes. In multivariable logistic regression analysis, SGLT2i use (OR = 1.892, P = 0.040), total cholesterol (OR = 1.494, P = 0.002), elevated blood urea nitrogen (OR = 1.082, P = 0.022), and diuretic use (OR = 3.389, P < 0.001) were associated with an increased risk of CIAKI. After propensity score matching, SGLT2i use remained associated with a higher incidence of CIAKI (OR = 2.384, P = 0.003), DPP4 inhibitor use was associated with a lower observed incidence of CIAKI (OR = 0.179, P = 0.027). In contrast, no statistically significant associations were observed for other glucose-lowering agents with respect to CIAKI or overall adverse cardiovascular outcomes.
Conclusions
SGLT2i use may be associated with a higher incidence of CIAKI in patients with T2DM undergoing CAG or PCI. These findings may aid risk stratification and clinical management. Further research is needed to clarify the underlying mechanisms.
Keywords
Introduction
Contrast-induced acute kidney injury (CIAKI) is a common complication following intravascular administration of iodinated contrast media, particularly in patients undergoing coronary angiography (CAG) or percutaneous coronary intervention (PCI). 1 With the widespread use of these procedures, CIAKI has become an important cause of hospital-acquired acute kidney injury.2,3 The pathogenesis of CIAKI is multifactorial and may involve renal medullary hypoxia, oxidative stress, endothelial dysfunction, and direct tubular toxicity.4,5 Although the incidence in the general population is relatively low, it may reach up to 30% in high-risk patients and is associated with prolonged hospitalization, increased cardiovascular complications, and higher mortality. 6 Currently, preventive strategies remain the main approach for management. 7
Type 2 diabetes mellitus (T2DM) is a well-recognized risk factor for CIAKI.8,9 Patients with diabetes frequently have concomitant cardiovascular disease and therefore commonly undergo CAG or PCI. In addition to traditional risk factors such as impaired renal function and contrast volume, increasing attention has been paid to the potential influence of antidiabetic medications on susceptibility to CIAKI.10,11
Different classes of hypoglycemic agents exert diverse effects beyond glycemic control, including modulation of renal hemodynamics, inflammation, oxidative stress, and tubular metabolism, which may affect the risk of kidney injury after contrast exposure.12,13 In particular, sodium–glucose cotransporter-2 inhibitors (SGLT2i) have attracted considerable interest because of their established cardiovascular and renal protective effects.14–16 However, their acute hemodynamic effects have raised concerns regarding a possible association with acute kidney injury, and existing studies have reported conflicting findings. 17
Despite these observations, few studies have systematically compared the associations between different classes of hypoglycemic agents and the risk of CIAKI in patients with T2DM undergoing CAG or PCI. Therefore, this study aimed to investigate the clinical characteristics of CIAKI and evaluate the relationship between commonly used hypoglycemic agents and the occurrence of CIAKI in this population.
Methods
Study design and population
This retrospective observational study consecutively screened patients with T2DM who were hospitalized in the Department of Cardiology and the Cardiac Critical Care Unit (CCU) of Nanjing First Hospital and Sir Run Run Hospital, Nanjing Medical University, and underwent CAG or PCI between January 2020 and December 2022. The inclusion criteria were as follows: (1) hospitalized patients with T2DM who underwent CAG or PCI; (2) age ≥18 years; and (3) availability of complete perioperative clinical data. The exclusion criteria were: (1) preoperative acute kidney injury; (2) chronic kidney disease stage 5 requiring long-term dialysis; (3) other identifiable causes of acute kidney injury, including the use of potentially nephrotoxic medications; and (4) repeated exposure to iodinated contrast media during the same hospitalization. This study was conducted in accordance with the Declaration of Helsinki (1975, as revised in 2024). All patient data were de-identified prior to analysis.
