Resource use and quality of care in an urban stroke unit
JK Boyle, H Casey, CL Doyle and MR Walters
University of Glasgow, UK
Introduction: Stroke is the third most common cause of mortality and the most common cause of disability worldwide. Patients admitted to stroke units (SU) have better clinical outcomes. Availability of stroke unit care is determined by resources and logistics. We investigated the efficiency of bed use in a busy urban stroke unit, and compared simple indices of care between stroke patients placed on stroke units and in general wards. Patients and methods: Over a 3-week period we investigated all patients under the care of the stroke team. There were 3 groups: stroke patients within SU; medical boarders in SU; and stroke patients boarded out with SU. At 11 am on each weekday a snapshot view of all three groups was performed in order to assess bed management. Results: 29 stroke patients in ASU and 18 stroke patients boarded out were identified during the audit period (mean age 71.8 years, 57% male). Stroke patients within SU had significantly less time to brain imaging (mean 2.34 (SD=3.48) hours vs. 12.61 (SD=9.25) hours, p<0.0001), shorter time to therapist review (mean 25.15 (SD=22.92) hours vs. 43.96 (SD=34.84) hours, p=0.0447), more measurements of BP and GCS (mean 12.17 (SD=6.83) vs. 7.67 (SD=3.85), p=0.0243, and mean 7.81 (SD=4.90) vs. 3.56 (SD=2.60) measurements, p=0.033). Age, sex, DEPCAT score and time to consultant review did not differ between the two groups of stroke patients. The snapshot data revealed that bed capacity on ASU matched the number of stroke (mean number of stroke inpatients per day 8.44 (SD=2.53), 14 beds available). However, an average of 5.25 (SD=2.38) non-stroke patients were boarded into the SU every day. Conclusions: In our institution patients admitted to stroke units undergo more frequent clinical observation, and receive more rapid investigation and therapy than those admitted to general wards. These differences are not driven by differences in age, gender or privation, and may explain previously-observed differences in longer-term clinical outcomes. Our data suggest that a provision of stroke care could be improved through greater efficiency of bed use, without significant resource implications.
References
Stroke Unit Trialists’ Collaboration. Organised inpatient (stroke unit) care for stroke. Cochrane Database of Systematic Reviews 2007, Issue 4. Art.Management of patients with stroke or TIA: assessment, investigation, immediate management and secondary prevention. Scottish Intercollegiate Guidelines Network 108; December 2008.
Investigation of the adequacy of documentation of DNACPR decisions following the implementation of local guidance
Liesbeth Van Look and Andrew Jamieson
St John’s Hospital, Livingston, UK
Introduction: With recent changes in shift patterns, increasing numbers of medical staff are involved in the care of patients. Appropriate decision-making and adequate documentation are paramount to ensure optimal patient care. In 2006, NHS Lothian introduced the UK’s first fully integrated DNACPR policy to enhance care at the end of life.1Patients and methods: On a single day in the Medical Unit at St John’s Hospital, all in-patient medical records were examined by a single clinician. Each record was examined to determine the prevalence of DNACPR forms and thoroughness of completion of appropriate documentation. Key areas included documentation of the reason for not attempting CPR, the time of completion of the documentation, and any evidence of treatment escalation policy for each individual. Results: A total of 163 complete sets of notes were evaluated and 41 had a DNACPR form (25%). Of those with forms, the age range was 55–102 years (median 81 years). There were 17 women and 24 men. On 25 forms (61.0%) frailty and/or multiple co-morbidities was given as the main DNACPR reason. Other DNACPR reasons included metastatic/recurrent cancer (21.9%), chronic airways disease (7.3%), stroke (4.9%) and cardiac disease (2.4%). 21 forms were completed by junior staff and counter-signed. 7 forms were not counter-signed. A total of 17 (42%) patients had DNACPR forms either at the time of admission or completed on the day of admission, with a further 18 (44%) completed within 7 days of admission. Only 15 (37%) patients had the DNACPR decision recorded in the in-patient record, and escalation plans were present in only 5 (12%). Conclusions: Despite clear guidance regarding implementation of DNACPR guidance, the practical application of this is extremely limited and requires further action to ensure inappropriate resuscitation and treatment escalation does not occur.
What is the best long-term GH assessment strategy for adult survivors of childhood acute lymphocytic leukaemia (ALL)?
SC McGeoch, DJ King and JS Bevan
Aberdeen Royal Infirmary, UK
Introduction: A joint ‘late effects’ clinic for follow-up of survivors of childhood cancer has been in operation in our institution since 1995. In patients who have undergone cranial irradiation, dynamic anterior pituitary function testing using a standard insulin tolerance test (ITT) or, if contraindicated, a glucagon or arginine/GHRH test was undertaken at around five yearly intervals. Patients and methods: Case note review was undertaken for 24 patients (male: female ratio 1:1) who underwent cranial irradiation for ALL (age of diagnosis 5.8±3.6 years). 4/24 patients defaulted from adult clinic follow-up. 12/20 patients under follow-up had undergone more than one dynamic assessment of pituitary function. Results: Average time following cranial irradiation to first dynamic pituitary function testing was 17.1 ± 4.8 (10–26) years and at this point 65% of patients were GH deficient as defined by a peak GH <7 mcg/L. There was no difference between peak GH during the first and second dynamic test (p=0.53) and only one further patient was found to be GH deficient at the second dynamic test (20 years post cranial irradiation). 5/20 patients were on adult GH replacement therapy. Mean time between cranial irradiation and starting adult GH therapy was 16.8±8.5 years. Those patients with biochemical GH deficiency who were not started on GH replacement therapy were asymptomatic and did not satisfy NICE AGDHA criteria. 3/10 males under follow-up were on testosterone replacement therapy, all had undergone testicular irradiation. No patients had any other pituitary hormone deficiencies or required other hormone replacement therapy. Conclusions: Between 10 and 26 years following cranial irradiation for ALL 65% of patients developed biochemical GH deficiency illustrating the importance of well-organised long-term endocrine follow-up for this patient group. However, continued repeated dynamic pituitary function testing may be unnecessary as there was no deterioration in peak GH concentrations during subsequent tests. The optimum time interval for initial dynamic pituitary function assessment remains unclear.
Evolving trends in place of death in South West Scotland 2000–2010
H Black1, A Allan2, A Carnon2, D Clark3, K Donaldson1, F Graham4, P Hutchison4, L Martin4 and C Isles1
1Medical Unit, UK
2Department of Public Health, UK 3University of Glasgow, Dumfries Campus, UK
4Dumfries and Galloway Health Board, UK
Introduction: As the proportion of the population over 85 years increases so too has interest in place of death. Despite majority preference for death at home most deaths still occur in acute hospitals. Patients and methods: Descriptive analysis of 19,697 deaths in Dumfries and Galloway 2000–2010 using data provided by the National Records of Scotland Office before and after redesign of our out-of-hours service and introduction of an unscheduled collaborative care programme in 2005. Results: The proportion of deaths in acute hospitals rose from 45.4% in 2000 to 50.4% in 2005 before falling to 47.6% by 2010 (r2 = 0.907). Home deaths fell from 29.6% in 2000 to 24.9% in 2005 and 23.3% in 2010. Deaths in cottage hospitals were essentially unchanged during the period of study at 10.5%, 10.5% and 11.0% respectively, while deaths in care homes were 14.5% in 2000 and 14.2% in 2005 before rising to 18.1% in 2010. There were striking differences in place of death by cause of death: patients with dementia were most likely to die in a care home (68%) and least likely to die in an acute hospital (9%). Conclusions: Our data suggest evolving trends in place of death with fewer deaths in acute hospitals and more deaths in care homes since 2005. Death at home was less common in 2010 than it was in 2000. Health boards should continue to monitor trends in place of death in order to meet the needs and preferences of an ageing UK population.
An audit of the recognition and management of hypoglycaemia
E Murphy, DM Carty and RS Drummond
Glasgow Royal Infirmary, UK
Introduction: Hypoglycaemia in hospital inpatients is common and preventable; morbidity remains high despite national guidelines.1,2Patients and methods: Diabetes monitoring charts were screened in three medical wards of Glasgow Royal Infirmary during a 5-week period between 6 February 2012 and 9 March 2012. Any blood glucose level below 4 mmol was recorded. The nursing and medical notes were analysed to determine management of each episode. Results: A total of 67 hypoglycaemic events were identified in 37 different patients during a 5-week period. Almost one quarter of the events (29; 24%) led to no treatment being administered and of those, half (14; 50%) of the patients went on to have a further event. Over half (28; 57%) of the hypoglycaemic events did not have documentation of a repeat BM and of these patients, just over half (20; 52%) had a further hypoglycaemia event. 39 (58%) of the hypoglycaemic events led to an initial formal review following the episode with the majority performed by the ward doctor (25; 64%) and of those just over one third had a further hypoglycaemia episode (15; 38%) whereas more than half (15; 54%) of those who were not formally reviewed by a doctor had a further episode. Conclusions: The results of this audit have shown that both nursing and medical staff are not treating and managing hypoglycaemic events as set out in local and national guidelines. Our data suggest that patients who do not have their BM rechecked are more likely to have a further hypoglycaemic event and are at further risk of hypoglycaemia if the previous event was not treated appropriately. These results suggest that if the patient has a formal review by the ward doctor they are less likely to have a further hypoglycaemic event. As a result, we have designed a hypoglycaemia protocol, highlighting the diagnosis and management, for both nursing and medical staff in order to improve these results. We will re-audit this once the protocol has been fully introduced.
References
Hackett, E. An audit of knowledge and treatment of hypoglycaemia. Br J Clin Pharm 2010: 1; 185–186.Diabetes UK 2010 Guidelines. Hospital management of hypoglycaemia in adults with diabetes mellitus.
