
Abstract
Objective
Fracture nonunion remains a significant clinical challenge. The inhibitory effects of beta-blockers on ADRB2 signaling may interfere with this process and impair fracture repair. However, their overall impact on bone healing remains unclear. We aimed to investigate the association between beta-blocker use and nonunion risk in patients with tibial and femoral fractures.
Methods
This retrospective cohort study utilized real-world data from the TriNetX database. Patients aged 40 or older with tibial and femoral fractures treated with intramedullary nailing between 1992 and 2022 were included. Four cohorts were categorized based on beta-blocker use, and propensity score matching (PSM) was applied to construct balanced matched cohorts. The primary analysis used multivariable Cox proportional hazards models, while multivariable logistic regression was performed as a sensitivity analysis.
Results
In the matched cohort, multivariable Cox regression demonstrated an association between beta-blocker use and increased nonunion risk in tibial fractures (HR = 1.505, 95% CI: 1.177-1.924). Logistic regression sensitivity analysis showed consistent findings (odds ratio [OR] = 1.438, 95% CI: 1.023-2.023). No significant association was observed between beta-blocker use and nonunion risk in femoral fractures. In femoral fractures, nicotine dependence and obesity emerged as stronger risk factors, potentially masking the effects of beta-blockers on fracture healing.
Conclusions
Beta-blocker use was associated with a moderate likelihood of nonunion in tibial fractures, a finding that may relate to its inhibitory effects on angiogenesis. The association was less pronounced in femoral fractures, likely due to the masking effects of nicotine dependence and obesity.
Level of evidence
Level III, Prognostic.
Introduction
The rise in life expectancy has led to an increase in skeletal diseases, such as osteoporosis and age-related fractures.1,2 Despite advances in fracture treatment, approximately 10% to 15% of fractures fail to heal properly, which can result in nonunion. 3 Nonunion presents significant challenges for patients, often requiring multiple surgeries and leading to complications such as long-term bed rest, disability, or even death. Fracture healing is a complex physiological process that involves immune responses, angiogenesis, and bone metabolism regulation, which typically includes the inflammatory phase, proliferative phase, and remodeling phase. 4 During the proliferative phase, angiogenesis plays a vital role by supplying oxygen and nutrients necessary for osteoblast activity and callus formation. 4 Despite extensive research, no clinically available drug has yet been proven to reliably improve fracture healing or reduce the risk of nonunion. 5
The sympathetic nervous system (SNS) has been implicated in regulating bone metabolism. Norepinephrine (NE), released by the SNS, acts on β2-adrenergic receptors (ADRB2) on bone cells, inhibiting osteoblast activity and promoting osteoclast differentiation. 6 Additionally, SNS activation influences RANKL expression, which in turn promotes osteoclast activity and accelerates bone loss. Beta-blockers (e.g., propranolol), which inhibit ADRB2, are commonly prescribed for cardiovascular diseases such as hypertension, heart failure, and coronary artery disease (CAD). 7 Beta-blockers have been shown to improve survival rates in patients with acute myocardial infarction (MI), making them a cornerstone in cardiovascular treatment. Current clinical guidelines recommend their use in MI patients and those with systolic heart failure (HF) to reduce the risk of further cardiovascular events. 8
In recent years, there has been growing interest in the role of the sympathetic nervous system in fracture healing. Beta-blockers may impact bone metabolism and healing processes by inhibiting ADRB2. However, current evidence regarding their effects on fracture healing is conflicting. Some observational studies suggest that beta-blockers could promote bone formation and have protective effects on bone health.9–11 However, the literature remains inconclusive regarding the effects of beta-blockers on fracture healing. Animal studies have indicated that ADRB2 inhibits bone formation in uninjured bone but promotes angiogenesis during fracture healing through the expression of αCGRP and vascular endothelial growth factor (VEGF-A), thereby potentially accelerating fracture repair. 12 On the other hand, beta-blockers can inhibit ADRB2 and suppress angiogenesis, potentially delaying the healing process. In this context, beta-blockers might impair fracture repair by suppressing angiogenesis. These discrepancies in the literature highlight the need for further investigation. A retrospective study by Steffenson et al., using healthcare insurance databases, found a 13% higher incidence of nonunion in patients using beta-blockers. 13 Given this uncertainty, we aimed to explore the association between beta-blocker use and nonunion risk in fracture patients, with a particular focus on tibial and femoral fractures. We leveraged the large-scale TriNetX database (https://trinetx.com/) for a real-world evidence (RWD) analysis of the correlation between beta-blocker use and nonunion in fracture patients, aiming to better understand the potential effects of beta-blockers on fracture healing and bone metabolism.
