
Abstract
Objective
Manual goniometry is the standard for hand range of motion assessment but is time-consuming and requires in-person visits. This pilot study aimed to develop an AI-based measurement method and to compare its agreement with manual goniometry in both healthy volunteers and patients.
Methods
In this prospective cross-sectional pilot study (July 2022 to February 2023), an AI-based method was developed using six hand gestures and MediaPipe Hands. Geometric optimization was used for metacarpophalangeal and proximal interphalangeal flexion measurements. For comparison, manual goniometry was performed to evaluate measurement errors. Agreement was evaluated using the intraclass correlation coefficient (ICC) and Bland-Altman analysis.
Results
The study consisted of 25 healthy individuals (50 hands) and 34 patients (68 hands). The mean difference between the AI-based method and manual measurements was 0.4°±8.8°. Geometric optimization reduced the mean absolute error by 13.5° for metacarpophalangeal and proximal interphalangeal flexion measurements and by 3.5 percentage points for Swanson score. Across all parameters, the overall mean absolute error was 5.14°, root mean square error was 7.05°, and normalized RMSE was 8.7%. For the Swanson score, the method demonstrated excellent consistency (ICC: 0.95) with the manual measurements, and Bland-Altman analysis showed a narrower 95% limits of agreement after optimization (-3.5%, 7.7%) compared to the pre-optimized results (-2.4%, 13.2%).
Conclusions
This AI-based method showed acceptable agreement with manual goniometry for most measurements. The Swanson score measurement was clinically acceptable, but thumb movements and proximal interphalangeal flexion require further refinement. The method may serve as a supportive tool for hand function assessment, pending validation in more severe hand impairments and varied environmental conditions.
Introduction
Range of motion (ROM) is a fundamental indicator of hand function and supports clinical decision-making for hand injuries or disorders. 1 Although several assessment methods exist, the optimal approach remains debated. In 1983, Swanson et al. established a standardized measurement system to quantify the deficits in digit flexion-extension and thumb adduction-opposition values. 2 This method has been recommended by the American Medical Association and the Chinese Medical Association for evaluating hand function and impairment.3,4 However, this comprehensive evaluation requires in-person hospital visits and clinician participation, and the manual measurement is time-consuming.5,6
In recent years, measuring ROM from image data has been investigated for assessing hand function, particularly in telemedicine.7,8 Photographs are easy to obtain during clinical examinations and follow-ups, and they enable angle measurement without direct patient-assessor contact, thereby improving hand hygiene and offering clear advantages for remote care. Nevertheless, the hand’s complex anatomy and multiplanar kinematics make manual landmark localization on 2D photographs difficult and time-consuming. 9
Hand pose estimation, an artificial intelligence (AI) technique in computer vision, potentially offers a contactless and automatic solution for predicting joint key point (landmark) localization from images. 10 However, few studies have reported its clinical use for measuring hand ROM. Developing an AI-based method with agreement comparable to manual goniometry is valuable for hand surgery and rehabilitation, as it can streamline hand function assessment while maintaining clinical reliability. Our previous study tested an AI-based hand ROM measurement method using smartphone images and MediaPipe Hands in healthy volunteers with normal ROM, 11 but two key issues remained: (1) flexion measurements at the metacarpophalangeal (MCP) and proximal interphalangeal (PIP) joints were unsatisfactory, likely due to key point occlusion during flexion12–14; and (2) the method had not been tested in patients with limited ROM.
Therefore, we conducted a feasibility-oriented pilot study to optimize this AI-based method according to the Swanson system, and evaluate its agreement in both healthy individuals and patients. We hypothesized that the optimized method would achieve comparable consistency with manual goniometry.
This study presents a standardized AI-based hand ROM measurement method with three novel contributions: Algorithmically, we introduce a monocular pseudo-depth correction strategy that geometrically reconstructs occluded joint coordinates during finger flexion, addressing the inherent depth ambiguity of MediaPipe Hands. Clinically, this study provides the first comparison of such a correction method in a patient cohort with hand impairments and integrates the automated measurements into the Swanson impairment scoring system.
Materials and methods
This prospective, cross-sectional comparison study was conducted in accordance with the Declaration of Helsinki of 1975, as revised in 2024, and was approved by the institutional review board of the First Affiliated Hospital of Sun Yat-sen University (ID: [2021]387, approved on 1 June 2021). All participant details have been de-identified to protect privacy. Images used in this study do not contain any identifying personal information. The reporting of this study conforms to STROBE guidelines. 15
Participant recruitment
From July 2022 to February 2023, we recruited healthy volunteers residing in Guangzhou, China. Patients who met the eligibility criteria were recruited consecutively from those attended the hand surgery outpatient clinic and treated in the First Affiliated Hospital of Sun Yat-sen University. We recorded the participants’ age, gender, body weight, height, hand dominance, and medical history. All participants provided written informed consent to participate and to have their hand images used for research purposes.
The inclusion criteria for the healthy volunteers were: age ≥18 years and normal ROM in both hands, as confirmed using Norkin et al.’s ROM values. 16 The exclusion criteria were: a history of previous injuries, disorders, deformities, or surgery of the upper limbs, which might affect hand ROM; neuromuscular disorders that might affect the hands; confirmed diagnoses of rheumatoid arthritis, degenerative arthritis, gout, etc.17,18; and presence of essential tremor, Parkinson’s disease, or other neurological conditions that affected hand measurement.
The inclusion criteria for the patients were: age ≥18 years; presence of hand ROM limitation caused by previous injuries, disorders, or surgery of the upper limbs and ROM of the affected joint <80% of the contralateral, unaffected site. The exclusion criteria were: persistent posttraumatic or postoperative edema of the upper limb (circumference >20% compared to the unaffected site), which affected measurement; digit amputations or polydactyly, which are not suitable for the hand pose estimation algorithm; essential tremor, Parkinson’s disease, or other neurological conditions that affected hand measurement; an unstable health condition and patients who refused to participate in the study.