Assessment of hypoglycemic medication use
Information on antidiabetic medication use was obtained from the hospital medication record system. Patients were classified as users of a specific hypoglycemic agent if the medication had been prescribed and used for at least 24 hours before CAG/PCI and continued for at least 3 days after the procedure. Patients who did not meet these criteria were classified as non-users of that medication. The hypoglycemic agents evaluated in this study included SGLT2i, metformin, dipeptidyl peptidase-4 inhibitors (DPP4i), glucagon-like peptide-1 receptor agonists (GLP-1 RAs), α-glucosidase inhibitors, sulfonylureas, and glinides.
Data collection
Clinical data were obtained from the electronic medical record systems of the two participating hospitals. Collected variables included demographic characteristics, medical history and comorbidities, perioperative laboratory parameters, contrast medium-related variables, and perioperative medication use (including angiotensin-converting enzyme inhibitor (ACEI), angiotensin II receptor blocker (ARB), calcium channel blocker (CCB), β-blockers, diuretics, insulin, and different classes of antidiabetic medications such as metformin, SGLT2i, DPP4i, α-glucosidase inhibitors, GLP-1 RAs, sulfonylureas, glinides.
Clinical endpoints and definitions
The primary outcome was the occurrence of CIAKI, which was defined according to the 2012 European Society of Urogenital Radiology (ESUR) criteria as an increase in serum creatinine of more than 25% of the baseline value or 44 μmol/L (0.5 mg/dl) within 72 hours of contrast exposure, and excluding other factors that could have contributed to AKI.18,19 Baseline serum creatinine was defined as the lowest value measured after hospital admission and prior to CAG/PCI. Secondary outcomes included dialysis during hospitalization, death, cardiovascular and cerebrovascular adverse events (aggravation of heart failure, myocardial injury, cerebral infarction), and length of hospitalization.
Coronary artery disease was defined as the presence of at least one coronary artery with >50% stenosis. 20 CAG was performed via the radial or femoral artery, and PCI was undertaken by balloon dilatation and/or stent implantation. The type of stent used was selected by the treating physician according to the patient’s clinical condition. T2DM was diagnosed according to the criteria of the American Diabetes Association. 21 Chronic kidney disease (CKD) was defined as an estimated glomerular filtration rate (eGFR) <60 mL/min/1.73 m2 persisting for at least 3 months. 22 Positive urine protein and urine occult blood were defined as ≥1+ on routine urine dipstick urinalysis. Other comorbidities, including old myocardial infarction, hypertension, and chronic obstructive pulmonary disease (COPD), were defined according to established diagnostic criteria or documented diagnoses in the electronic medical record system.
Statistical analysis
Patients were categorized into the CIAKI and non-CIAKI groups according to the occurrence of CIAKI, and baseline characteristics were compared between groups. Continuous variables were tested for normality using the Kolmogorov–Smirnov test. Normally distributed variables are presented as mean ± standard deviation and were compared using the unpaired Student’s t-test, whereas non-normally distributed variables are expressed as median (interquartile range, IQR) and compared using the Mann–Whitney U test. Categorical variables are presented as frequencies and percentages and were compared using the chi-square test or Fisher’s exact test, as appropriate.
Multivariable logistic regression with a backward stepwise method was performed to identify potential risk factors associated with CIAKI. Candidate variables were selected based on clinical relevance and prior literature, as well as variables showing potential association in univariable analyses. The model adjusted for COPD, positive urine protein, albumin, hemoglobin, total cholesterol, triglycerides, preoperative glucose, preoperative blood urea nitrogen, D-dimer, LVEF, use of calcium channel blockers, diuretics, ACEI, SGLT2i, and DPP4i. Multicollinearity was assessed using variance inflation factors (VIFs), and all VIF values were <1.5.
To reduce potential confounding bias, propensity score matching (PSM) was performed using 1:1 nearest-neighbor matching without replacement, with a caliper width of 0.1 of the standard deviation of the logit of the propensity score. Propensity scores were estimated using a logistic regression model incorporating baseline demographic characteristics, comorbidities, laboratory parameters, procedure-related variables, cardiovascular medications, as well as the concurrent use of other classes of glucose-lowering agents. The same set of covariates was applied across all drug-specific PSM analyses to ensure methodological consistency. Prior to matching, the distribution of propensity scores between groups was visually assessed to evaluate overlap and common support. Covariate balance after matching was assessed using standardized mean differences (SMDs), with values <0.1 indicating adequate balance. In the matched cohort, outcomes between drug users and non-users were compared, and conditional logistic regression was used to estimate the associations between different glucose-lowering agents and CIAKI as well as cardiovascular or cerebrovascular adverse events. All PSM analyses were performed using the same analytic framework to ensure comparability across drug-specific analyses.