In this study, we focused on patients aged 40 and above with tibial and femoral fractures between 1992 and 2022. To minimize the influence of surgical treatment variations and fracture complexity, we included patients with closed and open type I/II fractures. Propensity score matching (PSM) was used to adjust for age, gender, diabetes, hypertension, common antihypertensive drugs, and body weight, helping to reduce potential confounding factors. The primary outcome was the incidence of nonunion. The odds ratio (OR), hazard ratio (HR), and Cox regression models were employed to analyze the risk of nonunion in patients with tibial and femoral fractures.
Methods
Data acquisition
Data for this retrospective cohort study were obtained from the TriNetX database, a global federated health research network that aggregates electronic medical records (EMR) from numerous large healthcare organizations. Specifically, the study collected data from the US Collaborative Network, which consists of records from 69 healthcare organizations across the United States. This dataset includes EMR from approximately 68 million patients, encompassing diagnoses, procedures, medications, laboratory data, and genomic information. TriNetX continuously collects and updates data from a broad range of healthcare providers, including hospitals, primary care, and specialty care facilities, representing diverse geographic regions, age groups, and income levels. The data were de-identified in compliance with the HIPAA Privacy Rule (§164.514(b) (1)) using expert-certified methods, ensuring it does not qualify as protected health information (PHI). Given the retrospective, anonymized nature of the data, individual consent to participate was not required. The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 14
Study population
In March 2025, we analyzed a subset of data focusing on patients aged 40 or older with tibial and femoral fractures who underwent treatment with intramedullary nailing (CPT codes 27759 and 27506) between January 1, 1992, and December 31, 2022. The index date (time zero) was the date of surgery. Nonunion was defined by the presence of specific ICD-10 codes occurring between 180 and 720 days post-surgery. To ensure a comprehensive clinical profile and establish temporal precedence, chronic comorbidities and baseline covariates were assessed over a 12-month look-back period prior to the index date. However, active medication exposure, including beta-blocker use, was identified within the one-month period immediately preceding the surgery to ensure patients were active users at the time of the index event. To prevent immortal time bias, the risk set for the Cox proportional hazards model was left-truncated at Day 180 post-surgery, with the observation period ending at Day 720 to focus on the clinically relevant window for nonunion diagnosis. Patients without an event were censored at their last recorded encounter or at the end of the 24-month follow-up period. Healthcare utilization bias was mitigated by matching for total baseline