Image collection
The study was conducted in a real-world hospital examination room with adequate lighting and a standard green examination sheet background. The experimental setup was shown in Figure 1(a). Participants were seated at a table and placed the tested hand on a support fixture to reduce fatigue and unwanted movement. The forearm was maintained in the supination position with the distal wrist crease aligned to the edge of the fixture for standard hand placement. A smartphone (iPhone 12, Apple Inc., resolution: 1980×1080 pixels) was placed 40 cm above the fixture. The intrinsic calibration of smartphone camera was not performed, as the hand pose estimation algorithm normalizes coordinates internally. A laptop computer was placed in front of the participant to sequentially display the visual instructions for the required hand gestures and provide real-time video feedback of hand motion. Illustration of AI-based method. A: A setup for image collection; B: The 21 key points of hand pose estimation; C: Range of motion parameters acquired from each gesture.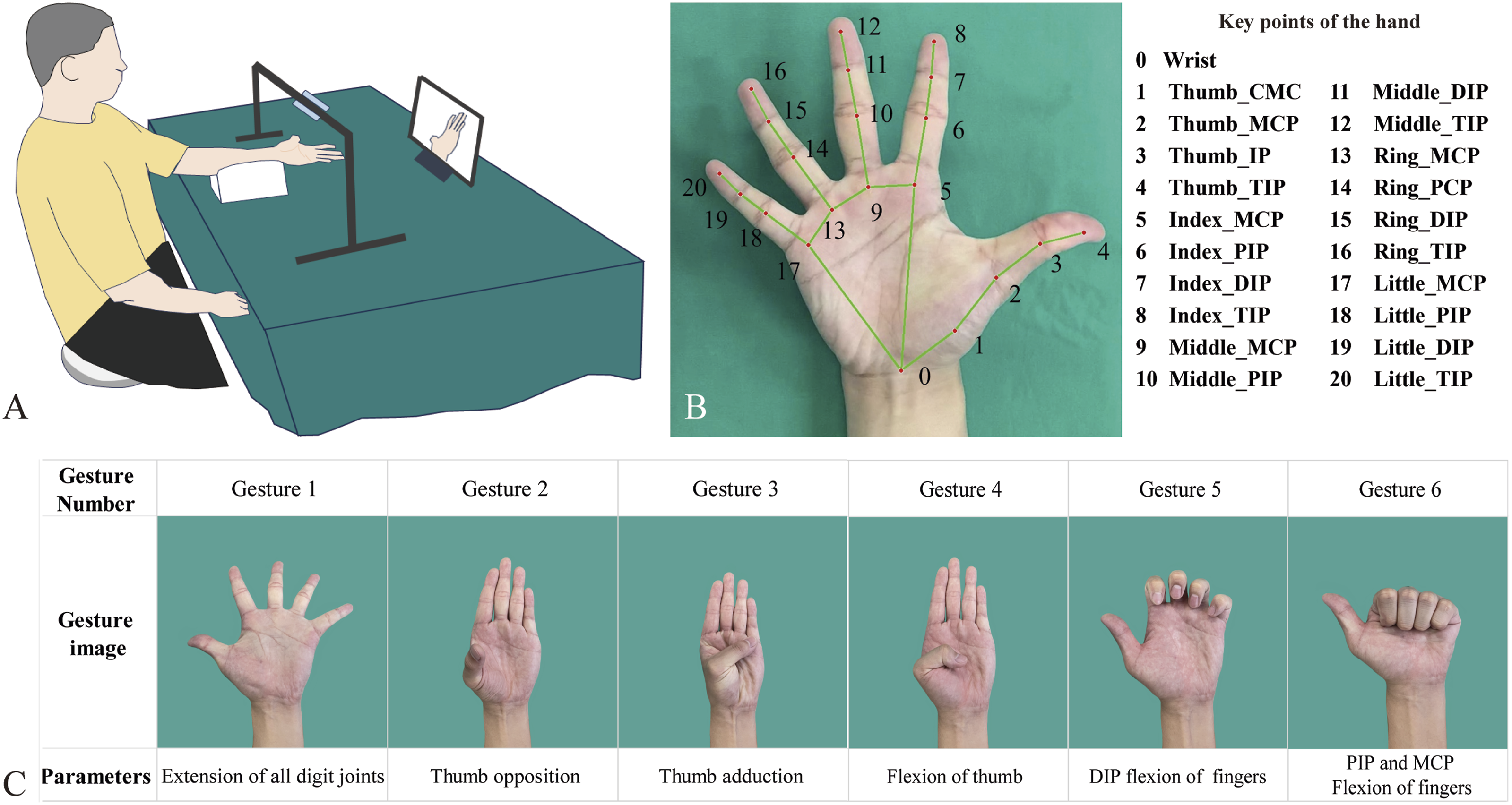
A standardized protocol consisting of six hand gestures was used to guide the participants in carrying out hand motions. The specific ROM values acquired from each gesture were shown in Figure 1(c). Both healthy volunteers and patients were asked to perform the gesture to the maximum of their capability. Three successive photos were captured for each gesture by a senior hand surgeon once the participant confirmed they had fully achieved the motion. For all participants, photos of both hands were captured and analyzed. The participant was allowed to take breaks if there was fatigue or discomfort in the hand.
Automatic ROM measurement
The photos were automatically processed and analyzed using Python (Version 3.8). We used MediaPipe Hands (Version 0.8.9), an open-source hand pose estimation algorithm, to extract 21 key points (Figure 1(b)) with three-dimensional coordinates (x, y, z) from each image.
19
The ROM parameters, including 28 joint angles and 2 distance ratios, were calculated using these coordinates. Joint angles were calculated following our established methodology.
11
To minimize the effects of hand size variability, we employed standardized ratios rather than absolute distance measurement (Figure S1). Detailed calculations were shown in Supplementary Text S1. Three images were obtained for each gesture and the mean value was recorded. In this study, the coronal plane (the palmar plane) was defined by the x-y axes, the sagittal plane was defined by the y-z axes, and the transverse plane was defined by the x-z axes (Figure 2). Processing time was evaluated on a laptop (Intel i7-11800H, 16 GB RAM, NVIDIA RTX 3080). Illustration of MCP and PIP optimization: the relationship between phalanx length, its 2D projection, and its depth value follows the Pythagorean theorem. The phalanx length (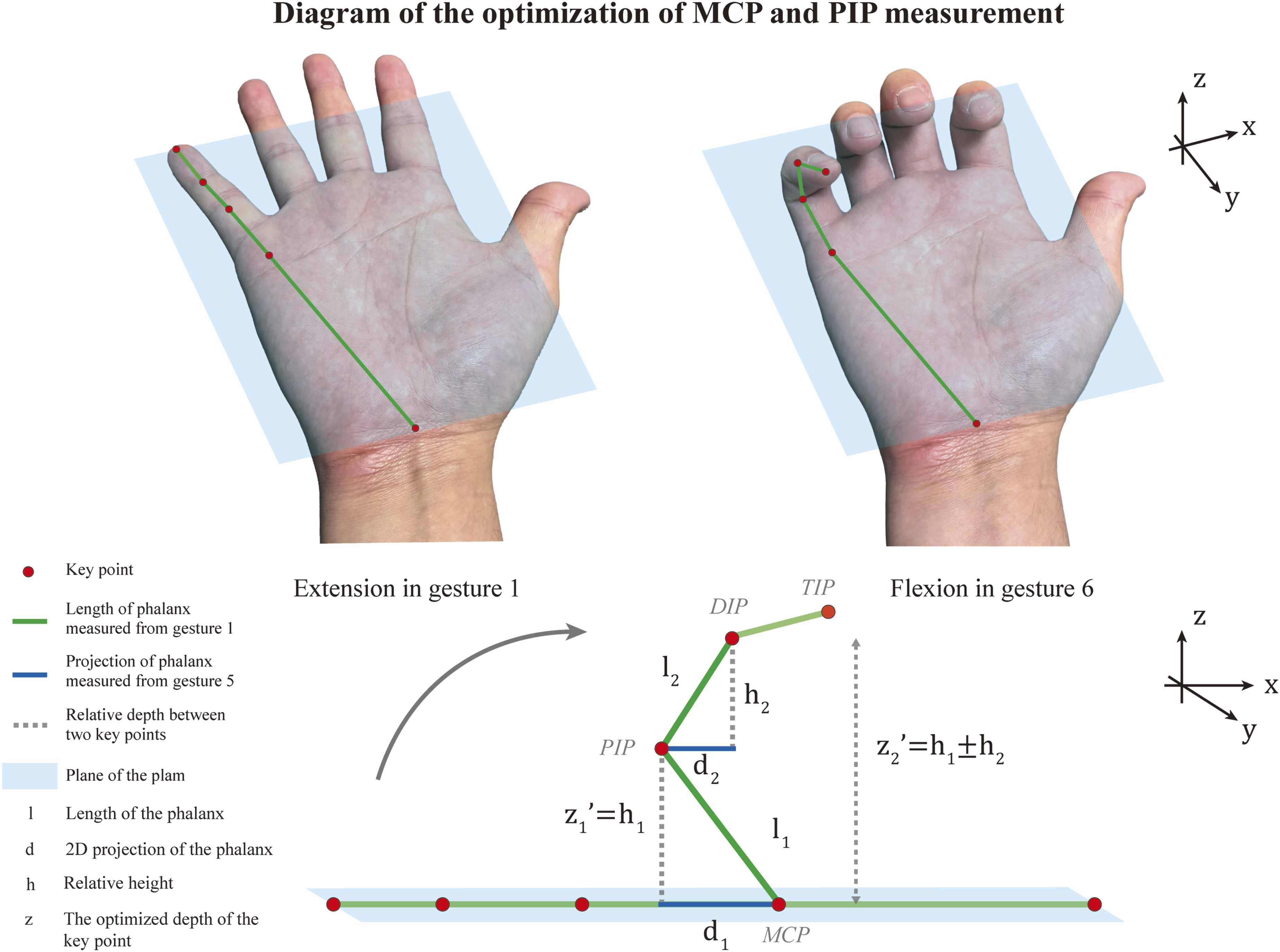
Optimization of MCP and PIP flexion measurement
It is important to note that, according to the official documentation, the z-coordinate represents the landmark depth with the depth at the wrist being the origin. The smaller the value, the closer the landmark is to the camera, and the magnitude of z uses roughly the same scale as x. 19 Consequently, the provided z-values are relative depth values (pseudo-depth) rather than metric depth obtained through stereo camera calibration. The x- and y-coordinates are normalized to the image dimensions. Directly calculating joint angles from these raw coordinates, especially during finger flexion when key points become partially occluded, may therefore introduce errors. To address this inherent limitation, we developed a geometric optimization strategy for MCP and PIP flexion measurements, as illustrated in Figure 2:
In the palmar plane, the relationship between phalanx length (




Swanson evaluation