Can an ambulatory pathway for investigation and management of pulmonary embolism prevent admission and save on bed days?
ADL Marshall and K Carter
Aberdeen Royal Infirmary, UK
Introduction: Suspected pulmonary embolism (PE) is a common presentation to acute medicine. There is evidence supporting both outpatient management and investigation of possible PE in selected patients at low risk of death.1–4 Since November 2011, we have investigated low-risk patients in our ambulatory clinic. Patients and methods: Retrospective case note analysis of all patients managed in the ambulatory setting over 6 months. Suitable patients were either d-dimer positive with low risk pre-test probability (PTP) (Geneva score) or intermediate PTP. All patients should have had a normal chest x-ray and a Pulmonary Embolus Severity Index (PESI) score of <86 to be eligible. Results: We reviewed 22 patients’ case notes. 100% of patients were investigated by VQ scan as ambulatory CTPA slots are unavailable. Two patients (9%) had confirmed PE. Three patients had an abnormal CXR and should have been excluded from ambulatory management. One patient was imaged despite being low risk and d-dimer negative. One patient was subsequently readmitted with confirmed pulmonary embolism on CTPA after negative VQ. 49 bed days were saved (average 2.3/patient) by ambulatory management. 72% of patients had their scan on a Monday. Conclusions: Some patients were investigated inappropriately suggesting further education and reinforcement is needed. A majority of patients were seen on a Monday suggesting ambulatory management was used to avoid admission over the weekend. Ambulatory management clearly saves on hospital bed-days. Access to CTPA should allow further development and savings.
References
Jiménez D, Yusen RD, Otero R, et al. Prognostic models for Selecting patients with acute pulmonary embolism for initial outpatient therapy. Chest 2007; 132: 24–30.Chan CM, Woods C and Shorr AF. The validation and reproducibility of the pulmonary embolism severity index. J Thromb Haemost 2010; 8: 1509–1514.Rowlinson JS, Deagle J and Roseveare CD. Ambulatory investigation and treatment of patients with suspected pulmonary embolism. J R Coll Physicians Edinb 2006; 36: 12–16.McDonald AH and Murphy R. A pilot audit of a protocol for ambulatory investigation of predicted low risk patients with possible pulmonary embolism. J R Coll Physicians Edinb 2011; 41: 196–201.
Emergency readmissions to a medical unit: Higher than you would think
LSI Suleiman and JD Walker
St John’s Hospital, Livingston, UK
Introduction: Readmission rates to hospitals have increased over the past decade. Data from the Scottish government in December 2011 suggests the rate to be around 11%. Patients and methods: The aims of this study were to determine the 7- and 28-day readmission rate to our Medical Unit, and to identify various factors associated with the likelihood of a readmission. A retrospective study looking at patients admitted to the Acute Medical Unit during a week in January using the hospital computer system then a detailed review of case-notes of those admitted. Results: From a total of 170 patients, 42 were readmissions, giving a readmissions rate of 13% within 7 days, and 25% at 28 days. Readmissions were more frequent on a Friday and Saturday (17 vs. an expected of 12). Subsequent analysis are for 26 of the 42 patients (62%) with complete data: 69% of readmissions were older than 65 years, and 73% were female, 58% had an initial length of stay of less than 7 days and 65% were due to a similar presentation or complication from previous admission. 38% had physiotherapy during their initial admission, 27% had occupational therapy, and 24% had any package of care in place at the time of initial discharge. 23% were considered to be social admissions. Conclusions: Shortcomings of this survey are that we have not compared the readmitted cohort with those who were not readmitted and that this is a small survey conducted over a short time period. However, we are able to conclude that the 7- and 28-day medical emergency readmission rate to our unit during this period is more than double the rate published by the Scottish government.
Introduction of sepsis bundle stickers in the emergency receiving unit
S Sullivan, S Maclean, V Sharma and S Chohan
Monklands Hospital, UK
Introduction: Sepsis is common and causes significant morbidity and mortality.1 Early recognition and management improve outcomes.2 Checklists have been shown to improve compliance with best practice.3 The Surviving Sepsis Campaign sepsis bundle is associated with improved outcome.1 We introduced a sepsis bundle checklist sticker based on the Surviving Sepsis criteria into the Emergency Department (ED) and Emergency Receiving Unit (ERU) in our District General Hospital and measured how its use affected the management of patients with sepsis. Patients and methods: Prospective case note review in the ERU, 1 day per week over 6 weeks. We measured whether sepsis sticker placed in notes, blood cultures taken, antibiotics given within NHS Lanarkshire policy, antibiotics within 1 hour of recognition of sepsis, lactate measured. Compliance with the checklist was compared between those with and without a sticker. Results: Of the 22 patients identified with sepsis, 7 (32%) had a sepsis sticker vs. 15 (68%) did not. 7 (100%) vs. 9 (60%) had blood cultures, 7 (100%) vs. 2 (13%) had antibiotics within 1 hour of sepsis recognition, 5 (72%) vs. 13 (87%) had antibiotics compliant with NHS Lanarkshire policy, and 7 (100%) vs. 5 (33%) had lactate measured. Conclusions: The use of sepsis bundle stickers is associated with higher compliance with protocol in the early management of patients with sepsis; however, use of the sticker was low. Small numbers were involved and we are therefore unable to draw strong conclusions. Selection bias is likely. We cannot say whether the positive effect of the stickers could be sustained. It may be that implementation of our sepsis bundle sticker in the ED and ERU would guide appropriate evidence-based management of sepsis. Reasons for poor recognition of sepsis and non-use of the sticker should be explored.
References
Dellinger RP, Levy MM, Carlet JM, et al. Surviving Sepsis Campaign: International guidelines for management of severe sepsis and septic shock. Crit Care Med 2008; 36: 296–327.Rivers E, Nguygen B, Havstad S, et al. Early goal-directed therapy in the treatment of severe sepsis and septic shock. N Engl J Med 2001; 345: 1368–1377.Haynes AB, Weiser TG, Berry WR, et al. A surgical safety checklist to reduce morbidity and mortality in a global population. N Engl J Med 2009; 360: 491–499.
Hospital readmissions: A lengthy process
N Hunter and E MacDonald
Western General Hospital, Edinburgh, UK
Introduction: A retrospective analysis of 100 consecutive readmissions of patients aged over 65 years was undertaken at the Western General Hospital, Edinburgh between 1 August 2008 and 23 September 2011. These readmissions comprised 13% of the total number of emergency medical admissions aged over 65 during this period. This study aimed to identify all patients readmitted in the defined period and explore the reasons for their further presentation. Patients and methods: The data was collated from TRAK online electronic medical records system and included patient demographics, length of stay, time interval between admissions, reason for admission, co-morbidities and the specialty involved in their care. Results: Of the 100 patients studied 45 were male and 55 were female. Mean age was 81.9±7.7. The mean length of stay was shown to increase significantly on readmission, from 10.8±15.5 days on the first admission to 20.0±28.8 on the second admission (p<0.0015). Additionally, 48% of patients were readmitted within 1 week of discharge and in this group the reason for the readmission was the same as their initial presentation in 59% of cases. These patients had multiple comorbidities (mean 5.9±2) and polypharmacy (mean 9.9±4.5 drugs on initial discharge). The number of drugs the patients were discharged on after their readmission was not significantly different to their first discharge 10.3±4.7.30% of these patients were managed by Medicine of the Elderly (MoE) on their first admission with a higher percentage of 43% admitted to MoE on readmission. Conclusions: This study highlights that the readmissions observed are characterised by their age, complexity with significant comorbidities and polypharmacy. Furthermore, their readmission is with the same initial problem in 59% of patients and their readmission occurs within just 1 week of previous discharge in almost half of cases. Despite their age and complexity less than half of these patients studied were admitted to the care of MoE.
If it looks like it and smells like it … how good are we at detecting Clostridium difficile associated diarrhoea?
C Adams and TJ Quinn
Glasgow Royal Infirmary, UK
Introduction:Clostridium difficile associated diarrhoea (CDAD) is an important hospital-associated infection with significant associated morbidity and mortality. In 2011 there were 2078 cases of CDAD in Scotland,1 and 270 deaths recorded CDAD as a cause or contributing factor.2 Health professionals suspect CDAD if stool is foul-smelling, green-tinged, or the patient has had recent antibiotics. We aimed to describe the diagnostic accuracy of this basic initial clinical assessment for CDAD. Patients and methods: Information was collected on all patients with loose stool across various settings in a single hospital. We included 4 geriatric assessment wards (two week data collection); 2 gastroenterology wards (8 weeks); 3 medical receiving wards (3 weeks); 1 surgical receiving ward (1 week). On first presentation of loose stool we asked medical and nursing staff if they suspected CDAD. We assessed diagnostic accuracy of this clinical assessment against results of laboratory testing when available. Results: Of 72 patients with loose stool, 58 had specimens sent for analysis; 17 were suspected CDAD, of which 5 were confirmed positive. Sensitivity of healthcare staff for CDAD prediction was 71.4% (95% CI: 35.9–91.8%), and specificity 76.5% (95% CI: 63.2–86%). Positive predictive value 29.4% (13.1–53.1); negative predictive value 95.1% (83.9–98.7). Likelihood ratio (LR) positive was 3.0 (1.5–6.0%), and LR negative was 0.37 (0.12–1.2%). Conclusions: It is desirable to start treatment of CDAD as soon as possible, as delay in initiating treatment could cause harm. However, our data suggest that clinical assessment alone for possible CDAD is suboptimal. Clinical assessment combined with readily available laboratory data such as white cell count may perform better. Our data are open to bias as not all subjects had stool samples sent for analysis.