clinical encounters during the PSM process, which was implemented via the TriNetX platform using a logistic regression model. Patients were matched 1:1 using the greedy nearest neighbor algorithm with a caliper of 0.1 to construct balanced matched cohorts for subsequent regression analyses. Missing data were handled using a complete-case strategy. Post-matching balance was verified using standardized mean differences (SMD), with a value below 0.1 considered indicative of successful balance. To evaluate the association between beta-blocker exposure and bone healing outcomes, four cohorts were created based on the use or non-use of beta-blockers. Specifically, patients who had used beta-blockers more than twice in the month prior to surgery were compared with those who had not used beta-blockers. Fractures were classified as either closed and open (Type I and II) tibial and femoral shaft fractures. Only patients who underwent fixation with intramedullary (IM) nails were included in the study. The inclusion criteria were as follows: closed fractures, open Type I and II fractures, and fixation with IM nails. Type III open fractures were not included as part of the inclusion criteria, while pathological fractures were excluded to minimize the confounding effects associated with surgical complexity and fracture severity. Figure 1 showed the study flowchart, where Cohort 1 was matched with Cohort 2, and Cohort 3 was matched with Cohort 4. Cohort 1 consisted of patients with tibial closed fractures and Type I and II open fractures treated with IM nails and Beta-blocker use. Cohort 2 included patients with tibial closed fractures and Type I and II open fractures treated with IM nails without Beta-blocker use. Cohort 3 involved patients with femoral closed fractures and Type I and II open fractures treated with IM nails and Beta-blocker use. Finally, Cohort 4 comprised patients with femoral closed fractures and Type I and II open fractures treated with IM nails without Beta-blocker use. The cohort selection and the outcomes of interest were provided in Supplement 1. Study flowchart.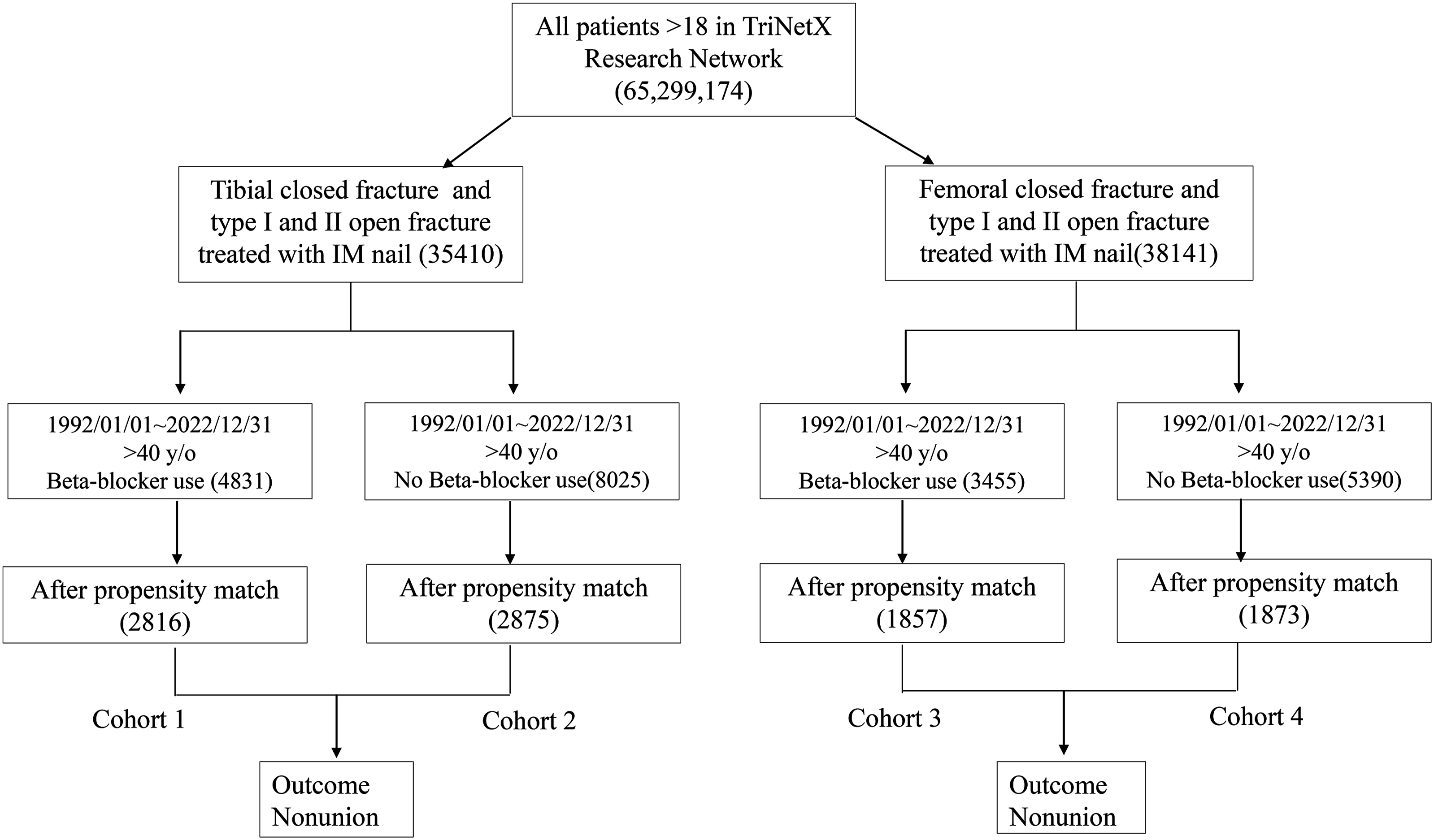
The index events included patients with tibial and femoral fractures identified using the following ICD-10 codes: Closed fracture of shaft of right tibia (S82.201A), Open type I and II fracture of the shaft of the right tibia (S82.201B), Closed fracture of shaft of left tibia (S82.202A),Open fracture of the shaft of the left tibia (S82.202B), Fracture of the shaft of the tibia, unspecified (S82.209A), Open type I and II fracture of the shaft of the tibia, unspecified (S82.209B),Closed and open type I and II fracture of the shaft of the left femur (S72.302A and S72.302B), Closed and open type I and II fracture of the shaft of the femur, unspecified (S72.309A and S72.309B). To minimize the effect of soft tissue injury on bone healing, we only included closed fractures and open type I and II fractures of the tibia and femoral shafts, excluding pathological fractures (tibia: M84.461, M84.462, Femur:M84.451, M84.452).