Following Swanson et al.’s original calculation, 2 thumb impairment was derived by sequentially combining the impairment percentages of the MCP and interphalangeal (IP) joints using Equation (5), where A and B are the impairment percentages of the two joints. The conversion of measurement values to impairment percentage was shown in Table S1. The result was then weighted by 0.2 and added to the opposition and adduction impairment values.
Impairment of each finger was calculated by sequentially combining the impairment percentages of the MCP, PIP, and DIP joints using the same Equation (5), starting with the MCP joint and then adding the PIP and DIP joints stepwise. The values for extension and flexion impairments were first summed at each joint level before performing the combination.
Total hand impairment was then computed as the weighted sum of the thumb and four fingers using Equation (6).


Manual measurement and evaluation
Following image acquisition, manual measurements were performed by another senior hand surgeon using a universal goniometer. Each measurement was repeated three times, and the mean value was recorded in accordance with standardized protocols. 11 To minimize manual calculation errors, the Swanson evaluation score was automatically computed using the same Python analysis procedure applied to the manual measurements. The surgeon was blinded to the AI-based measurement results throughout the process. Measurements were performed in a fixed order (manual followed by AI-based) and were not randomized, as the primary objective was to compare the two methods under controlled conditions.
Statistical analysis
Differences between all AI-based measurements and manual measurements were expressed as mean±standard deviation (SD) with 95% confidence interval (CI). Three complementary error metrics were calculated to quantify the magnitude of measurement error: the mean absolute error (MAE), the root mean square error (RMSE), and the normalized RMSE (NRMSE). MAE was defined as the average of absolute differences between AI-based and manual measurements; RMSE was defined as the square root of the average squared differences. NRMSE was computed as (RMSE/range of manual measurements)×100%, where the range was the difference between the maximum and minimum manual measurement values for each parameter. Paired t-tests were used to compare the MAEs for MCP and PIP optimizations.
Agreement between methods was evaluated using a two-way random-effects intraclass correlation coefficient (ICC) for consistency. ICC values below 0.5 indicate poor reliability, 0.5–0.75 moderate, 0.75–0.9 good, and above 0.9 excellent. 20 Clinical agreement was also evaluated by Bland-Altman plots to assess the validity and describe the 95% limits of agreement (LOA). The threshold of ±5° for joint angles was chosen based on published literature indicating that experienced clinicians can achieve measurement reproducibility within this range under standardized conditions.21,22 The ±10% threshold for Swanson evaluation was derived from the minimum clinically important difference reported in hand impairment studies.2,4 Pearson correlation coefficient was calculated for analyzing linear correlation. 23
To assess whether including both hands from the same participant introduced bias, we performed a cluster bootstrap sensitivity analysis. 24 In each of 500 resamples, we randomly selected one hand per participant and recalculated MAE and RMSE for all parameters (Python, random seed=2026). A parameter was considered robust if the full-dataset value fell within the bootstrap 95% confidence interval (CI).
A significance level of α=0.05 (P<0.05) was applied. Figures 4 and 5 and Figure S2 were generated using the Python Matplotlib library (Version 3.5.2). This was a feasibility-oriented pilot study designed to test whether the AI-based method achieves clinically acceptable agreement with manual goniometry. No a priori sample size calculation was performed, as there were insufficient preliminary data on the expected measurement differences in patient populations.