As this was a retrospective observational study, no prospective sample size calculation was performed prior to study initiation, and the available sample size was determined by the total number of eligible patients enrolled at the two participating hospitals during the study period. Following completion of the analyses, statistical power was evaluated for each drug-specific propensity score–matched comparison using a two-proportion z-test with a two-sided α of 0.05. For analyses yielding statistically significant results, post-hoc power was calculated based on the observed CIAKI incidence rates and matched sample sizes. For analyses yielding non-significant results, given the recognized limitations of post-hoc power calculations in the context of null findings, the minimum detectable effect size (MDE) was calculated to quantify the ability of each comparison to detect clinically meaningful differences at 80% statistical power.
All statistical analyses were performed using IBM SPSS Statistics (version 27.0; IBM Corp., Armonk, NY, USA) and R software (version 4.3.2; R Foundation for Statistical Computing, Vienna, Austria). Results are presented as odds ratios (ORs) with 95% confidence intervals (CIs). A two-sided P value <0.05 was considered statistically significant.
The reporting of this study conforms to the STROBE guidelines. 23
Results
Baseline characteristics of study population
A total of 2238 patients were screened, and 2082 patients with T2DM undergoing CAG/PCI were ultimately included (Figure 1). The mean age was 65.8 ± 10.8 years, and 1451 patients (69.7%) were male. The overall incidence of CIAKI was 11.7% (n = 244). Baseline characteristics are summarized in Table 1. Compared with the non-CIAKI group, patients who developed CIAKI had higher blood pressure and a greater prevalence of arrhythmia and COPD. Several laboratory markers, including WBC count, lipid parameters, BNP, ST2, Lp-PLA2, and glycemic indices, were also higher in the CIAKI group (all P < 0.05). In terms of medications, ACEI, diuretics, and SGLT2i were more frequently used in the CIAKI group, whereas CCB, DPP4i, and metformin were less commonly used. The incidence of CIAKI among different hypoglycemic agents is shown in Figure 2, with the highest incidence observed in SGLT2i users (15.31%). Patients with CIAKI also experienced worse in-hospital outcomes, including higher rates of dialysis, death, worsening heart failure, and myocardial injury (Table 2). Flowchart of patient selection and study design. Baseline characteristics of patients with and without CIAKI. Abbreviations: CIAKI, contrast-induced acute kidney injury; BMI, body mass index; SBP, systolic blood pressure; DBP, diastolic blood pressure; CKD, chronic kidney disease; COPD, chronic obstructive pulmonary disease; WBC, white blood cell count; RBC, red blood cell count; HDL, high-density lipoprotein cholesterol; LDL, low-density lipoprotein cholesterol; BNP, brain natriuretic peptide; ST2, suppression of tumorigenicity-2; Lp-PLA2, lipoprotein-associated phospholipase A2; NGAL, neutrophil gelatinase-associated lipocalin; LVEF, left ventricular ejection fraction; ACEI, angiotensin-converting enzyme inhibitor; ARB, angiotensin II receptor blocker; CCB, calcium channel blockers; SGLT2i, sodium–glucose cotransporter-2 inhibitors; DPP4i, dipeptidyl peptidase-4 inhibitors. Incidence of CIAKI in patients with different hypoglycemic agents. Comparison of secondary outcomes and postoperative laboratory parameters between patients with and without CIAKI. Abbreviations: CIAKI, contrast-induced acute kidney injury.



Association between SGLT2i use and increased risk of CIAKI in patients with T2DM
Baseline characteristics of SGLT2i users and non-users before and after propensity score matching.