High sensitivity troponin T in acute medical admissions: A prospective cohort study
M Anwar1, M Fakri1, M Kerr1, J Abed1, RAP Weir2 and CJ Petrie1
1Monklands Hosipital, UK
2Hairmyres Hospital, UK
Introduction: Troponin (Tn) testing in acute medicine is routine, the standard Tn T assay cannot detect levels <30 ng/L. A new high sensitivity assay (hs Tn T) can detect levels down to < 14 ng/L. There is diagnostic uncertainty regarding hs Tn T thresholds and their clinical significance, in the acute medical setting. Patients and methods: Prospective cohort study of patients attending an acute medical admission unit (AMAU) in a busy District General Hospital. All those with a hs Tn T level ≥ 14 ng/L (> 99th centile) over a 1-month period were recruited. Results: Of 564 patients with a troponin measured, 224 (40%) had a hs Tn T ≥14 ng/L. Median (IQR) peak Tn T level was 47.5 ng/L (24–130) and 36% had a hs Tn T < 30 ng/L. Mean (SD) age was 72 (12) years and 57% were male. Mean (SD) creatinine 120 (103); mean (SD) estimated glomerular filtration rate was 50 mL/min/1.73 m2 (14) and mean (SD) haemoglobin was 13 g/dL (8.4). The commonest presenting symptoms were chest pain (34%), breathlessness (21%), and pre-syncope (13%). Final diagnosis was wide-ranging with cardiac (heart failure, valve disease, arrhythmia, myocarditis, endocarditis) and many non-cardiac (including sepsis, respiratory failure, pulmonary embolus, stroke, pancreatitis, gastrointestinal bleeding, disseminated malignancy, seizures, renal failure, necrotising fasciitis) findings. Acute myocardial infarction (AMI) was seen in only 20%. A ‘non-cardiac’ diagnosis accounted for approximately 55% of all patients. Amongst others, electrocardiographic findings included normal sinus rhythm in 24%, atrial fibrillation/flutter (12%), ST depression (10.4%), ST elevation (4.1%) and sinus tachycardia (4%). Coronary angiography occurred in 14.5%, revascularisation in 9%, was associated with improved survival but represented selection bias in favour of those without extensive co-morbidity. Echocardiography was performed in 31% and left ventricular systolic dysfunction documented in 17%. Prognosis was poor with 65 deaths (29.5%) over a mean (SD) follow up of 344 (20) days. Mortality at 30 days was 12.5%; at 90 days 18.8% with 23 deaths (35% of total) occurring after 90 days. In a multivariate model, independent predictors of death were elevation in C-reactive protein, non-treatment with enoxaparin, elevation in white cell count and increasing age. Outcome was worse for those with no dynamic change in hs Tn T on repeat testing, representing 50% of the study cohort. These patients were more likely to have systemic illness such as sepsis, heart failure, renal dysfunction or respiratory disease. Conclusions: Elevation in hs Tn T is common in the AMAU, prognosis is poor and most do not have a diagnosis of AMI. Up to 50% have no dynamic rise and or fall in Tn T. It is not known whether improvements in outcome can be modified by an alternative therapeutic strategy, than is currently in place.
Endobronchial ultrasound transbronchial needle aspiration at Aberdeen Royal Infirmary
ADL Marshall, D Miller, P Mahendra, J Miller, M Chetty and GP Currie
Aberdeen Royal Infirmary, Aberdeen, UK
Introduction: Endobronchial ultrasound transbronchial needle aspiration (EBUS-TBNA) is a superior alternative to mediastinoscopy for sampling mediastinal lymph nodes and masses. We wish to describe the demographics, results and diagnostic sensitivity of EBUS-TBNA in the first consecutive 150 patients in whom this procedure was performed at Aberdeen Royal Infirmary. Patients and methods: Since the service began, patient age, gender, numbers of passes for each node and results were recorded on a protected spreadsheet, which we retrospectively interrogated. Results: Of the 150 patients, 62% were male with mean age 63 years (range 22–88). 206 lymph nodes were sampled with a median of 5 passes per node. Lymphoid material was obtained in 139 (93%) of samples. A pathological abnormality was found in 111 patients (74%). Of these 51 (46%) were non-small cell lung cancer, 27 (24%) were small cell lung cancer, 24 (22%) showed granulomatous inflammation consistent with sarcoidosis and 9 (8%) had either tuberculosis or metastatic breast, colon, renal tract or head and neck cancer. In the remaining 39 patients, no lymph node was sampled in 11 and lymph nodes were sampled in 28 with no obvious abnormality. Of the latter, 12 were true negatives. The diagnostic sensitivity for EBUS-TBNA for all 150 cases was 82% (77% in the first 50 patients sampled versus 84% in cases 51–150.Conclusions: A variety of different cell types can be identified by the use of EBUS-TBNA. Our overall diagnostic sensitivity was 82%, although it would appear reasonable to consider that the top of the learning curve is achieved not long after 50 procedures have been performed.
Reference
Miller D, Mahendra P, Bruce V, et al. Endobronchial ultrasound transbronchial needle aspiration at Aberdeen Royal Infirmary: the initial experience. QJM 2012; 105: 607–608.
PB15
Prediction of hip osteoarthritis using DXA images
K Yoshida1,2, J Gregory2, B Mason3, I Reid3 and DM Reid2
1ST4 Rheumatology, Department of Rheumatology, Aberdeen Royal Infirmary, UK
2University of Aberdeen, Aberdeen, UK
3University of Auckland, Auckland, New Zealand
k.yoshida@nhs.net
(01224) 554782
Introduction: Osteoarthritis (OA) is a common musculoskeletal disease and the burden will increase alongside lifespan. Dual energy X-ray absorptiometry (DXA) measures bone mineral density (BMD) to assess osteoporosis and the images can be used to assess hip OA using Kellgren-Lawrence grading (KLG). Active shape modelling (ASM), a statistical modelling technique applied to radiographs, has been shown to predict hip OA progression.1. This study aimed to assess whether active appearance modelling (AAM), an extension of ASM incorporating BMD distribution applied to DXA images, can predict progression of hip OA in a longitudinal cohort. Patients and methods: Hip DXA scans taken every 30 months over 5 years from postmenopausal women in the Auckland Calcium Study2 were scored for OA using KLG and modelled using AAM. Hip OA progression was defined as: (a) hip arthroplasty (HA) (excluding hip fracture and avascular necrosis) or (b) KLG change of ≥1/2 grade based on progressive OA features and KL≥2 on final scan. Frequency matching for age obtained a 1:3 ratio of OA progression cases (a and b) to never OA controls (n=378). Odds ratios (OR) were calculated after adjustment for KL. Results: Significant correlations (p<0.001) were found between baseline KLG and 6 Appearance modes (App) including 13 and 16 (r= --0.24 and 0.16). When OA progression was defined as HA of the scanned hip (cases n=21, controls n=419), 3 modes including App16 showed significant differences (OR 2.36 (1.38–-4.03)). With incident hip OA defined as KLG≥2 at follow up (cases n=47; controls n=378), App7 and 13 showed significant OR (OR 1.78 (1.19–-2.36); OR 0.7 (0.50–-0.98)). When OA cases were defined as KLG change≥1/2 or HA (n=126) and controls included non-progressive hip OA cases (n=419), 6 modes (App7, 13 and 16 inclusive) remained significant. Conclusions: AAM can be applied to DXA images to assess and predict progression of hip OA. This makes DXA an attractive modality to assess and predict the two most common musculoskeletal diseases in the elderly population.
References
Gregory JS, Waarsing JH, Day J, et al., Early identification of radiographic osteoarthritis of the hip using an active shape model to quantify changes in bone morphometric features: can hip shape tell us anything about the progression of osteoarthritis? Arthritis Rheum 2007; 56: 3634–-3643.Reid IR, Mason B, Horne A, et al. Randomized controlled trial of calcium in healthy older women. American Journal of Medicine. 2006; 119(9): 777–785.
PB16
Baclofen, a GABA-B Agonist, Improves Alcohol Consumption, Psychometrics and Hospital Admission Rates in Patients with Alcoholic Liver Disease
Benn Macdonald1, Neil Masson2, Jim Lewsey1, Leona Cunningham31, Aleksandra Irnazarow31, Amanda Nardone31, Jan Cosgrave31, Jonathan Chick43 and Mathis Heydtmann54
1Institute of Health and Wellbeing, University of Glasgow, Glasgow, UKnited Kingdom.
2Department of Psychiatry, NHS Lanarkshire, Lanark, UKnited Kingdom
3Department of Psychology, University of Glasgow, Glasgow, United Kingdom.
4Department of Psychiatry, Queen Margaret University, Edinburgh, UKnited Kingdom.
5Department of Gastroenterology, RAH Paisley, Paisley, UKnited Kingdom.
mathis@doctors.org.uk
Introduction: Alcoholic liver disease (ALD) contributes significantly to global health burden and cost not least through frequent hospitalisations. Mortality due to ALD is significantly higher in Scotland than in the rest of the UK and even higher in the Greater Glasgow area. In 53 patients admitted to a Glasgow hospital with ALD, out of license treatment with baclofen as anti-craving drug was initiated. We here analysze our case series of patients treated with out of license baclofen with regards to effectiveness in reduction of alcohol consumption and adverse consequences of alcohol consumption. Patients and methods: Clinical information was prospectively collected. Patients were given tailored dose baclofen for a mean of 5 months and patient care was handed over to the general practitioner who treated patients as she felt appropriate. Patients were sent standardiszed and in- house questionnaires and followed up for hospital re-admission for a mean of 30 months. Results: With this approach patients reported a reduction in alcohol consumption by an average of 58.7 %. Self- reported alcohol craving improved significantly (AUQ, p=0.004) as did consequences of drinking (DrInC-SIP2R, p=0.02) but not anxiety (p = 0.16), depression (p = 0.5) or quality of life (p = 0.94). In the first 2 years after initiation of treatment, patients spent on average 6.37 days per year less in hospital compared to before (p = 0.59). Reduction in hospitaliszation was related to duration of treatment with tailored dose baclofen (p = 0.066) with an average benefit of 0.81 hospital days less per year for 1 month of baclofen treatment. Higher patient age was associated with increased benefit from baclofen (p = 0.037), average benefit of 0.46 hospital days less per year for 1 year increase in age. Conclusions: We propose randomiszed controlled trials of baclofen should be conducted and can be powered to demonstrate a benefit in hard endpoints such usage of NHS resources.