Results
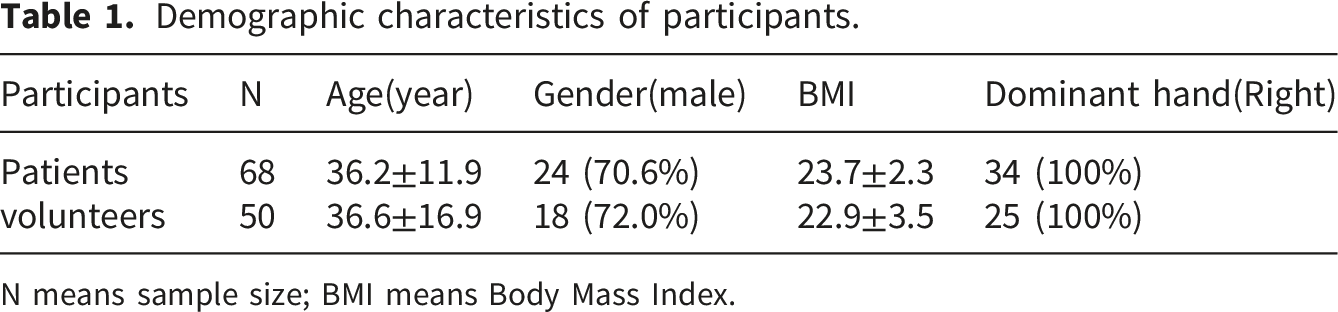
A total of 25 healthy volunteers (50 hands) and 34 patients (68 hands) were recruited in the study. The flow diagram of 59 participants (118 hands) was shown in Figure 3, and the demographic characteristics were summarized in Table 1. Swanson scores of the patient cohort ranged from 7.8% to 61.6% (22.7%±13.4%). The distribution was: 57 hands (83.8%) with mild impairment (0-25%), 9 hands (13.2%) with moderate impairment (26-50%), and 2 hands (2.9%) with severe impairment (51-75%). No hand reached the 76-100% category. A total of 2,124 hand images were processed using the hand pose estimation algorithm and all images were recognized successfully. Total processing times were 3 min 24 sec (GPU) and 3 min 35 sec (CPU). The flowchart of healthy volunteers and patients who participated in this study. Demographic characteristics of participants. N means sample size; BMI means Body Mass Index.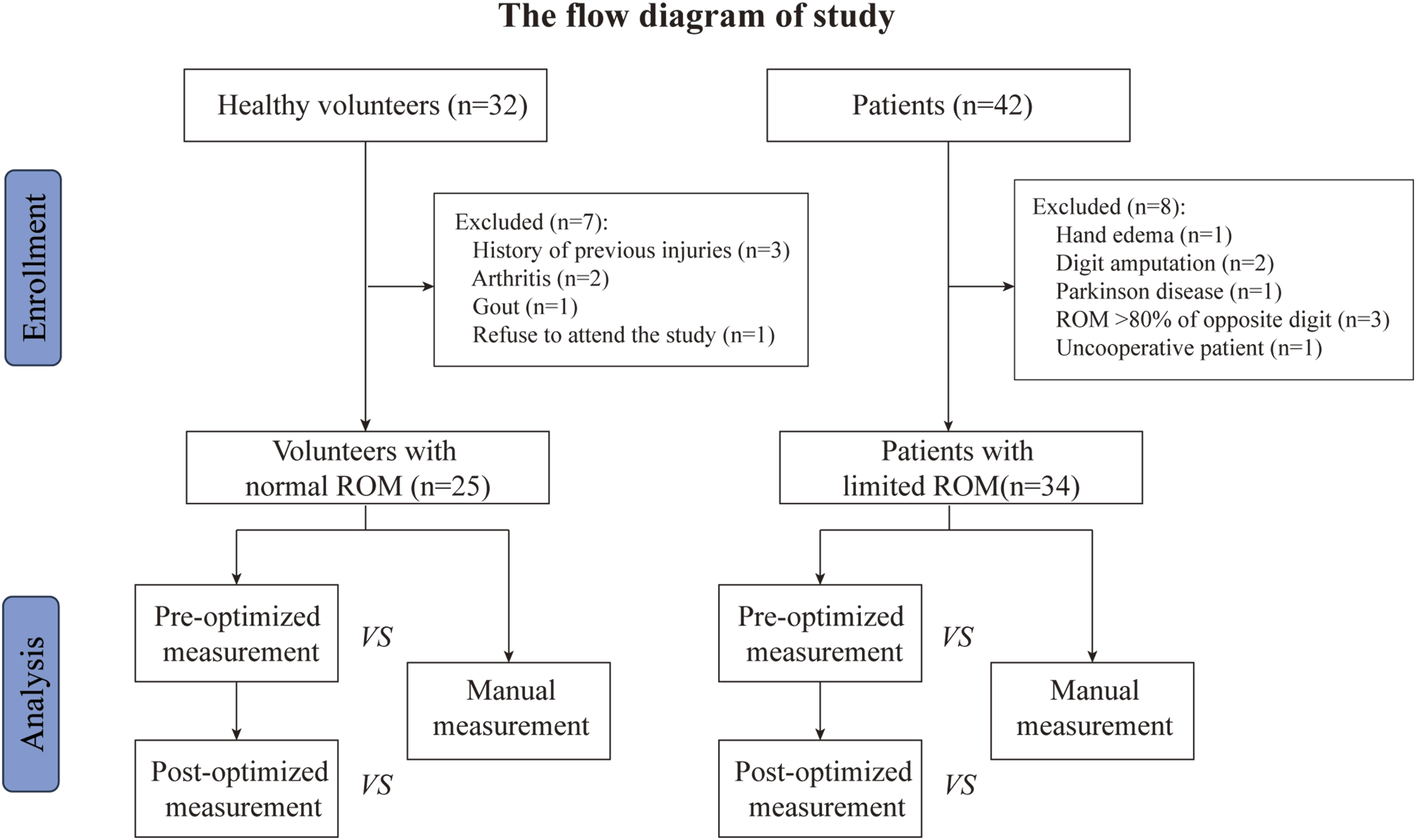
Validity of the AI-based measurement
Comparison of automatic measurement against manual measurement.
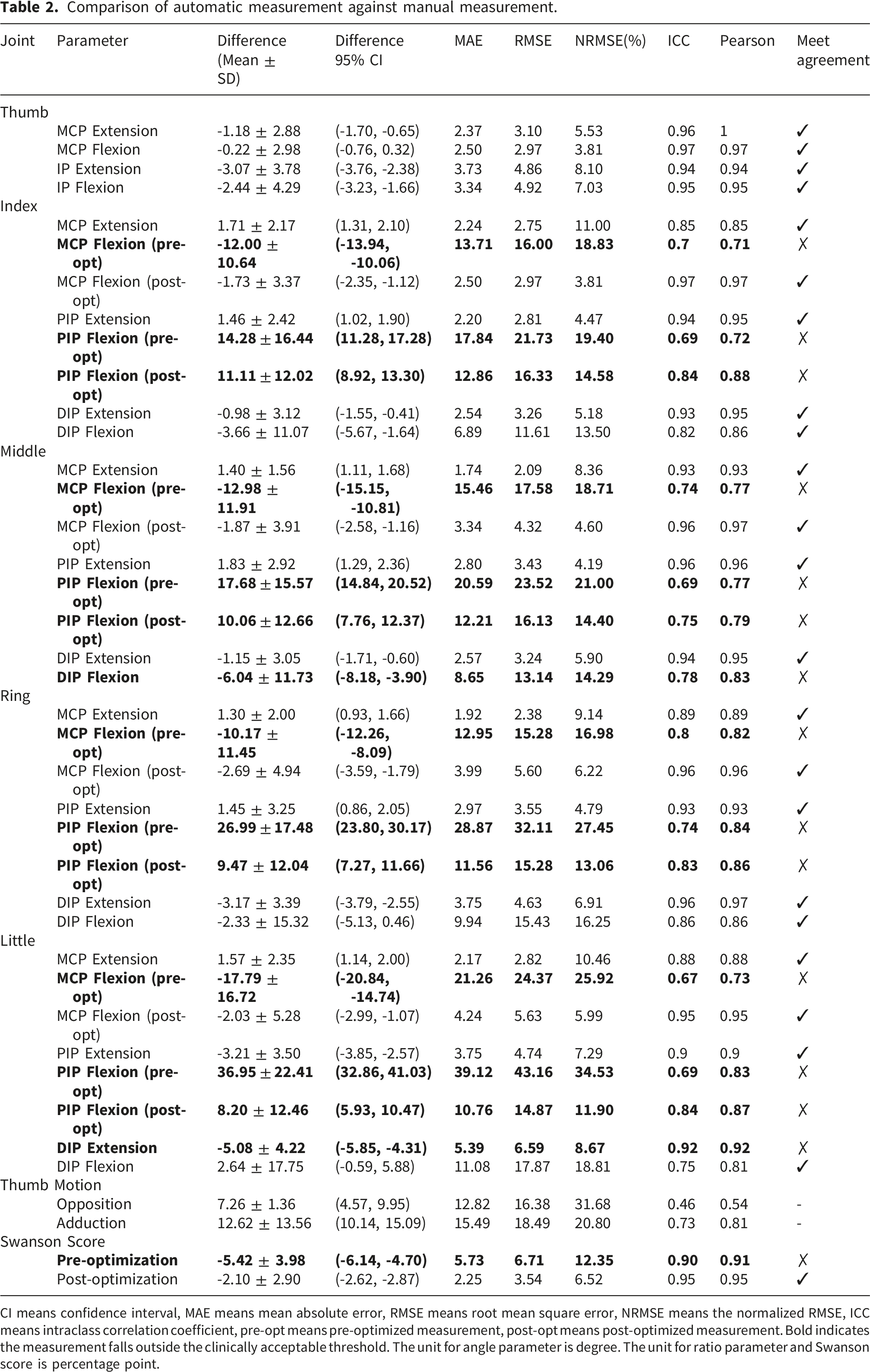
CI means confidence interval, MAE means mean absolute error, RMSE means root mean square error, NRMSE means the normalized RMSE, ICC means intraclass correlation coefficient, pre-opt means pre-optimized measurement, post-opt means post-optimized measurement. Bold indicates the measurement falls outside the clinically acceptable threshold. The unit for angle parameter is degree. The unit for ratio parameter and Swanson score is percentage point.