Abbreviations: SGLT2i, sodium–glucose cotransporter-2 inhibitors; SBP, systolic blood pressure; DBP, diastolic blood pressure; ACS, acute coronary syndrome; CKD, chronic kidney disease; WBC, white blood cell count; RBC, red blood cell count; HDL, high-density lipoprotein cholesterol; LDL, low-density lipoprotein cholesterol; ACEI, angiotensin-converting enzyme inhibitors; ARB, angiotensin II receptor blockers; CCB, calcium channel blockers; DPP4i, dipeptidyl peptidase-4 inhibitors.

Distribution of propensity scores before and after propensity score matching (PSM) for SGLT2 inhibitor use.

Standardized mean differences of baseline variables before and after propensity score matching (PSM) for SGLT2 inhibitor use.
Before PSM, the incidence of CIAKI was higher in patients receiving SGLT2i than in those not receiving SGLT2i (15.31% vs. 8.2%). After matching, the incidence remained higher in the SGLT2i group (14.6% vs. 8.4%, P < 0.001) (Figure 5). Conditional logistic regression analysis in the matched cohort showed that SGLT2i use was significantly associated with the occurrence of CIAKI (OR = 2.384, 95% CI: 1.348–4.214, P = 0.003) (Table 4). Consistent findings were observed in the multivariable logistic regression analysis of the entire cohort (OR = 1.892, 95% CI: 1.030–3.474, P = 0.040). In addition, higher total cholesterol (OR = 1.494, 95% CI: 1.166–1.915, P = 0.002), elevated blood urea nitrogen (OR = 1.082, 95% CI: 1.011–1.157, P = 0.022), and the use of diuretics (OR = 3.389, 95% CI: 1.855–6.192, P < 0.001) were also associated with the occurrence of CIAKI (Table 5). Incidence of CIAKI and major adverse cardiovascular and cerebrovascular events (MACCE) in SGLT2i users and non-users after propensity score matching. Association between different hypoglycemic agents and CIAKI based on conditional logistic regression analysis. Abbreviations: CIAKI, contrast-induced acute kidney injury; OR, odds ratio; CI, confidence interval; SGLT2i, sodium–glucose cotransporter-2 inhibitors; DPP4i, dipeptidyl peptidase-4 inhibitors. Multivariable logistic regression analysis of risk factors for CIAKI. Abbreviations: CIAKI, contrast-induced acute kidney injury; OR, odds ratio; CI, confidence interval; SGLT2i, sodium–glucose cotransporter-2 inhibitors.


Subgroup analyses of the association between SGLT2 inhibitor use and CIAKI stratified by CKD status and diabetes duration in the propensity score–matched cohort.
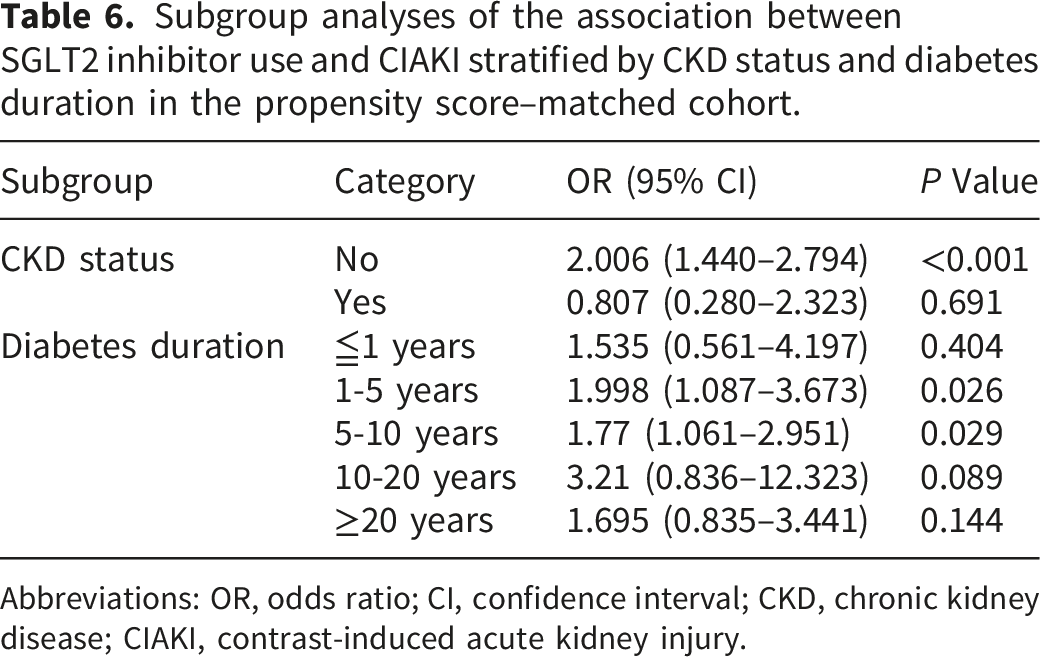
Abbreviations: OR, odds ratio; CI, confidence interval; CKD, chronic kidney disease; CIAKI, contrast-induced acute kidney injury.