Statistical analysis
To evaluate the association between beta-blocker exposure and bone healing outcomes across subgroups, propensity score matching was conducted within the TriNetX platform. The matching process was performed to pair cohorts receiving beta-blockers with non-beta-blocker counterparts, considering baseline confounding factors such as age, sex, comorbidities (including diabetes, hypertension, and atherosclerosis), weight, and the use of common cardiovascular medications (e.g., antihypertensives, calcium channel blockers, ACE inhibitors, angiotensin II inhibitors, and alpha-blockers). Additional covariates included race, BMI, nicotine dependence, long-term use of steroids and NSAIDs, systemic connective tissue diseases, hypertensive heart disease, chronic kidney disease, and use of antilipemic agents. Balance between cohorts was assessed using standardized mean differences (SMD), with a threshold of < 0.1 indicating optimal balance. To address potential residual confounding, we performed multivariate regression analysis within the propensity-score matched sample. This approach was intended to address any residual confounding that might remain even after the initial matching process. The propensity score matching procedure was used to construct balanced matched cohorts rather than to directly estimate a marginal treatment effect. Therefore, the reported hazard ratios and odds ratios should be interpreted as model-based adjusted associations within the matched cohorts. Categorical outcomes were assessed using chi-squared tests, while continuous outcomes were evaluated with Mann-Whitney U tests. The differences were reported as hazard ratios and odds ratios, with statistical significance set at p < 0.05.
The primary analysis was the multivariable Cox proportional hazards model, while a multivariable logistic regression was performed as a sensitivity analysis to verify the consistency of the findings. To account for the matched-pair structure generated by 1:1 propensity score matching, all Cox and logistic regression models were fitted using cluster-robust sandwich variance estimators with clustering on matched pairs. This cluster robust variance estimation ensures valid inference by accounting for the within pair correlation inherent in the matched design for both the Cox and logistic regression models. The Cox proportional hazards models were fitted on the matched sample without additional stratification by matched pair, while inference was corrected using cluster-robust sandwich variance estimators. These models adjusted for confounding factors included chronic conditions such as nicotine dependence, diabetes mellitus, obesity, systemic connective tissue disorders, and hypertension, as along with long-term use of steroids, non-steroidal anti-inflammatory drugs (NSAIDs), antilipemic agents, diuretics, calcium channel blockers, ACE inhibitors, and alpha blockers. The outcomes of interest were the occurrence of nonunion in tibial and femoral fractures identified using ICD codes. Univariate tests, such as chi-squared and Mann-Whitney U tests, were used solely for initial descriptive comparisons of the matched cohorts.
Results
Patient cohorts and demographics
Demographics and baseline characteristics of patients with tibial fractures using and not using beta-blockers before and after propensity score matching (PSM).

aStandardized mean difference.
Demographics and baseline characteristics of patients with femoral fractures using and not using beta-blockers before and after propensity score matching (PSM).

aStandardized mean difference.
Risk of nonunion in patients with tibial and femoral fractures
Risk of nonunion in patients with tibial fractures with and without beta-blocker use.

Risk of nonunion in patients with femoral fractures with and without beta-blocker use.

Factors influencing nonunion risk in patients with tibial and femoral fractures
Cox regression analysis of risk factors associated with nonunion in patients with tibial fractures.