Paired t-test comparison of MAE between pre- and post-optimization measurements relative to manual goniometry.
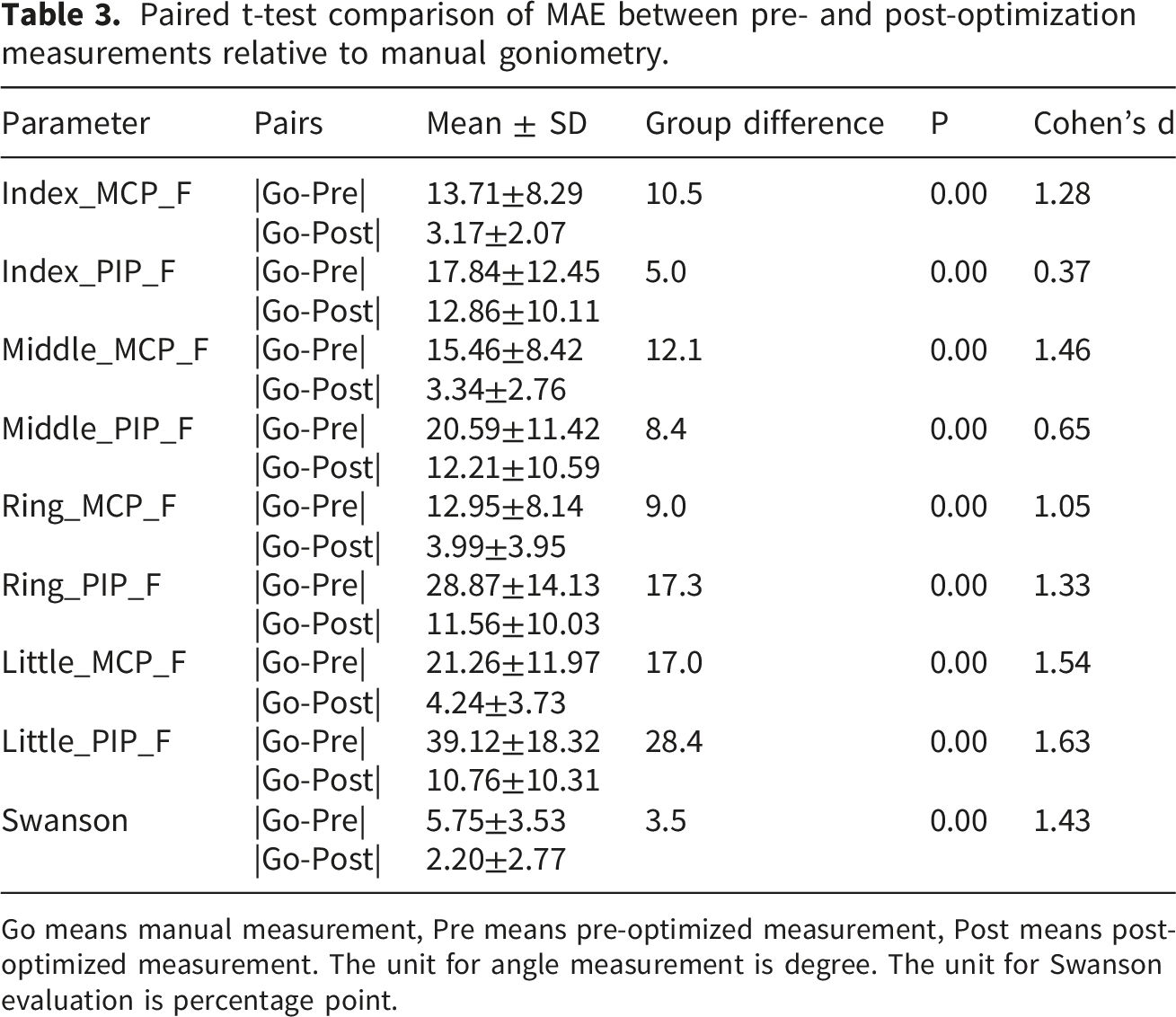
Go means manual measurement, Pre means pre-optimized measurement, Post means post-optimized measurement. The unit for angle measurement is degree. The unit for Swanson evaluation is percentage point.