PB17
Management and outcomes of patients with subdural haematoma in the Borders General Hospital January 2009 to- June 2011
HY Lim, and JF Faccenda
FY1 Anesthetics. Borders General Hospital
limhanying88@yahoo.co.uk
07838715171
Introduction: In a DGH setting we are reliant on tertiary services to advice regarding the care of subdural haematomas. There is currently a lack of specific guidelines. Therefore the advice and management provided is variable. We aimed to look at how patients are managed in the Borders General Hospital and their outcomes. Patients and methods: A retrospective study of 23 cases was undertaken with a diagnosis of subdural haematomas over 2.5- year period. We examined patient demographics, management, and outcomes. Results: 23 cases were identified; however, 2 were excluded due to lack of information. The incidence in this population was 8.1/100,000. Four patients (19%) who underwent surgical intervention were discharged with a mean length of stay of 32.5 days. In the group conservatively managed, mortality was 30.4%. Ten patients (58.8%) in this group were discharged and had a mean length of stay of 28.2 days. Four patients (19%) were readmitted within a 6- month period. Conclusions: Mortality rates are comparable to a previous study. Deaths in this group were a direct consequence of subdural haematoma or because of complications of poor mobility and frailty. In our cohort, patients who underwent surgical intervention had a better outcome.
References
BMJ best medical practice, subdural haematoma,: http://bestpractice.bmj.com/best-practice/monograph/416.html.Asghar, M., Adhiyaman, V., Greenway, M. W., et al.Bhowmick, B. And Bates, A. Chronic subdural haematoma in the elderly - a North Wales experience. J R Soc Med 2002;: 95: 290–-292.National Records of Scotland.
PB18 – Winner of the Best Poster Award
Pre-stroke risk stratification and oral anti-coagulant (warfarin) prescribing in hospitalised stroke patients with known atrial fibrillation
A Coyte1, P Fearon2, D Stott2 and P Langhorne2
13rd Year Medical Student, School of Medicine, University of Glasgow, UK
2Academic Section of Geriatric Medicine, University of Glasgow
patricia.fearon@glasgow.ac.uk
00 44 141 211 4976 / 00 44 7816420015
Introduction: Much emphasis has been placed on improving comprehensive assessment of stroke risk in atrial fibrillation (AF). A risk factor- based approach incorporated in the CHA2DS2VASC score is now recommended. Using pre-stroke CHA2DS2VASC scores we aimed to risk stratify patients with AF who subsequently develop stroke and determine factors associated with oral anti-coagulant (warfarin) prescribing. Patients and methods: Consecutive acute stroke presentations, from a geographically defined population in East Glasgow were recorded over 5 completed calendar years spanning a decade (August 2000–July 2002 and August 2007–July 2010). Recorded variables included age, sex, vascular risk factors, admission medications, pre-morbid function (dichotomised modified Rankin scale (mRS)) and imaging results. Pre-stroke CHA2DS2VASC scores were calculated retrospectively. All analyses were performed using SPSS 18.0. Results: We recorded 1833 acute stroke presentations. Prevalence of prior known AF was 13.4% (n=246). Median pre-stroke CHA2DS2VASC score was 5 (IQR 3,6). Whilst 233 (95%) patients with AF met criteria for oral anticoagulation (i.e. pre-stroke CHA2DS2VASC ≥ 2), warfarin was prescribed pre-stroke to only 50 (22%); rates of warfarin prescribing in AF were unchanged over the 10-ten year period; in comparison to patients who were not anti-coagulated, patients on warfarin were younger (69.7 years vs. 77.1 years; p<0.001), more likely to have had prior history of TIA (22.9% vs. 10.3%; p=0.027) and to have been independent before their stroke (pre-stroke mRS 0-2: 92% vs. 75%; p=0.012). Conclusions: Most patients with stroke and AF have not been receiving effective thromboprophylaxis with warfarin prior to their presentation. Clinicians are apparently being highly selective in warfarin use, with younger, more independent patients with prior transient cerebral ischaemia more likely to receive warfarin before their stroke. Routine use of risk prediction scores to guide anti-coagulation has the potential to substantially reduce the risk of embolic stroke due to AF.
Reference
Olesen JB, Lip GY, Hansen ML, et al. Validation of risk stratification schemes for predicting stroke and thromboembolism in patients with atrial fibrillation: nationwide cohort study. BMJ 2011; 342: d124.
PB19
Audit of analgesia prescribing in cancer patients – are we meeting the current standards?
Dr Rosemary RS A Meharry, Dr Claire SR Holmes and Dr Holly Edmondson
Dr Meharry – Foundation Year 1, General Medicine, Monklands Hospital, Airdrie, UKMonklands Hospital, Airdrie.
Dr Holmes – Core Medical Trainee 1, General Medicine, Monklands Hospital.
Dr. Edmondson - Foundation Year 1, General Medicine, Monklands Hospital, Airdrie.
rosiemeharry@gmail.com
07845515212
Introduction: Cancer pain is often inadequately managed despite the existence of guidelines at local, national and international levels. This audit analysed analgesia prescribing in patients with cancer pain in a district general hospital to assess prescribing adherence to the current SIGN guidelines.1Patients and methods: A cross-sectional study was performed over the medical, surgical and care of the elderly wards in Monklands Hospital. The notes of those inpatients with documented cancer pain were assessed to ensure prescribing adhered to the current SIGN guideline. Results: Of the notes reviewed. 29 patients were documented to be on analgesia for cancer pain, 14 of which had proven metastatic disease. 23 (79%) patients were prescribed analgesia at step 1 of the pain ladder. Adjuvants were prescribed in 21 (72%) of all cases. 25 patients were prescribed opiates, 8 (28%) were on regular weak opiates and 17 (59%) on strong opiates. Of those on opiates 14 (56%) were prescribed breakthrough analgesia. Conclusions: This review shows that prescribing in Monklands Hospital is adhering to currently practiced guidelines. However, from the results it is noted that the prescribing of breakthrough analgesia is inadequate, with only 56% of patients on regular opiates having breakthrough analgesia available. We plan to provide a teaching session to junior medical staff to ensure awareness of the analgesic ladder and the importance of breakthrough analgesia prescribing in managing caner pain.
Reference
Control of pain in adults with cancer. A national clinical guideline. Edinburgh: Scottish Intercollegiate Guidelines Network, November 2008.
PB20
Determinants of poor quality of life in ANCA- Associated Vasculitis (AAV)
N Basu, GT Jones, GJ Macfarlane and DM Reid
Senior Clinical Lecturer in Rheumatology, University of Aberdeen, UK
neilbasu@abdn.ac.uk
01224 437144
Introduction: ANCA- associated vasculitis (AAV) are auto-immune conditions, which are managed by multiple specialities. Advances in treatment have led to their becoming chronic illnesses with good long- term survival. However, patients continue to report significantly reduced quality of life (QOL) for which the precise cause(s) are unknown. This study aimed to identify the determinants of poor QOL amongst AAV patients in order to inform future interventions designed to modify this crucial outcome. Patients and methods: A cross-sectional study was conducted. AAV cases were recruited from across the UK. Participants completed a questionnaire which determined physical- and mental-health- related QOL (SF36 physical and mental component summary scores; PCS and MCS). The questionnaire also collected data on putative psychosocial determinants of poor QOL, such as depression and fatigue. Concurrently, putative clinical determinants, such as assessments of disease activity and renal function were measured. Variables were categorised and 2 multivariable explanatory models of poor PCS and MCS were developed using forward stepwise logistic regression and expressed as odds ratios (OR) and 95% confidence intervals. The importance, in population terms, of the identified associations was quantified using population attributable risks (PAR). Results: Of 486 invited patients, 410 participated (86%): 49% male, median age 63.5 years (inter-quartile range 51.8–-72.4 years). The final multivariable models identified clinical (e.g. CRP, nervous system involvement) and psychosocial factors (e.g. sleep disturbance, depression) found to be independently and significantly associated with poor PCS and MCS. Fatigue was the only factor to be associated with both PCS (OR 3.2, 1.5–-6.9) and MCS (OR 4.0, 1.8–-8.9) and was also, by far, the greatest contributor to poor QOL in population terms across both models (PAR 24.6% and 47.4% respectively). Conclusions: Poor QOL amongst AAV patients is determined by multiple clinical and psychosocial factors;, however, fatigue appears to be the most important. Clinically, optimal control of underlying inflammation and neurological manifestations are likely to improve aspects of QOL;, however, multidisciplinary interventions targeting psychosocial determinants may offer even greater gains.
PB21
Does process of care explain the apparent socioeconomic inequalities in stroke outcomes?