Association between SGLT2i use and other outcomes
Association between hypoglycemic agents and major adverse cardiovascular and cerebrovascular events (MACCE) assessed by conditional logistic regression.

Abbreviations: OR, odds ratio; CI, confidence interval; SGLT2i, sodium–glucose cotransporter-2 inhibitors; DPP4i, dipeptidyl peptidase-4 inhibitors; GLP-1 RAs, glucagon-like peptide-1 receptor agonists.
Association between other hypoglycemic agents and CIAKI
Supplemental Tables 1–6 summarize the baseline characteristics of users and non-users of each hypoglycemic agent before and after propensity score matching. Before matching, several clinical and laboratory variables differed between users and non-users across the medication groups. After matching, baseline variables were well balanced between groups, indicating adequate comparability. The distribution of propensity scores and standardized mean differences of baseline covariates before and after matching are shown in Supplemental Figures 1–6. After matching, all standardized mean differences were <0.1, indicating good balance and comparability between groups.
Conditional logistic regression analysis showed that DPP4i use was associated with a lower observed incidence of CIAKI (OR = 0.179, 95% CI: 0.039–0.823, P = 0.027). In contrast, metformin (OR = 0.968, 95% CI: 0.599–1.565, P = 0.895), α-glucosidase inhibitors (OR = 0.737, 95% CI: 0.514–1.057, P = 0.097), sulfonylureas (OR = 1.201, 95% CI: 0.743–1.942, P = 0.456), GLP-1 receptor agonists (OR = 0.560, 95% CI: 0.248–1.265, P = 0.163), and glinides (OR = 1.350, 95% CI: 0.356–5.119, P = 0.659) were not significantly associated with CIAKI (Table 4). In addition, none of these hypoglycemic agents were significantly associated with overall adverse cardiovascular events (Table 7).
Discussion
In this retrospective study of 2,082 patients with T2DM undergoing CAG or PCI, SGLT2 inhibitor use was associated with a higher observed incidence of CIAKI, and this association remained significant after propensity score matching and conditional logistic regression analysis. DPP4 inhibitor use was associated with a lower observed incidence of CIAKI; however, this finding remains exploratory given the relatively small, matched sample size. In contrast, no statistically significant associations were observed between other classes of glucose-lowering agents and CIAKI or short-term adverse outcomes. Overall, these findings suggest that different glucose-lowering therapies may have heterogeneous associations with the risk of CIAKI in patients with diabetes exposed to contrast media.
In the present study, CIAKI was defined according to the ESUR criteria, which have been widely used in studies of contrast-related kidney injury. 18 Compared with the KDIGO criteria, 19 which use a lower threshold for serum creatinine elevation, the ESUR definition may identify a somewhat different spectrum of AKI, particularly with respect to milder cases, which may partly account for differences between our findings and those reported in previous studies.