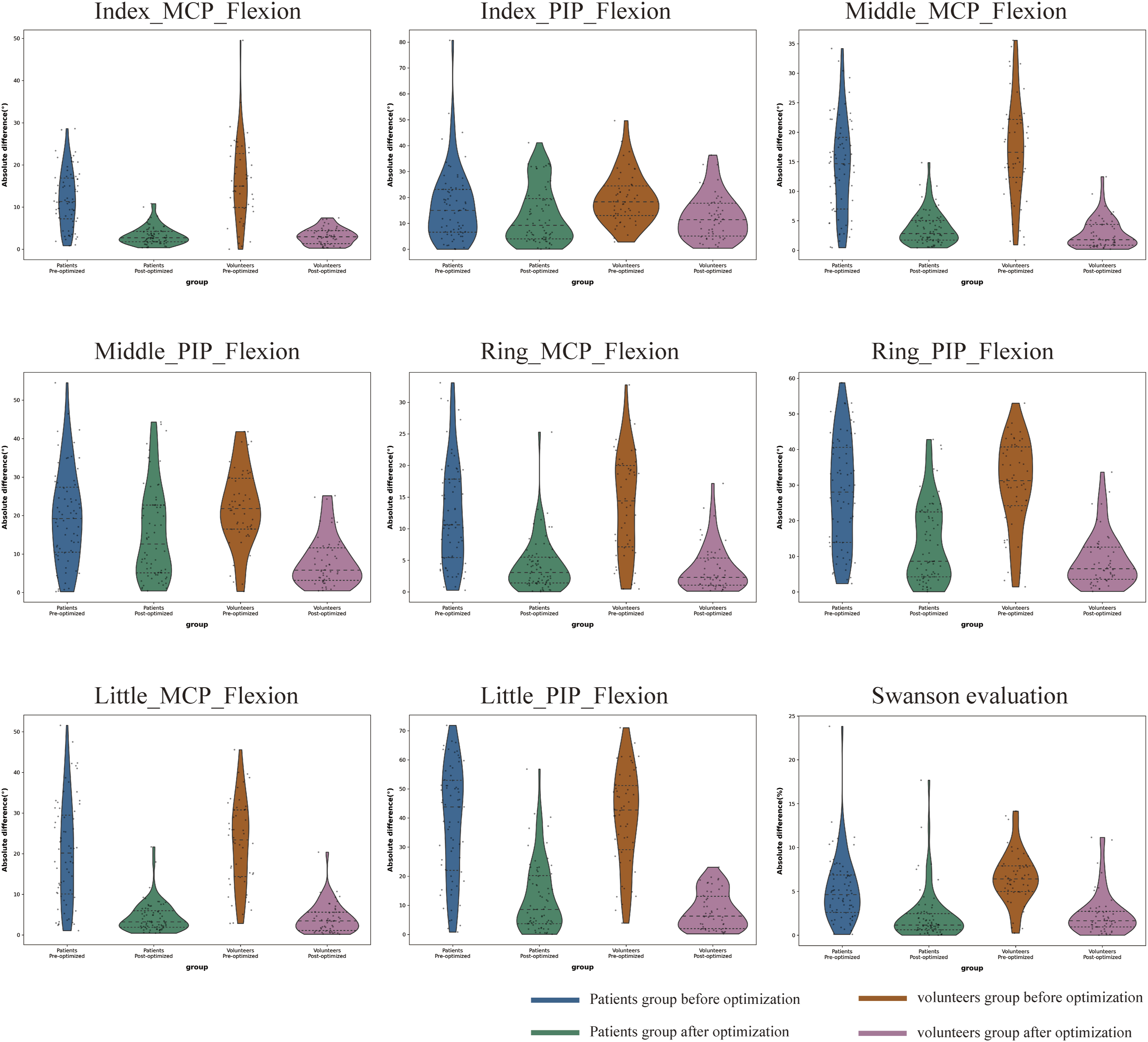
The violin plots demonstrate the distribution of absolute differences of optimized measurements in patients and volunteers.
Absolute difference between patients and healthy volunteers.
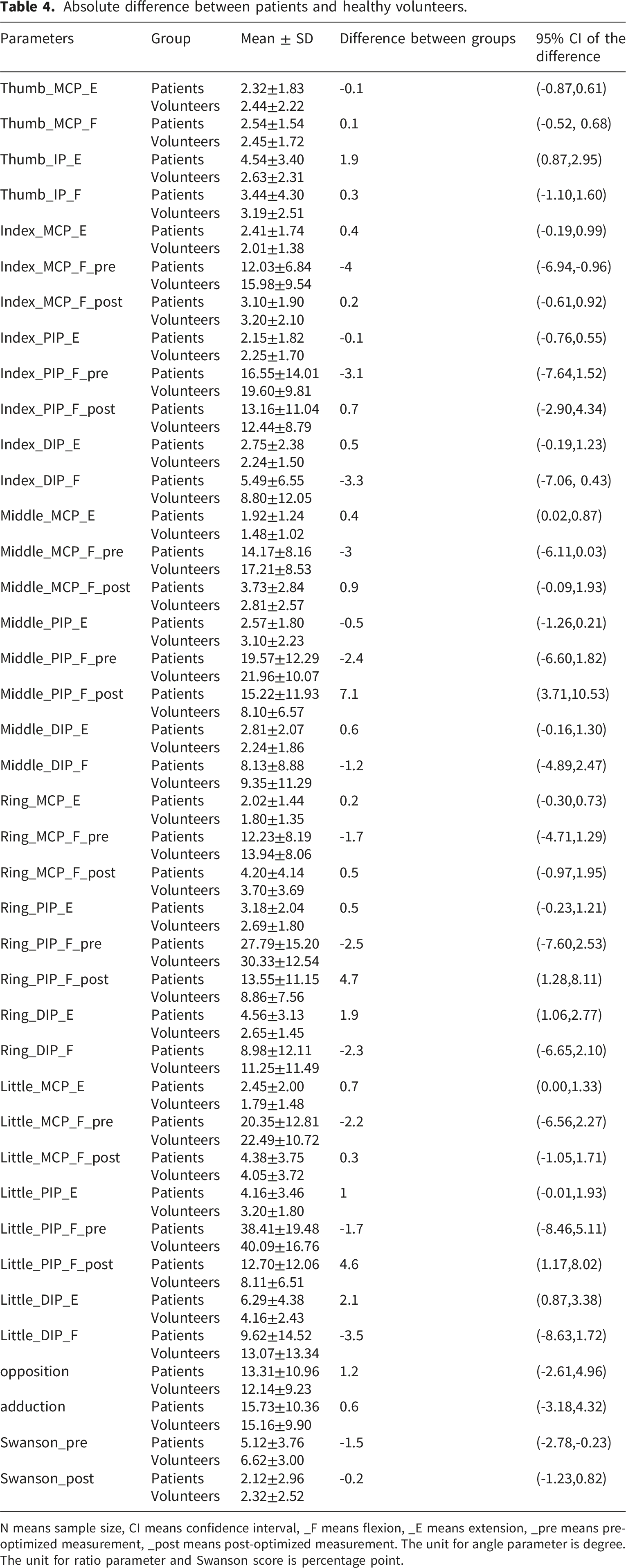
N means sample size, CI means confidence interval, _F means flexion, _E means extension, _pre means pre-optimized measurement, _post means post-optimized measurement. The unit for angle parameter is degree. The unit for ratio parameter and Swanson score is percentage point.
Clinical agreement of the AI-based measurement
In general, 83% of the parameters (25/30) demonstrated excellent consistency with manual measurements after optimization, as indicated by ICC ranging from 0.75 to 0.97 (Table 2). This represented a notable improvement compared with pre-optimization values, which ranged from 0.67 to 0.80. However, two thumb parameters, opposition (ICC: 0.46) and adduction (ICC: 0.73), remained at poor or moderate levels.