S Wong, MR Walters and TJ Quinn
Lecturer, Institute of Cardiovascular & Medical Sciences, School of Medicine, University of Glasgow, UK
Terry.quinn@glasgow.ac.uk
+44 141 2114976
Introduction: Low socioeconomic status (SES) is associated with poor outcomes from cardiovascular disease including stroke, these poor outcomes are independent of traditional vascular risk factors. Differing processes of care may explain this apparent inequality. Our aim was to determine whether stroke care (investigation and prescribing) is influenced by SES and associations with stroke outcomes. Patients and methods: We collected data from Glasgow Royal Infirmary and Western Infirmary, chosen to represent deprived and affluent areas in one city. We identified consecutive ischaemic stroke admissions aged less than 75 years (August–November 2011 inclusive). We derived clinical and demographic data; outcomes; investigations and prescribing details from case note review. SES was described as Scottish Index of Multiple Deprivation using postcode data. We analysed the proportion of patients who received comprehensive investigations (taking carotid ultrasound as exemplar) and prescribing (taking antiplatelet and statins as exemplars) in relation to SES using univariate and multivariate analysis. Results: We assessed 200 ischaemic stroke patients (51% men, median age 65 years). Deprivation was over-represented in our study population n=95 (53%) in lowest SIMD quintile. Previous vascular events (p=0.04; smoking (0.03)) were more common in lowest SIMD quintile. There was no association between SIMD and outcomes (modified Rankin p=0.85; mortality p=0.75). We found no association between SES and investigation or prescribing patterns. All results remained non-significant after adjusted for age, sex and vascular risk factors in multivariate analysis. Conclusions: We found no association between socioeconomic deprivation and process of care in stroke. However, in contrast to other studies, we also found no association between deprivation and stroke outcomes. The high prevalence of deprivation in our population skewed the dataset and consequently our study may have had insufficient power to detect a true effect.
PB22
Predictors of anticoagulant prescribing in Glasgow stroke survivors with atrial fibrillation – a registry- based analysis
S Wong, C McAlpine, C Young and TJ Quinn
Lecturer, Institute of Cardiovascular & Medical Sciences, School of Medicine, University of Glasgow, UK
Terry.quinn@glasgow.ac.uk
+44 141 2114976
Introduction: Risk of stroke related to atrial fibrillation (AF) is substantial. Risk can be quantified, CHADS2 and CHA2DS2-VASc tools estimate stroke risk based on clinical data (heart failure; hypertension; age; diabetes; vascular disease; sex). The strongest predictor of stroke is history of previous stroke. Guidelines recommend anticoagulation for stroke survivors with AF. We sought to describe anticoagulation prescribing patterns in community based stroke survivors with AF. Patients and methods: We used Glasgow General Practice (GP) data. As part of the Local Enhanced Service, GPs perform detailed annual reviews on stroke survivors. We collected clinical and demographic data, including vascular risk factors; comorbidity; disability; history of alcohol or bleeding. We described socio-economic status using Scottish Index of Multiple Deprivation (SIMD); we described stroke risk using CHADS2 and CHA2DS2-VASc. Associations with anticoagulation were described using univariate and multivariate analyses. Given the multiple analyses we chose a significance level of p<0.001. Results: Data were available for 3429 stroke survivors with AF; 1699 (49%) male; median age 78 (IQR: 72–-84). Median CHA2DS2-VASc was 5 (IQR: 4–-6). Anticoagulation (warfarin) was prescribed in 1165 (34%). Univariate analysis suggested younger age; higher socioeconomic status; history of depression; smoking; obesity and no disability were associated with anticoagulation prescription (p<0.001). Those with higher CHADS2 and CHA2DS2-VASc scores were less likely to be prescribed anticoagulation (p<0.001). On multivariate analysis only age; depression and SIMD were independently associated with anticoagulation prescription. Conclusions: AF is prevalent in community dwelling stroke survivors and is undertreated. In this population at high risk of stroke. Risk factors for future stroke or anticoagulation related adverse event were not clearly associated with anticoagulation. Those at highest risk of stroke were less likely to be treated. Further work should describes barriers to anticoagulation and attempt to improve anticoagulation rates.
PB23 (combined)
Questionnaire assessment of usual practice in mood and cognitive assessment in Scottish stroke units
R Lees, NM Broomfield and TJ Quinn
Lecturer, Institute of Cardiovascular & Medical Sciences, School of Medicine, University of Glasgow, UK
Terry.quinn@glasgow.ac.uk
+44 141 2114976
Introduction: National and international guidelines recommend cognitive and mood assessment for all stroke survivors but there is no formal guidance on preferred method. We aimed to describe clinical practice across Scottish stroke units. Patients and methods: We created a short questionnaire survey to describe use of cognitive and mood assessments in acute, rehabilitation and outpatient stroke settings. The questionnaire was piloted locally and revised. We used mixed methodologies of distribution to ensure comprehensive national coverage. Scottish Stroke Managed Clinical Network co-ordinators distributed the questionnaire to staff; we accessed mailing lists for relevant special interest groups (geriatric medicine; stroke physicians; allied health professionals; stroke nurses and clinical psychologists) and we distributed paper copies through the U.K stroke forum delegate pack. Results: We received 174 responses, comprising: clinicians (n=61, 35%); occupational therapists (n=27, 16%); nurses (n=23, 13%); psychologists (n=13, 7%); physiotherapists (12, 7%). Return rate was highest from Greater Glasgow and Clyde (n=55, 32%). Of respondents 148 (85%) described routinely assessing cognition, 119 (72%) for mood. A variety of tools were used (cognitive n=45 tools; mood n=17). Mini Mental State Examination (n=162 respondents) and Abbreviated Mental Test (n=112) were the most popular cognitive screens. Hospital Anxiety and Depression Scale (HADS) (n=109) and Geriatric Depression Scale (n=79) were the most popular mood screens. Conclusions: Response rate was low but included all Scottish regions with active stroke services. Although the majority of responders are assessing cognition and mood there is substantial heterogeneity in measures used and certain popular tools may not be suitable for use in stroke. Greater consistency in choice of assessment tools, based on evidence of test accuracy in stroke survivors is required.
PB23 (combined)
Diagnostic test accuracy of various brief screening tools for detection of cognitive impairment or delirium in an acute stroke setting
R Lees, S Corbet, J Lua, C Johnston, E Melling, Y Miao, E Moffitt, G Shaw, J Tan and TJ Quinn
Lecturer, Institute of Cardiovascular & Medical Sciences, School of Medicine, University of Glasgow, UK
Terry.quinn@glasgow.ac.uk
+44 141 2114976
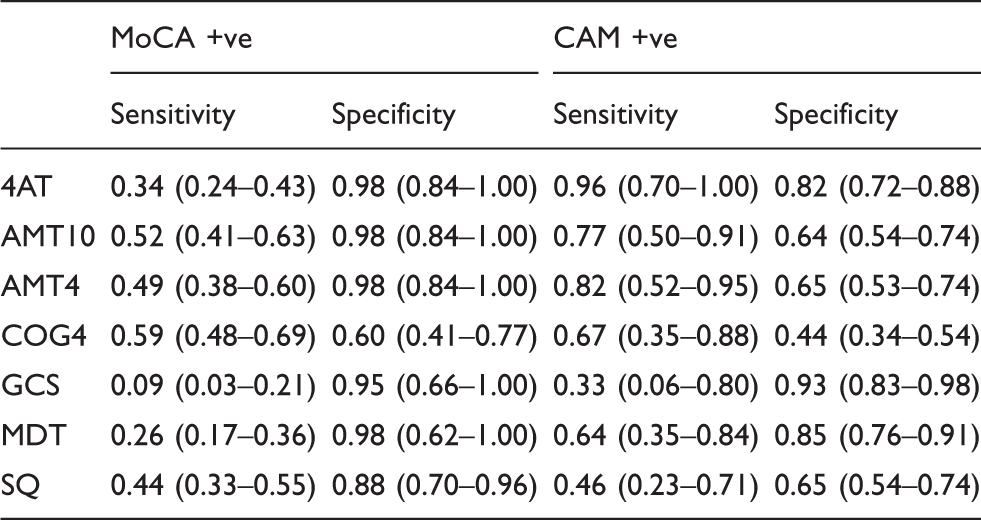
Introduction: National and international guidelines recommend screening for cognitive issues in acute stroke and various instruments are available. For routine use in a busy clinical environment, brief assessments would be preferred. We aimed to describe test accuracy of brief (less than 2 minutes) screening tools for diagnosis of cognitive impairment and delirium in acute stroke. Patients and methods: We collected data on sequential stroke unit admission in a city teaching hospital. Assessors were four students trained in cognitive testing. Brief assessments comprised: 10- point abbreviated mental test (AMT10); 4- point AMT (AMT4); 4-A test (4AT); Cog-4; Glasgow coma scale (GCS) and single question (SQ). We also recorded the multidisciplinary team’s informal review (MDT). We performed reference standard of Montreal cognitive assessment (MocA) and confusion assessment method for delirium (CAM) blinded to results of brief screening tests and using usual diagnostic cutpoints. We described sensitivity, specificity, positive and negative predictive values (PPV, NPV). Results: Over a 10-ten week period, 111 subject s were admitted; 102 had cognitive data. Subjects were 50% male (n=55); median age: 74 (IQR: 64–-85). The Cog4 test had greatest sensitivity for detecting cognitive impairment (0.59 [95% CI: 0.33–-0.69]) but poor specificity (0.6 [0.41–-0.77]). All other tests had sensitivity <0.5 and specificity >0.88. The 4AT had greatest sensitivity for detecting delirium (0.96 [0.70–-1.00]) and reasonable specificity (0.82 [0.72–-0.88]). Conclusions: Brief screening assessments are sensitive but not specific for detection of cognitive impairment and delirium in acute stroke. Our data suggest that 4AT is a reasonable choice for delirium screening but do not suggest an optimal test for routine cognitive screening in an acute stroke setting.