Values shown in bold indicate statistically significant (p < 0.05)
Cox regression analysis of risk factors associated with nonunion in patients with femur fractures.

Values shown in bold indicate statistically significant (p < 0.05)
Discussion
This study investigated the association between beta-blocker use and nonunion risk in patients with tibial and femoral fractures while accounting for potential confounding factors. Before propensity score matching (PSM), significant baseline differences were observed between beta-blocker users and non-users, including older age and a higher prevalence of comorbidities. After PSM, these differences were minimized, allowing for a more balanced comparison. The Cox regression analysis for tibial fractures identified overweight and obesity, alpha-blocker use, and hypertension as significant risk factors for nonunion. In our analysis, the univariate HR for tibial nonunion reported in Table 3 was 1.171 (95% CI: 0.836–1.640). However, after adjusting for significant baseline covariates in the multivariable Cox model (Table 5), the HR increased to 1.505 (p=0.001). This divergence suggested that the association between beta-blocker use and nonunion risk becomes statistically evident when confounding factors were controlled. While the relative risk increase was statistically significant, the absolute risk difference was modest, and these findings should be considered hypothesis-generating. The divergence between the univariate and multivariable Cox models in the tibial cohort suggests a masking effect by confounding factors. Prior to propensity score matching, beta-blocker users were significantly older and had a higher prevalence of hypertension and obesity. These baseline imbalances can obscure the independent effect of beta-blockers in a univariate analysis. After multivariable adjustment within the matched cohort, an independent association between beta-blocker use and nonunion became statistically apparent. This resulted in consistent associations between beta-blocker exposure and nonunion risk across both HR and OR models.
In contrast, beta-blocker use in femoral fractures was not significantly associated with nonunion risk (HR = 1.221, p = 0.352). Instead, nicotine dependence (HR = 1.765, p = 0.039) and overweight/obesity (HR = 2.109, p = 0.005) were significant risk factors for nonunion in femoral fractures, suggesting that their dominant influence may have masked any potential effect of beta-blockers. Given their well-documented impact on angiogenesis, microvascular function, and inflammation, these factors likely played a major role in impairing fracture healing, particularly in femoral fractures where vascular supply is more robust.15,16 Despite the fact that the association between beta-blocker use and tibial nonunion reached statistical significance (OR 1.438, p < 0.05; HR 1.505, p = 0.001), the absolute risk difference was 0.9%, and the number needed to harm (NNH) was 111. This indicates that while beta-blocker use is associated with an increased relative risk, the clinical impact on an individual patient level is relatively modest. It is essential to distinguish statistical significance from clinical importance; an NNH of 111 suggests that clinicians should balance the potential minor risk to bone healing against the well-established cardiovascular benefits of beta-blocker therapy. We do not recommend routine discontinuation of these medications based solely on these findings, but rather suggest they be considered part of a comprehensive perioperative risk assessment.
The potential role of beta-blockers in delaying fracture healing may be related to the inhibition of ADRB2 signaling, which has been shown in in vitro and animal studies to be essential for early angiogenesis and osteoblast activity. 12 However, it is important to note that our clinical dataset lacked direct surrogate markers of impaired vascularization or molecular activity. Therefore, while our findings are biologically plausible, the proposed mechanisms remain speculative and should be considered hypothesis-generating frameworks rather than definitive explanations. To better evaluate these associations in a clinically relevant context, it is necessary to consider the demographics of those most affected by both the injury and the medication. Tibial and femoral shaft fractures are primarily caused by high-energy trauma, such as motor vehicle accidents, falls from height, or direct blunt force trauma.17,18 These fractures are more commonly observed in younger individuals, as they are more frequently involved in high-risk activities, including sports, extreme sports, and other scenarios prone to severe trauma. In contrast, beta blockers are primarily prescribed for the management of cardiovascular diseases, such as hypertension, arrhythmias, and coronary artery disease.19,20 Because age is a critical determinant of bone healing capacity and cardiovascular burden, our study specifically focused on patients aged 40 years and older. This targeted selection was implemented to minimize the confounding effects of age-related differences in healing capacity and to isolate the potential impact of beta-blocker therapy within a population where its use is most prevalent.