Bland-Altman analysis for the Swanson evaluation (Figure 5) further confirmed the impact of optimization. Prior to optimization, the mean difference between AI-based and manual measurements was 5.42%, with 95% LOA ranging from -2.36% to 13.19%. The upper LOA exceeded the predefined clinical acceptance threshold of ±10%, indicating substantial disagreement in a subset of cases. The proportional bias test showed a slope of -0.0956 (p=0.022), indicating significant proportional bias that the discrepancy between methods varied systematically with the level of the Swanson score. After optimization, the mean difference decreased to 2.10% and the 95% LOA narrowed to -3.50% to 7.69%, falling entirely within the ±10% clinical acceptance threshold. The proportional bias test showed a slope of -0.0023 (p=0.938), confirming that the optimized method maintained consistent agreement across the full range of hand impairment severity. Bland-Altman plots for clinical agreement in pre- and post-optimized Swanson evaluation. In each plot, the x-axis represents the mean and the y-axis represents the difference between AI-based and manual methods. The bold black line represents the mean difference, the dotted lines represent the limit of agreement, and the light blue area represents the range of clinical acceptance (±10%).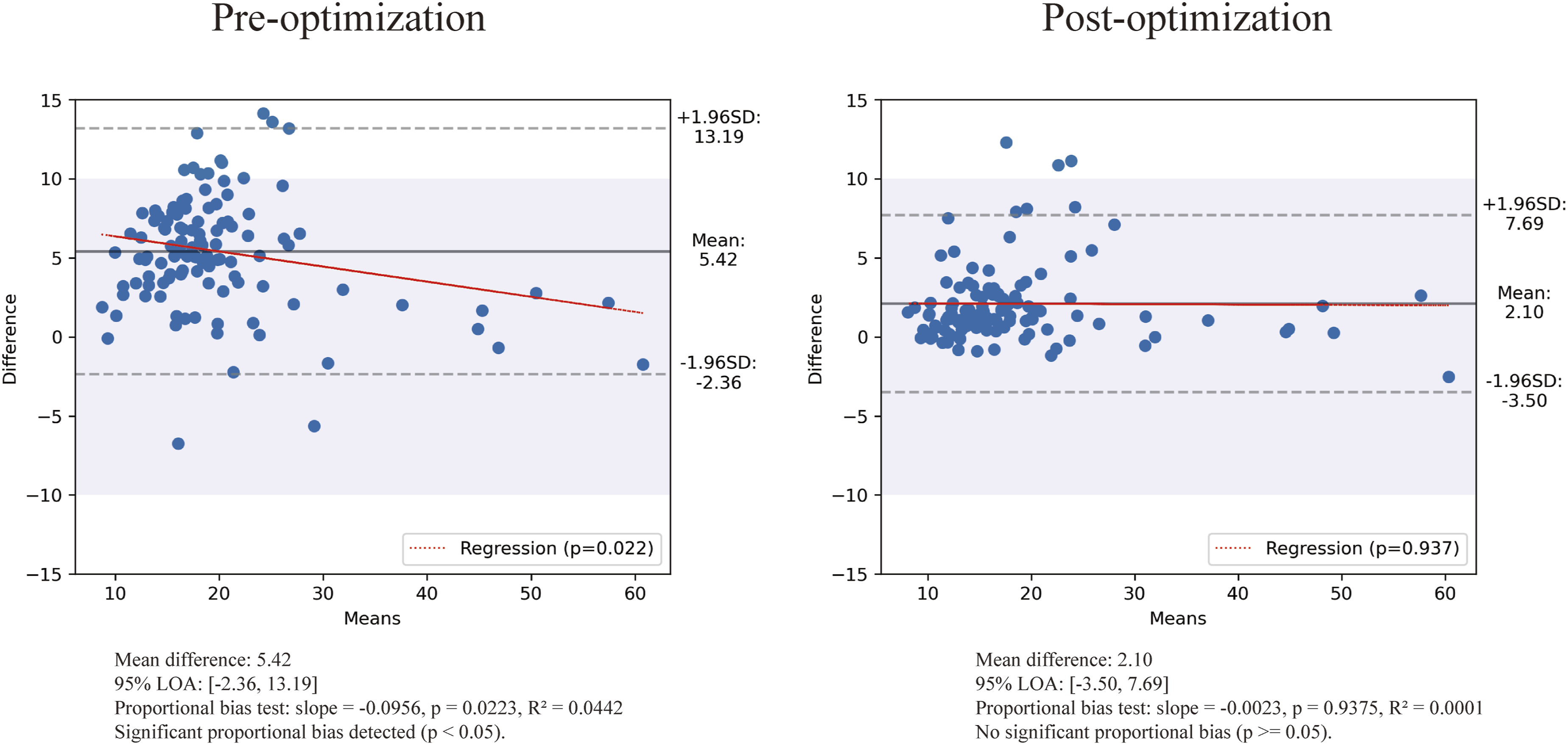
The Pearson correlation coefficient ranged from 0.54-1.00 after optimization, consistent with the improvement observed in ICC values.
In summary, the geometric optimization reduced the discrepancies between AI-based and manual measurements. The Swanson scores fell within the predefined clinically acceptable range (±10%), thereby achieving the objective of this study.
Sensitivity analysis for clustering effect
The bootstrap sensitivity analysis showed that the original full-dataset MAE and RMSE values fell within the 95% bootstrap confidence intervals for all parameters and Swanson score in both pre- and post-optimization phases (Table S3). These results confirm that the potential clustering effect introduced by including both hands from the same participant did not materially bias the results.
Discussion
Clinical comparability with manual measurement
Conventional manual goniometry is a widely accepted standard for clinical ROM measurement. 25 It offers a favorable balance of acceptable agreement, minimal cost, and exceptional clinical practicality. The primary objective of this study was to compare the agreement between the AI-based method and manual goniometry. To minimize inter-rater variability, all manual measurements in this study were performed by a single senior hand surgeon. Given that previous studies have established clinically acceptable intra-rater and test-retest reliability of manual goniometry,9,22 we did not perform formal intra-rater or test-retest reliability analyses. Specifically, Ellis et al. reported that repeated intra-rater goniometric measures fell within 4-5 degrees of each other 95% of the time, while inter-rater measures fell within 7-9 degrees. 22 A margin of error within ±5° is generally considered acceptable even for experienced clinicians under standardized conditions. 23 Moreover, pathophysiological changes and therapeutic interventions can introduce intrinsic measurement error, indicating that variability related to pain, joint laxity, soft-tissue compliance or muscle strength is unavoidable. 26
Importantly, our findings demonstrate clinical comparability, rather than absolute biomechanical accuracy. An optical motion capture system is often considered the gold standard for biomechanical analysis. 27 However, several limitations restrict its use in clinical hand studies. These include time-consuming marker placement, marker occlusion during finger flexion, soft tissue artefact, and the need for expensive, laboratory-bound equipment.28,29 A systematic review of upper limb motion analysis in clinical populations found that optoelectronic systems were predominantly used (57/76 studies) but identified major barriers to clinical adoption, including the lack of standardized reference tasks, protocols, software, funding, and clinical need. 30 Despite the high precision that optoelectronic systems can offer, quantified upper limb motion analysis has not yet been fully integrated into routine clinical care. Therefore, manual goniometry remains the most practical and accessible reference standard for comparing new measurement methods in clinical settings.
In the present study, most joint measurements fell within the ±5° clinical threshold. The improvement in MCP and PIP flexion measurement confirms the feasibility of the depth correction strategy. The residual error in PIP flexion likely results from error accumulation, as its calculation sums the depth values of both MCP and PIP key points (Equation 4). For the Swanson score, the MAE decreased from 5.73% to 2.25% after optimization, a relative improvement of 60.7%. The ICC was 0.95, and the 95% LOA narrowed to -3.5% to 7.7%, falling entirely within the ±10% clinical acceptance threshold. While this absolute change may appear small within the full 0-100% Swanson scale, it is clinically meaningful, as classification near impairment thresholds is essential for patient management and medicolegal reporting. For thumb opposition and adduction, we adapted the Swanson system using standardized ratios validated in large Chinese cohorts 31 to account for hand size variability without relying on absolute image-derived distances. However, agreements for these thumb movements remain only poor and moderate (ICC: 0.46 and 0.73, respectively), likely due to the thumb’s complex and multiplanar kinematics. Thumb opposition requires simultaneous flexion, rotation, and pronation, while adduction involves flexion and rotation. Monocular RGB images suffer from fundamental depth ambiguity and provide limited evidence regarding such motions. Future work may need to develop dedicated thumb-specific motion models to better resolve the thumb’s complex movements without relying solely on monocular vision.