MoCA +ve
CAM +ve
Sensitivity
Specificity
Sensitivity
Specificity
4AT
0.34 (0.24–0.43)
0.98 (0.84–1.00)
0.96 (0.70–1.00)
0.82 (0.72–0.88)
AMT10
0.52 (0.41–0.63)
0.98 (0.84–1.00)
0.77 (0.50–0.91)
0.64 (0.54–0.74)
AMT4
0.49 (0.38–0.60)
0.98 (0.84–1.00)
0.82 (0.52–0.95)
0.65 (0.53–0.74)
COG4
0.59 (0.48–0.69)
0.60 (0.41–0.77)
0.67 (0.35–0.88)
0.44 (0.34–0.54)
GCS
0.09 (0.03–0.21)
0.95 (0.66–1.00)
0.33 (0.06–0.80)
0.93 (0.83–0.98)
MDT
0.26 (0.17–0.36)
0.98 (0.62–1.00)
0.64 (0.35–0.84)
0.85 (0.76–0.91)
SQ
0.44 (0.33–0.55)
0.88 (0.70–0.96)
0.46 (0.23–0.71)
0.65 (0.54–0.74)
PB24
Haemolysed Blood Samples Audit on patients in CAU, A&E and AAU
N Allen, T Sproat and A Strang
FY2, Forth Valley Royal Hospital, Larbert, UK
astrang@nhs.net
07790030886
Introduction: 1 in 10 samples sent to the lab will need to be repeated. This is a problem because it:
Causes delay in treatment and discharge of patients
Impacts on ED ‘“4- hour target-”
Is distressing to patients to have an unnecessary second invasive procedure
Has cost implications in terms of equipment and lab costs (80p per blood sample) and time (around 40 minutes to process)
Lab data shows that between 3000 and- 3500 samples are received from our front door areas per month. This equates to £280 per month or £3350 per year in repeat testing
Aim of study:
To identify why 1 in 10 samples haemolyse
To identify both practical and patient ‘“risk factors’”
To suggest ways in which the haemolysis rate could be reduced
Patients and methods:MethodsDevised a data set of 5 variables:
Method of collection i.e. needle/cannula, vacutainer/syringe, needle size.
Site of collection (hand/arm/leg) as the size of vein will vary
Volume of blood in the sample
Who took the bloods and from which department (CAU, AAU, ED)
Patient factors (Age, sepsis, etc.)
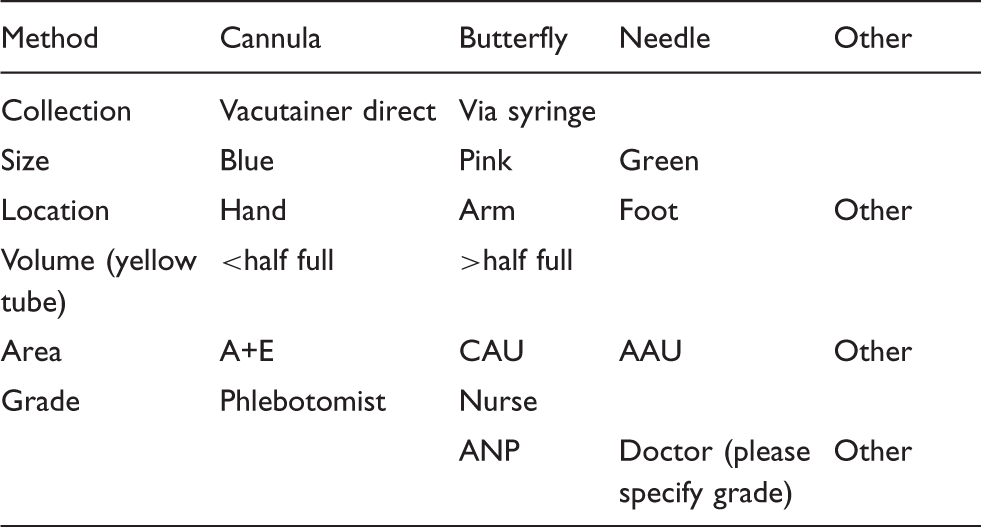
In order to collect relevant information, cards were made (included as appendix at top) –- staff asked to complete when they sent samples away
Patients
Patients requiring bloods in CAU, AAU or ED
Samples collected over a 3-week period
Results:
In total 191 samples received
Total haemolysis rate of 8.9%
11.4% from CAU, 7.01% from AAU, 9.1% from ED
Official lab data from same time showed average rate of 8.6%
Increased haemolysis rate with:
Cannula:14.8% haemolysis
Syringe: 22% haemolysis
More likely if sample under-filled (but why is sample under-filled?)
More likely with FY1’s (?more difficult to obtain blood)
Slightly more haemolysis with increasing age, 63.79 versus 69.82
Stage 2 of study
‘“Standardised technique’” and ‘“venesect before venflon’” policy
Repeat data collection stage for 1 week
Results
72 cards sent to the lab
Only 1 haemolysed
Haemolysis rate reduced from 11.3% to 1.3%in CAU
About one-a third of the people who had blood taken actually required a cannula after review of the case by senior clinician
Conclusions: We have identified various ‘risk factors’ for a blood sample to haemolyse. Taking blood using a syringe or from back a cannula or butterfly were the biggest predictors of haemolysis. Interestingly the manufacturers, BD, DO NOT recommend blood letting from a cannula. When we repaeated our study using a standardised technique (needle and vacutainer) only 1 sample was haemolysed.
Recommendations:
Blood should NOT be taken from the back of a cannula
Blood should be taken using a standardised technique using a needle and vacutainer whenever possible
References
Kennedy C, Angermuller S, King R, et al. A comparison of haemolysis rates using intravenous catheters versus venepuncture tubes for obtaining blood samples.RN, ADNColleen Kennedya, , staff nurses, RN, MEd, MSNSarah Angermullerb, staff nurse, instructor in the nursing program, RN, BSNRobin Kingb, instructor in the nursing program, RN, MSNSheri Noviellob, staff nurse, instructor in the nursing program, RN, ADNJoann Walkerb, staff nurses, RN, MSNJoanie Wardena, staff nurse, instructor in the nursing program and RN, MSNSusan Vangb, staff nurse, instructor in the nursing program. Journal of Emergency Nursing Volume 1996; 22:, Issue 6, December 1996, Pages 566–569.
For each of the 7 categories please circle one of the options
Method
Cannula
Butterfly
Needle
Other
Collection
Vacutainer direct
Via syringe
Size
Blue
Pink
Green
Location
Hand
Arm
Foot
Other
Volume (yellow tube)
<half full
>half full
Area
A+E
CAU
AAU
Other
Grade
Phlebotomist
Nurse
ANP
Doctor (please specify grade)
Other
PB25
Communication of DNACPR –- Raising the bar
Dr Ula J Chetty GP ST2 and Dr Graeme Simpson Consultant Geriatrician
Ward 5, Care of the elderly, ST1, Royal Alexandra Hospital, UK
ulachetty@hotmail.co.uk
07834717617/ 0141 560 2966
Introduction: Communication about resuscitation is a topical subject. Healthcare Improvement Scotland (HIS) carried out an inspection of elderly care in the RAH in March 2012. It concluded that decisions regarding DNACPR were documented without discussion with the relatives. This finding was widely reported in the media, but was based on just 2 DNACPR forms. Therefore, a larger sample of DNACPR forms were audited to see if the inspection result was a true reflection of practice. Patients and methods: All patient case notes in 5 care of the elderly wards were examined for DNACPR forms in May (cycle 1) and August 2012 (cycle 2). Audit criteria were created after reference to the DNACPR Scotland Policy. For each form, the following criteria were evaluated:
Which reason for DNACPR was selected
If there was a documented discussion with relatives
The presence of a consultant countersignature
The standard (Std) for each criterion was set at 100%.
After cycle 1, audit results and a discussion around key recommendations from the NHS Integrated Scotland Policy were presented at the RAH local medical meeting. Furthermore, HIS recommended that NHS Greater Glasgow and Clyde initiated mandatory training for all medical staff starting from July 2012.
Results: There were 28 DNACPR forms in cycle 1 and 31 in cycle 2 from a sample of 130 elderly patients.
A reason was documented in 100% forms in cycle 1 and 97% in cycle 2
There was a documented discussion with relatives in 71% forms cycle 1 and 58% in cycle 2
A consultant countersignature was present in 57% forms in cycle 1 and 74% in cycle 2
The vast majority of forms (89% cycle 1 and 77% cycle 2) had ‘“Resuscitation would be unlikely to be successful’” as the reason for DNACPR.
In cycle 2, There was an improvement in consultant countersignatures but deterioration of documented discussions with patient or relatives.
Conclusions: Cycle 2 results suggested that the completion of DNACPR forms was still suboptimal although not to the extent implied in the HIS report. Further training of all medical staff is essential in order to improve both written and verbal communication about resuscitation.
References
Healthcare Improvement Report, March 2012.DNA CPR Integrated Policy Scotland, May 2010.End Of Life Care Guidance, General Medical Council.Decisions relating to cardiopulmonary resuscitation, A Joint statement from the BMA, Resuscitation Council and the Royal College of Nursing, October 2007.