Recent studies have suggested that short-term exposure to SGLT2 inhibitors may be associated with an increased risk of AKI, particularly in high-risk populations. For example, Zang et al. 24 reported that short-term use of SGLT2 inhibitors was associated with a higher incidence of post-contrast AKI in patients with diabetes. Similarly, Yang et al. 25 found that short-term administration of dapagliflozin was associated with an increased risk of CIAKI in patients with type 2 diabetes and renal insufficiency undergoing PCI. SGLT2 inhibitors may increase susceptibility to AKI under certain clinical conditions.26,27 Mechanistically, these agents inhibit proximal tubular sodium reabsorption, thereby enhancing tubuloglomerular feedback and inducing afferent arteriolar vasoconstriction, which leads to a reduction in intraglomerular pressure. In addition, osmotic diuresis may result in mild volume depletion and reduced renal perfusion. In the setting of contrast exposure, these hemodynamic alterations may exacerbate medullary hypoxia and tubular stress, thereby increasing the risk of acute kidney injury. However, evidence regarding the relationship between SGLT2 inhibitors and CIAKI remains inconsistent. Some studies and meta-analyses have suggested that SGLT2 inhibitors are associated with a reduced risk of AKI in patients with diabetes.28,29 Hua et al. 30 reported that SGLT2 inhibitor use was not associated with an increased risk of CIAKI among patients with CAD and T2DM undergoing PCI (OR = 0.37, 95% CI: 0.19–0.67; P < 0.01), which may be related to differences in patient characteristics and relatively preserved baseline renal function. In addition, previous studies have proposed potential renoprotective mechanisms of SGLT2 inhibitors.31,32 For example, osmotic diuresis and natriuresis may facilitate contrast clearance, thereby reduce tubular contrast concentration and attenuate medullary vasoconstriction. Overall, these discrepancies may be attributable to differences in study populations, baseline renal function, timing and duration of drug exposure, as well as peri-procedural management strategies. In addition, the higher incidence of CIAKI observed among SGLT2 inhibitor users may partly reflect residual differences in patient characteristics and real-world clinical practice patterns. Variations in diabetes severity, cardiovascular comorbidities, renal function, and clinical monitoring intensity may influence both the risk and detection of CIAKI, while differences in peri-procedural medication management may further contribute to the observed associations. Further large-scale prospective studies and randomized controlled trials are warranted to clarify these relationships.
In real-world clinical practice, the selection of glucose-lowering therapy is not random but is influenced by multiple clinical considerations, including renal function, cardiovascular comorbidities, glycemic control, and physician preference. 33 As a result, patients receiving different classes of hypoglycemic agents may have inherently different baseline risk profiles. In our cohort, prescribing patterns were generally consistent with current clinical guidelines. SGLT2 inhibitors are recommended for adults with CKD and an eGFR ≥20 mL/min/1.73 m2 regardless of diabetes status, 34 which may partly explain the differences in CKD prevalence and concomitant ACEI/ARB use between treatment groups before matching. In contrast, DPP4 inhibitors, which are considered safe across a broad range of renal function, were used more widely. In addition, the selection of other glucose-lowering agents is guided by specific clinical contexts, including baseline renal function, cardiovascular risk, glycemic targets, and treatment tolerability. Despite adjustment for measured baseline characteristics using multivariable models and propensity score matching, residual confounding related to treatment selection may still have influenced the observed associations.
With respect to other hypoglycemic agents, we did not observe significant associations between metformin, α-glucosidase inhibitors, sulfonylureas, GLP-1 receptor agonists, or glinides and CIAKI risk. These findings are consistent with previous studies indicating that continuation of metformin around the time of contrast exposure does not increase the risk of CIAKI in patients with preserved renal function.35,36 In our cohort, DPP4i use was associated with a lower observed incidence of CIAKI. Experimental and clinical studies suggest that DPP4 inhibition may exert kidney protective effects through anti-inflammatory, antioxidative, and endothelial-protective mechanisms. 37 However, because the number of CIAKI events among DPP4i users was relatively small, this finding should be considered exploratory and requires confirmation in larger cohorts.