The observed delay in fracture healing may be linked to the inhibition of ADRB2 signaling. ADRB2 activation on periosteal cells stimulates vascular endothelial growth factor A (VEGF-A) and calcitonin gene-related peptide-α (αCGRP) expression, which are essential for the formation of type-H vessels and bone regeneration. 21 Beta-blockers may impair angiogenesis and subsequent osteoprogenitor cell recruitment, by blocking these pathways, consequently delaying fracture repair. To minimize potential confounders, our study design prioritized clinical consistency by focusing on closed fractures and open type I and II fractures. This selection criterion reduce the variability introduced by soft tissue destruction and surgical technique, ensuring that the observed outcomes primarily reflect secondary bone healing mechanisms rather than mechanical instability or fracture complexity.
The femur has a complex and robust vascular network, including the deep femoral and circumflex arteries, which are critical for fracture healing. However, nicotine-induced vasoconstriction and endothelial dysfunction can severely compromise this blood supply, delaying femoral fracture healing.22,23 In contrast, the tibia has a more limited vascular supply, relying mainly on the nutrient artery and periosteal vessels. 24 While nicotine can still impair blood flow, the tibia may be less dependent on extensive vascularization, making it less susceptible to nicotine’s detrimental effects compared to the femur. Mechanical loading differences between the femur and tibia further contribute to this variation. 25 Given its restricted blood supply, the tibia relies heavily on angiogenesis for both fracture healing and soft tissue repair.26,27 Angiogenesis supports healing by facilitating oxygen and nutrient delivery, resolving inflammation, and remodeling the extracellular matrix.21,28,29 Among the key regulators of this process, the sympathetic nervous system influences vascular remodeling through neurotransmitter interactions with adrenergic receptors, primarily ADRB2, on endothelial cells and pericytes. 21 Unlike the femur, which benefits from well-vascularized muscle groups providing collateral circulation, the tibia has minimal soft tissue coverage and an exposed periosteal surface, limiting its ability to compensate for ischemic conditions. This makes angiogenesis even more critical for tibial fracture healing. Given this vulnerability, the anti-angiogenic effects of beta-blockers, which inhibit ADRB2 activation and suppress vascularization, may disproportionately increase the risk of nonunion in tibial fractures compared to femoral fractures.
Given the tibia’s inherently poor blood supply and dependence on angiogenesis for healing, this suppression of vascular growth may significantly heighten the risk of nonunion. Additionally, obesity is associated with chronic systemic inflammation, which disrupts bone remodeling and impairs osteoblast function. 30 Due to the femur’s larger marrow space, obesity-related inflammatory cytokines may have a greater negative impact on bone marrow stem cells and overall fracture healing in femoral fractures compared to tibial fractures. 31 These differences in vascular supply, mechanical loading, and inflammatory response may explain why beta-blocker use was associated with a higher risk of nonunion in tibial fractures but not in femoral fractures. One possible explanation is that nicotine dependence and obesity exert a stronger influence on femoral fracture healing, potentially overshadowing any impact of beta-blockers. In contrast, tibial fractures appear to be less affected by these confounders, making the association between beta-blocker use and nonunion more detectable in this cohort. These findings highlight the need for further investigation into how beta-blockers influence fracture healing, particularly in bones with inherently poor vascularization such as the tibia. A deeper understanding of these mechanisms could help refine clinical decision-making and optimize patient outcomes.
Limitations
A major limitation of this study was the inherent lack of granular clinical data within the administrative database. Important variables such as specific fracture patterns, the degree of comminution, and the severity of initial soft tissue injury were not available for analysis. Furthermore, although we matched for general procedure codes, specific details regarding fixation techniques and the quality of mechanical reduction could not be evaluated. Other factors that influence bone healing, including the severity of systemic trauma and the use of postoperative adjuvant therapies like bone stimulators or biologics, also remained uncaptured. Despite using extensive PSM to balance systemic comorbidities, residual confounding from local and mechanical factors may still influence the results. These factors could potentially impact the observed association between beta-blocker use and nonunion risk.Furthermore, while we controlled for a wide range of cardiovascular conditions, beta-blocker use may still serve as a surrogate for an underlying cardiovascular disease burden that is not fully captured by ICD codes. The inclusion of data spanning from 1992 to 2022 introduced potential bias from secular trends in surgical techniques and postoperative protocols. Although the majority of our data reflected contemporary clinical practice and TriNetX provided robust coding harmonization, the lack of explicit adjustment for the calendar year of surgery remained a limitation of this study. The definition of beta-blocker exposure in this study lacked granular details including specific dosages and the exact duration of therapy. Most importantly, we could not stratify the analysis by drug selectivity to distinguish between β1 selective and nonselective agents. These different classes of beta blockers may exert varying biological effects on bone metabolism and angiogenesis, but the administrative nature of our database did not allow for such detailed stratification. Furthermore, because postoperative medication adherence could not be reliably tracked, our findings reflect a general association rather than a definitive causal link based on specific dosing regimens. Future research utilizing more detailed pharmacological data is necessary to isolate the specific effects of different beta blocker types on the bone healing process.