PB26
Aortic dissection in patients presenting with chest pain: Audit of the measurement of BP and pulse variation in a district general hospital
Lindsay EM Reid1 and Daniel J Beckett2
1ST3 in Acute Medicine, Acute Assessment Unit, Forth Valley Royal Hospital, UK
2Consultant in Acute and General Medicine, Acute Assessment Unit, Forth Valley Royal Hospital
Lindsay.reid@nhs.net
07968992959
Introduction: Aortic dissection is a rare but frequently fatal cause of acute chest pain. Early diagnosis and optimal management can increase 30-day survival to 90%.1. It has been shown that aortic dissections are more likely in the presence of the certain clinical features, including a variation in pulse and/or blood pressure (BP) (>20 mmHg between left and right arms). 1. The NICE guidelines state that a physical examination to look for signs of non-coronary causes of acute chest pain, such as aortic dissection, should be carried out in all patients presenting with chest pain.2 We aim to investigate what percentage of patients presenting with chest pain undergo BP and/or measurement in both arms. Patients and methods: We identified a cohort of patients with chest pain as those being referred to the Chest Pain Assessment Unit at Forth Valley Royal Hospital. This included patients from both the medical receiving unit and the emergency department. A retrospective review of the notes of all patients referred to the unit during a 2two-week period in February 2012 was undertaken. Results: We analysed a total of 47 cases. Only 19% of patients presenting with chest pain underwent BP measurement in both arms and/or evaluation of their pulses during clinical examination. Conclusions: Our study shows that blood measurement in both arms is not being conducted on a routine basis. This quick, non-invasive bedside test has been shown to aid the diagnosis of aortic dissection and should be a routine component of the clinical assessment in all patients presenting with chest pain.
References
Von Kodolitsch Y, Schwartz AG, and Nienaber CA (2000). Clinical prediction of acute aortic dissection. Archives of Internal Medicine: 2000; 160 (19): 2977.NICE Guideline CG95: Chest pain of recent onset, (March 2010).
PB27
Prescribing paracetamol in low weight patients
Dr Heidi Cook, Dr Matthew Greig and Dr Jillian MacFarlane
Dr Heidi Cook – FY1, Ward 1 & 2 (Respiratory Medicine), Aberdeen Royal Infirmary
Dr Matthew Greig - ST4, Ward 11 & 12 (Department of Medicine for the Elderly), Aberdeen Royal Infirmary
Dr Gillian MacFarlane – GPST2, A&E, Aberdeen Royal Infirmary, UK
heidi.cook1@nhs.net
07714 578 351
Introduction: Paracetamol is the most commonly used analgesic in Primary and Secondary care. The Greater Glasgow and Clyde acute therapeutics handbook now suggests a reduced dose of oral paracetamol for patients of low body weight (≤50 kg) to 15 mg/kg up to four times daily1.1 The dose of 500 mg four times daily is suggested. The objective was to audit the dose of paracetamol prescribed to patients who weigh ≤ 50 kg in a secondary care setting. Patients and methods: The audit was initially conducted in November 2011 and re-audited in February 2012. All patients weighing ≤ 50 kg in a care of the elderly hospital over a 1one -week period were identified. Drug charts were interpreted and doses of paracetamol and treatment regimes were extracted. Results: Cycle one identified 17 patients prescribed regular paracetamol and 8 prescribed as required paracetamol. Of these 35% (n=6) and 38% (n=3) respectively were prescribed an excessive dose. Cycle two identified 18 patients prescribed regular paracetamol and 17 prescribed as required paracetamol. Of these 28% (n=5) and 18% (n=3) respectively were prescribed an excessive dose. Conclusions: Patients weighing ≤ 50 kg continue to be prescribed more than the recommended dose of paracetamol. This could lead to morbidity and medico-legal implications. With increased awareness, we have shown that prescribing habits have improved, however room for improvement remains.
Reference
Therapeutics: A handbook for prescribing in adults. NHS Greater Glasgow and Clyde, 2011.
Experience of PET/CT in fever of unknown origin in North of Scotland
O Lloyd, M Peirse, R Laing, G Douglas, A Mackenzie and A Denison
Aberdeen Royal Infirmary, UK
Introduction: Fever of unknown origin (FUO) continues to be a diagnostic challenge and a final diagnosis may remain elusive in a significant number of cases.1 The aetiology of FUO can be broadly divided into: infections, autoimmune/inflammatory conditions, neoplasia and miscellaneous conditions.1 PET/CT is finding a role in diagnosing FUO after conventional laboratory and radiological investigations have failed to yield a diagnosis.2 Here we present our experience of PET/CT over the past 2 years in patients with FUO. Patients and methods: Patients referred from Aberdeen Royal Infirmary’s Infection Unit for PET/CT because of FUO over the preceding 2 years were identified from our local electronic PACS system and PET/CT paper records. A retrospective case note review was then undertaken to establish whether a diagnosis had been established, and if so, whether PET/CT had contributed to this diagnosis. Results: 11 patients underwent PET/CT for FUO in the preceding 2 years. 7 patients received a final diagnosis (64%). PET/CT aided the diagnosis in 4 cases (36%). The pathologies diagnosed were: giant cell arteritis (2 cases), sarcoidosis (1 case) and lymphoma (1 case). Of the 7 cases with a normal PET/CT, 5 cases remained undiagnosed (45%), 1 case subsequently declared itself as polymyalgia rheumatica and 1 case was diagnosed at post mortem as intravascular lymphoma. A normal PET/CT was highly reassuring in 4 cases (36%) without a diagnosis. PET/CT either contributed to the diagnosis or was normal in 8 cases (73%). Conclusions: Our findings show a rate of final diagnosis in FUO broadly inline with the literature. We have found PET/CT a useful modality. It has helped to secure a diagnosis in over half the cases achieving a final diagnosis, with the literature suggesting possibly even higher diagnostic rates.3 In those cases which remain undiagnosed it has reassured both the patient and physician that there is unlikely to be serious underlying pathology. As PET/CT continues to become more accessible, it should be considered early in the diagnostic algorithm after conventional investigations have failed to secure the diagnosis.3
References
Knockaert DC, Vanderschueren S and Blockmans D. Fever of unknown origin in adults: 40 years on. J Intern Med 2003; 253: 263–275.Qiu L and Chen Y. The role of 18F-FDG PET or PET/CT in the detection of fever of unknown origin. Eur J Radiol 2012. https://dx-doi-org.web.bisu.edu.cn/10.1016/j.ejrad.2012.05.025.Crouzet J, Boudousq V, Lechiche C, et al. Place of 18F-FDG-PET with computed tomography in the diagnostic algorithm of patients with fever of unknown origin. Eur J Clin Microbiol Infect Dis 2012. DOI: 10.1007/s10096-011-1440-6.
Documentation of chest radiograph interpretation in the acute setting
T Elswood and B Routledge
Forth Valley Royal Hospital, UK
Introduction: The Ionising Radiation (Medical Exposure) Regulations 2000 state that ‘100% of plain film examinations will have a written evaluation recorded in the notes by the clinician at a time when the evaluation will influence the management of the patient’. It is also good practice for clinicians to follow-up investigations that they request, and to record the date and time for every entry into patient notes. An audit was carried out in Forth Valley Royal Hospital (FVRH) regarding these three standards when applied to chest radiographs (CXRs). Patients and methods: 50 patients who passed through the Acute Admissions Unit (AAU) and received a CXR were audited over the course of 8 days. The following data were collected: patient demographics; the individual requesting the CXR; whether an interpretation was made in the patient’s notes; whether this was made by the requester; whether date and time were documented. Acute interpretations of CXRs were also correlated with the official radiologist’s report. Results: 84% of CXRs (85% day shift; 83% night shift) requested had an interpretation documented. Of these, 81% were interpreted by the requester. 17% of interpretations had a date and time documented. 33% of interpretations used potentially confusing terms such as ‘nil focal, (N), √’; 38% of interpretations did not correlate with the radiologist’s report. Of these, half were normal CXRs which had pathology documented by the clinician. Half were pathological CXRs which were documented by the clinician as having different or no pathology. One of the latter was reported as displaying potentially significant pathology. Conclusions: Acute CXR documentation in AAU, FVRH did not meet the three standards audited. A significant percentage of interpretations also used illegible or potentially confusing terms. Awareness of this, through presentations and posters in clinical areas, is being spread in the hospital. Regarding incorrect acute interpretations, a system is being implemented for liaison between radiology and AAU to ensure all CXRs are followed up following formal reporting. The audit cycle will be completed in August.
Stroke unit care in a real life setting: a case control analysis
P Fearon1, TJ Quinn1, D Stott1 and P Langhorne1
Clinical Research Fellow
1Academic Section of Geriatric Medicine, University of Glasgow, Glasgow UK.
patricia.fearon@glasgow.ac.uk
07816420015
Introduction: Clinical trials of stroke patients who receive organised inpatient stroke unit (SU) care have demonstrated improved survival, discharge home and functional outcome. We aimed to describe effects of SU implementation in routine clinical practice. Patients and Methods: Consecutive acute stroke presentations from a geographically defined population (East Glasgow, United Kingdom) were recorded between August 2000–July 2002 and August 2007–July 2010. Stroke patients managed prior to SU implementation (2000/01) were frequency matched with SU admissions in the year immediately after implementation (2001/02) and contemporary SU admissions (2008/10) for age, sex, pre-stroke dependency, stroke severity (Modified Rankin Score (mRS)) and Oxfordshire Community Stroke Project classification. Outcomes of interest were death censored at 30 days; discharge home and dichotomised mRS. Outcomes were assessed using proportional analysis across the three epochs. Further analysis compared combined SU groups with non-SU care. Results: After matching, 717 patients were included with equal numbers in each group. Patients in both SU groups were more likely to be alive at 30 days (94% (2001/02) and 95% (2008/10) versus 89% (2000/01); p=0.038). More patients in both SU groups were independent at discharge (mRS 0-2) (p<0.001) and were discharged home (p<0.001). The odds ratio for death or institutionalisation for combined SU group versus non-SU care was 0.70 (95% confidence interval (CI): 0.49 – 1.00). There was no significant difference in length of stay (mean difference 0.7 days (95%CI: -5.1-6.6). Conclusions: Implementation of organised inpatient stroke unit care in routine clinical practice appears to achieve similar outcomes to those seen in clinical trials.