What this study adds beyond prior ROM measurement studies
Image-based goniometry has been a convenient alternative, with studies reporting reliable hand measurements from smartphone images32,33 and high inter-rater reliability in tele-consultations. 9 However, these methods still rely on manual landmark localization. Hand pose estimation has been used for gesture recognition,34–36 yet its application for precise ROM quantification remains underexplored. Previous studies reported large errors during finger flexion.12,13,23,37 For example, Nizamis et al. observed 37°-40° difference in DIP flexion with Leap Motion Controller, 12 and Lv et al. reported 29° bias with a depth camera. 37 Good-to-excellent consistency has been reported in similar studies. A virtual goniometer for the forearm, wrist and finger joints achieved ICC values of 0.69-0.98 38 . Our method achieves lower errors and offers the advantages of being markerless, contactless, and requiring only a smartphone camera.
A fundamental limitation of hand pose estimation is occlusion during flexion. 10 To address this, we employed six standardized palmar-view gestures to maximize key point visibility and isolated the DIP measurement to a dedicated gesture (Gesture 5), to avoid large DIP measurement errors in a fist gesture. 13 More importantly, we applied a geometric correction assuming constant phalangeal length to infer occluded depth coordinates for MCP and PIP flexion. Figure S2 compares the 3D positions of key points for a representative Gesture 6 before and after geometric optimization. Although this substantially improved MCP measurements, the LOA for PIP joints (particularly the little and ring fingers) remained wider than ±5°. This suggests that further refinement may be needed, possibly through multi-view imaging or more sophisticated depth inference algorithms.
Potential for telemedicine, home monitoring, and regulatory pathways
Ideally, an AI-based hand function measurement method should be applicable to telemedicine, home monitoring, and longitudinal follow-up, where repeated in-person assessments are resource-intensive. Recent studies have demonstrated the feasibility of web-based and smartphone-based platforms for remote hand evaluation.6–9,39 The use of a standard smartphone camera and automated post-processing could make the method accessible for remote hand function assessment, which could be particularly valuable for patients in underserved or remote areas. With a processing speed of approximately 10 images per second in CPU mode, the pipeline supports near-real-time feedback, suggesting its potential for integration into rehabilitation apps and home-based self-monitoring. From a regulatory perspective, AI-based ROM measurement tools require clinical validation, performance monitoring, and risk management. While our study represents early-stage technical evaluation, it provides a foundation for future regulatory studies.
However, we must acknowledge that our experimental setup was highly standardized. In real telemedicine conditions, lighting, camera type, background, motion blur, and hand positioning may vary considerably. The robustness of our method under such uncontrolled conditions has not yet been evaluated. Furthermore, the potential influence of soft tissue and skin motion artefact may cause discrepancies during high flexion, oedema, or complex thumb movements. 28 Addressing these challenges will be essential for successful translation of the method into routine telemedicine practice.
Strengths and limitations
Unlike traditional goniometry, which requires repeated measurements per joint, our method achieves comparable agreement using only six standardized gesture images, thereby reducing clinician burden. Moreover, the automated post-processing calculation eliminates the inter- and intra-rater variability inherent to manual goniometry. The use of standardized gesture images also aligns with routine clinical examination habits and allows for data traceability, ensuring consistency across repeated measurements.
Nevertheless, as a pilot study, several limitations must be acknowledged. First, our primary aim was clinical comparability with manual goniometry rather than biomechanical validation. The reliability of the reference method itself was not experimentally verified in this cohort and future studies should include formal intra-rater, inter-rater, and test-retest reliability analyses. In addition, a subset validation against an optoelectronic motion capture system or depth camera is needed to establish absolute accuracy. Second, our patient cohort was predominantly mild-to-moderate (Table S2, Swanson scores 0-25%), which is consistent with a large hand trauma follow-up reporting a mean impairment of 13.6%. 40 However, severe pathological conditions, such as open fractures, crush injuries and complex deformities, remain unverified. Furthermore, hand pose estimation algorithms suitable for anatomical variations like digit amputations or polydactyly are also needed. Third, our standardized setup and image collection protocol may limit applicability to real-world telemedicine. The robustness of our method should be evaluated under varied environmental conditions before deployment. Fourth, monocular imaging cannot fully resolve issues related to skin artefact, key point occlusion and multiplanar kinematics of the thumb. Further research using multi-view imaging or more sophisticated depth inference algorithms is warranted.
Conclusion
This feasibility pilot study evaluated an AI-based hand ROM measurement method in healthy individuals and patients with mild-to-moderate impairment. After geometric optimization, the method showed improved agreement with manual measurements for most parameters. However, thumb opposition/adduction and some PIP flexion measurements require further refinement, and applicability to severe pathological hand conditions and varied environmental conditions remains unverified. With these considerations, the method holds potential as a supportive tool for hand function assessment, and the findings provide a basis for subsequent validation studies.
Supplemental material
Supplemental material - Comparison of an AI-based hand range of motion measurement with manual goniometry: A prospective cross-sectional pilot study in patients and healthy volunteers
Supplemental material for Comparison of an AI-based hand range of motion measurement with manual goniometry: A prospective cross-sectional pilot study in patients and healthy volunteers by Fanbin Gu, Jingyuan Fan, Lulu Lv, Jiantao Yang, Qingtang Zhu, Honggang Wang in Science Progress
Supplemental material
Supplemental material - Comparison of an AI-based hand range of motion measurement with manual goniometry: A prospective cross-sectional pilot study in patients and healthy volunteers
Supplemental material for Comparison of an AI-based hand range of motion measurement with manual goniometry: A prospective cross-sectional pilot study in patients and healthy volunteers by Fanbin Gu, Jingyuan Fan, Lulu Lv, Jiantao Yang, Qingtang Zhu, Honggang Wang in Science Progress
Supplemental material
Supplemental material - Comparison of an AI-based hand range of motion measurement with manual goniometry: A prospective cross-sectional pilot study in patients and healthy volunteers
Supplemental material for Comparison of an AI-based hand range of motion measurement with manual goniometry: A prospective cross-sectional pilot study in patients and healthy volunteers by Fanbin Gu, Jingyuan Fan, Lulu Lv, Jiantao Yang, Qingtang Zhu, Honggang Wang in Science Progress
Footnotes
Acknowledgments
The authors thank Mr. Xiaolin Liu, Mr. Bai Leng, Mr. Zhenguo Lao, Mr. Lin Xiao and Ms. Jianwen Zheng for technical help, writing assistance, and general support.
Ethical considerations
Ethical approval to report this study was obtained from the institutional review board of The First Affiliated Hospital of Sun Yat-sen University (ID: [2021]387, approved on 1 June 2021).
Consent to participate
Written informed consent was obtained from all subjects before the study.
Author contributions
We have confirmed that all the authors meet the authorship criteria.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: National Key Research and Development Plan of China, (grant numbers 2022YFC3602801).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The anonymized coordinate dataset and analysis code supporting the findings of this study are publicly available in a GitHub repository: ![]() . The repository includes the coordinate data (anonymized), sample Python inference scripts, and a README file with instructions. The original images cannot be shared due to ethical restrictions.
. The repository includes the coordinate data (anonymized), sample Python inference scripts, and a README file with instructions. The original images cannot be shared due to ethical restrictions.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.