Additionally, due to the relatively small sample size of open Type I/II fractures within the matched cohorts, a separate stratified analysis was not performed to maintain statistical robustness. However, open fracture status was included as a covariate in the propensity score matching process to ensure balanced distribution between the two study groups. Consequently, our results should be interpreted with caution and confirmed by future prospective studies that can control for these mechanical, procedural, and pharmacological variables.
Conclusions
This study examined the association between beta-blocker use and nonunion risk in tibial and femoral fractures while accounting for potential confounders. The findings suggested that beta-blockers may be associated with a modestly increased nonunion risk, particularly in tibial fractures. In contrast, their effect on femoral fractures appeared less evident, possibly due to the masking influence of nicotine dependence and obesity, which independently impaired vascularization and delayed bone regeneration. The more pronounced association between beta-blockers and nonunion in tibial fractures may reflect differences in vascular supply, mechanical loading, and bone composition. While the findings reach statistical significance, the clinical impact should be weighed against the cardiovascular benefits of beta-blockers, as indicated by the high number needed to harm (NNH = 111) observed in our cohort. Future research should explore the mechanisms through which beta-blockers influence bone healing using time-dependent analyses, such as competing risk models or longitudinal assessments, to better understand their potential impact on fracture repair.
Supplemental material
Supplemental material - Role of beta-blockers in fracture healing and nonunion risk in tibial and femoral fractures: A retrospective cohort study using real-world data
Supplemental material for Role of beta-blockers in fracture healing and nonunion risk in tibial and femoral fractures: A retrospective cohort study using real-world data by Shao-Hsuan Chang, Siu-Ning Tsang, M.D, Yi-Chih Chen, Yu-Chen Huang, Che-Wei Liu in Science Progress
Footnotes
Acknowledgments
This work was performed at the Department of Orthopaedics, Cathay General Hospital, Taipei, Taiwan. The authors also thank Ms. I-Ming Chang for technical support. The authors used ChatGPT-4o for English language editing and clarity improvement during the preparation of this manuscript. The authors emphasize that these tools were utilized solely for linguistic refinement and not for data analysis or the formulation of scientific conclusions. The final content has been thoroughly reviewed, edited, and verified by all authors, who take full responsibility for the integrity and accuracy of the work.
Ethical considerations
The study was conducted in accordance with the Declaration of Helsinki of 1975, as revised in 2024. This study utilized fully de-identified data from the TriNetX global federated health research network. In accordance with the HIPAA Privacy Rule, all patient-level data are anonymized and do not contain protected health information (PHI). We have consulted with the Institutional Review Board (IRB) of Cathay General Hospital (Taipei, Taiwan), which confirmed that this retrospective analysis of de-identified data qualifies for an IRB exemption.
Consent to participate
Consequently, the requirement for informed consent was waived by the IRB.
Author Contributions
SH Chang and CW Liu contributed to the drafting of the original manuscript and figure preparation. SH Chang and SN Tsang contributed to data collection, study methodology, and statistical analysis. YC Chen, and YC Huang critically reviewed the manuscript and provided important intellectual input. CW Liu contributed to study conceptualization, manuscript review and editing, and overall supervision. All authors reviewed and approved the final manuscript and accepted responsibility for the integrity of the work.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data used in this study were obtained from the TriNetX global federated health research network. Due to the nature of the data and the terms of the data use agreement, the authors are not permitted to share the raw patient-level data publicly. However, researchers with appropriate TriNetX credentials may access the data through the federated network.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.