In addition to hypoglycemic therapy, elevated blood urea nitrogen, higher cholesterol levels, and the use of diuretics were also associated with CIAKI in this study. These factors may contribute to renal hypoperfusion, neurohumoral activation, and volume depletion, which are known mechanisms involved in contrast-associated kidney injury.38,39 Importantly, patients who developed CIAKI in our cohort experienced worse short-term clinical outcomes, including higher mortality and a greater incidence of heart failure exacerbation and myocardial injury. In this context, the higher CIAKI incidence observed in certain treatment groups may indicate increased susceptibility to renal injury in the peri-contrast setting and could be associated with a higher risk of subsequent chronic kidney disease progression and worsening cardiac function. These findings underscore the importance of identifying patients at high risk of CIAKI and implementing appropriate preventive strategies.
The present study also has several strengths. It included a cohort of patients with T2DM undergoing CAG or PCI, reflecting real-world clinical practice. In addition, multiple classes of glucose-lowering agents were evaluated within the same population using a consistent analytical framework, including multivariable adjustment and drug-specific propensity score matching. This design allowed for a more comprehensive and internally consistent comparison across commonly used antidiabetic therapies, providing additional insight into potential heterogeneity in CIAKI risk.
Several limitations should be acknowledged. First, due to the retrospective observational design, causal inference cannot be established, and residual confounding related to treatment selection may persist despite multivariable adjustment and propensity score matching. Second, detailed information on medication exposure, including duration, dosage, and precise timing relative to contrast administration, was not consistently available. Third, each hypoglycemic drug class was analyzed separately using drug-specific propensity score matching, which may have resulted in overlapping patient populations across analyses and the absence of a unified reference group. Fourth, the study was conducted in two tertiary centers within a single geographic region and included only adult patients with T2DM, which may limit the generalizability of the findings to other populations, including pediatric patients. Finally, matched sample sizes for several drug classes were relatively small, limiting statistical power, and long-term renal and cardiovascular outcomes were not available. Prospective studies and randomized trials are needed to further clarify the relationship between different hypoglycemic therapies and the risk of CIAKI.
Conclusions
In summary, among patients with T2DM undergoing CAG or PCI, the use of SGLT2i was associated with a higher observed incidence of CIAKI after adjustment for potential confounders, whereas DPP4i use was associated with a lower observed incidence. No statistically significant associations were observed for other glucose-lowering agents, which may be partly attributable to limited statistical power. Overall, these findings suggest potential heterogeneity in the relationship between glucose-lowering therapies and CIAKI risk and warrant further investigation in larger cohorts and prospective studies, including randomized controlled trials.
Supplemental Material
Supplemental material - Hypoglycemic agents and contrast-induced acute kidney injury in type 2 diabetes: A retrospective cohort study of patients undergoing coronary angiography or percutaneous coronary intervention
Supplemental material for Hypoglycemic agents and contrast-induced acute kidney injury in type 2 diabetes: A retrospective cohort study of patients undergoing coronary angiography or percutaneous coronary intervention by Danning Guo, Xia Du, Ting Zhang, Ruihan Liu and Mengqing Ma in Science Progress.
Footnotes
Acknowledgments
We thank all the staff from Sir Run Run Hospital, Nanjing Medical University, and Nanjing First Hospital affiliated with Nanjing Medical University who participated in this study.
Ethical considerations
This study was approved by the Medical Research Ethics Committee of Sir Run Run Hospital, Nanjing Medical University (Nanjing, China; approval number: 2024-SR-023; approval date: April 26, 2024) and the Medical Research Ethics Committee of Nanjing First Hospital, Nanjing Medical University (Nanjing, China; approval number: KY20190704-01; approval date: July 4, 2019).
Consent to participate
The requirement for written informed consent was waived by the institutional review boards due to the retrospective nature of the study.
Author contributions
Mengqing Ma designed the study and performed statistical analyses. Danning Guo and Xia Du conceived the study, interpreted data, and drafted the manuscript. Ting Zhang and Ruihan Liu participated in the design of the study and collected data. All authors revised the manuscript and approved the final version of the manuscript. Danning Guo and Xia Du contributed equally to this work.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the National Natural Science Foundation of China (82500834), the Jiangsu Funding Program for Excellent Postdoctoral (2025ZB004), the Jiangsu Province Traditional Chinese Medicine Science and Technology Development Program (MS2025046).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.