Predictors of immediate imaging in suspected stroke
S White, TJ Quinn, C McAlpine and A Cameron
Specialist Trainee Medicine, West of Scotland Deanery
stwhite@doctors.org.uk
+44 7725 949 885
Introduction: National guidelines recommend immediate brain imaging for patients presenting with suspected stroke. However, access to computerised tomography (CT) scanning, particularly in the out-of-hours period, is a limited resource in many hospitals. We aimed to identify the predictors of immediate imaging based on the patterns of CT scanning in cases of suspected acute stroke. Patients and Methods: We reviewed emergency admissions to a single urban teaching hospital (Glasgow Royal Infirmary) over the two-year period 21st March 2010 to 20th March 2012 inclusive. Using the Emergency Department Information System, we identified patients coded as definite or suspected stroke. We recorded clinical and demographic variables including Manchester triage category, routine observations including GCS, and grade of assessing doctor. We cross-referenced this group against the Picture Archiving and Communication System database and calculated time from presentation to brain imaging. Imaging was considered immediate if performed before leaving the initial assessing unit. We used a multiple logistic regression analysis to determine the factors associated with immediate scanning. Results: Of 780 total suspected stroke presentations (ED=559; AAU=221), 38.3% (299) had immediate imaging. The median waiting time was 1.7 hours for immediate scanning versus 20.7 hours for those scanned after admission to the ward. Patients with higher triage category were more likely to have immediate scans than those in lower triage groups. Other associations with immediate scanning were initial review by consultant, with odds ratio 3.82 (95% CI 1.4-10.39), arrival during office hours (OR 2.55, 95% CI 1.79-3.64), and a firm clinical diagnosis of stroke (OR 1.95, 95% CI 1.33 to 2.85). Conclusions: A significant number of patients presenting with probable acute strokes have delayed CT imaging. While the sickest patients and those with the most obvious clinical strokes are usually scanned promptly, our data suggest that non-clinical factors such as out-of-hours scans and seniority of assessor are also important, and may be targets for reducing waits for CTs.
Adjuvant use of 131I-MIBG in phaeochromocytoma and paraganglioma at high risk of malignancy
MA Rutherford1, AJ Rankin2, TM Yates3, NS Reed4, CG Perry5 and EM Freel5
1Glasgow Royal Infirmary, UK
2University of Glasgow, UK
3NICU, Royal Hospital for Sick Children, UK
4Beatson West of Scotland Cancer Centre, UK
5Western Infirmary Glasgow, UK
Introduction: Phaeochromocytomas and paragangliomas are rare catecholamine producing tumours. It can be difficult to predict their malignant potential and patients can sometimes present with metastatic disease many years after their original diagnosis.1 As a result, we offer a single dose of adjuvant 131I-Metaiodobenzylguanidine (131I-MIBG) to subjects felt to be at higher risk of local recurrence (demonstration of capsular or vascular invasion on pathology). However, there is a lack of evidence supporting this practice and concern regarding the safety and tolerability of such therapy. We therefore aimed to review outcomes of cases of adjuvant 131I-MIBG use in patients judged at ‘high risk’ of recurrent/malignant disease. Patients and methods: We reviewed the case notes of patients who received 131I-MIBG on an adjuvant basis from 1985 to 2010. Patients with metastatic disease at the time of treatment were excluded. Disease recurrence was assessed by 131I-MIBG scintigraphy, computed tomography/magnetic resonance imaging, biochemical measurement of catecholamines and symptom recurrence. Results: Fourteen patients (8 male) were reviewed. Mean age was 37 years (range 9–79). One patient was receiving an alpha blocker and one patient both beta and alpha blockade during treatment. All had undergone surgical resection prior to 131I-MIBG therapy. Indications for therapy were capsule breach, local nodal spread/vascular invasion or local recurrence. One patient received 131I-MIBG due to a strong family history of malignant disease. Each patient received one dose of 131I-MIBG; mean dose 9166 megabecquerel (MBq), range 5180–10,353 MBq. The treatment was largely well tolerated with no haematological sequelae. One patient (7%) developed recurrent disease and one patient died due to disease progression. Follow-up is ongoing for the rest of the cohort with no evidence of recurrent disease. Conclusions: Adjuvant 131I-MIBG treatment of phaeochromocytoma/paraganglioma is well tolerated and routine use of alpha/beta blockade during therapy is not required. These data support its use in an adjuvant basis to prevent progression to metastatic disease in patients thought to be at risk of malignant disease however lack of a control group prevents firm conclusions.
Reference
Chrisoulidou A, Kaltsas G, Ilias I, et al. The diagnosis and management of malignant phaeochromocytoma and paraganglioma. Endocrine-Related Cancer 2007; 14: 569–585.
Acute asthma – Assessing understanding of junior medical and nursing staff
ADL Marshall1, P Wilson2 and GP Currie2
1Aberdeen Royal Infirmary, Aberdeen, UK
2Gilbert Bain Hospital, Shetland, UK
Introduction: Acute asthma is a common cause of presentation to emergency departments and carries a low but significant risk of death. Gilbert Bain Hospital is a remote and rural hospital located in Shetland and junior staff may have limited experience of dealing with acute asthmatic patients. Patients and methods: We used a 13-point questionnaire to assess awareness of current guidelines and knowledge of assessment and management of acute asthma. This was distributed to 32 members of staff consisting of 8 junior doctors, 21 nurses and 3 medical students. Results were submitted anonymously. Results: 86% of responders were aware that a national guideline was available and 71% had read them. Only 19% felt confident in assessing the severity of an asthma exacerbation and 47% would always check peak flow (PF). 81% and 63% of responders felt incorrectly that arterial blood gases (ABG) and chest x-ray respectively were essential for assessment. 84% felt oxygen should be administered routinely and only 13% identified the correct target oxygen saturation range based on current BTS guidelines. 100% would use bronchodilators and 81% steroid while 19% administer antibiotics as routine treatment. With regards to preparation of drugs, 88% were confident in preparing nebulised salbutamol compared with 50% and 16% when preparing intravenous salbutamol and magnesium respectively. 88% felt local guidance in assessment and management of acute asthma would be useful. Conclusions: Despite national guidelines, many frontline medical and nursing personnel in a remote and rural hospital had limited knowledge of the optimal way of assessing and treating patients with acute asthma. Further education is required and a need for readily available local guidance has been identified.
The cost of blood tests on acute medical admissions: A single centre experience
R Ball1, H Rehman1 and A Cameron2
University of Glasgow, UK
Glasgow Royal Infirmary, UK
Introduction: Patients presenting to hospital with acute medical problems often have a range of blood tests taken to aid in their assessment. However, in these times of financial austerity, clinicians must take some corporate responsibility for ensuring cost-effective use of laboratory resources. We therefore aimed to measure the cost-effectiveness of the ‘routine’ bloods taken in medical receiving. Patients and methods: In this prospective study we took an electronically randomised sample of all presentations to the medical Acute Assessment Unit (AAU) at Glasgow Royal Infirmary. Details of the presentation, the blood tests requested, the adherence of blood testing to local guidelines and the presence of abnormalities were recorded. We also determined whether the results of each blood test altered subsequent investigations or treatment. These data were combined with the marginal cost of each blood test to determine the cost per change in management for each laboratory test. Results: 786 blood tests were performed on 109 patients. The most cost-effective blood tests, CRP and FBC, cost £4.22 and £6.13 per change in management, respectively, while the least cost-effective, LFTs and coagulation screens, cost £321.00 and £147.42. Increasing age was found to correlate with an increase in likelihood of a blood test leading to a change in patient management (odds ratio 1.023 ± 0.014, p= 0.0015). Conclusions: We demonstrate that ‘routine’, ‘cheap’ blood tests can actually be very expensive in terms of value for money, and in particular LFTs and coagulation screens are poor value for money if they are not carefully restricted to appropriate patient groups. Serious consideration should be given to tailoring blood tests more appropriately to presenting complaint in medical receiving, particularly in younger and otherwise well patients.
Diagnosis and management of pituitary apoplexy: A case series from a district general hospital
LEM Reid, N Barwell, C Kelly and L Buchanan
Forth Valley Royal Hospital, UK
Introduction: Headache is a common presenting symptom to the acute medical receiving unit. Pituitary apoplexy is a rare cause of such a presentation, but is both a medical and ophthalmologic emergency. Patients and methods: We retrospectively reviewed the case notes of six patients presenting with pituitary apoplexy to Forth Valley Royal Hospital over a 5-year period. Results: The demographics, past medical history, presentation, investigation and management of the 6 cases are summarised. Conclusions:
A high index of suspicion is required for the diagnosis of pituitary apoplexy – our series highlights that it does present to DGHs and often occurs in patients with no clear precipitating factors.
Common presenting symptoms are headache, visual disturbance, vomiting and meningism. Eighty per cent of patients have a hormonal abnormality at the time of presentation1.
MRI is the imaging modality of choice, and identifies the diagnosis in 90% of patients (compared to 28% for CT).1 In this study, one CT scan and one MRI were initially mis-reported as having no pituitary abnormality. The radiologists should be specifically requested to review the pituitary, and there should be a low threshold for further referral to the neuroradiology team.
Our series suggests that conservative management in a DGH with close monitoring is an acceptable treatment option in stable patients with no/mild visual impairment.
Reference
UK guidelines for the management of pituitary apoplexy. Pituitary apoplexy Guidelines Development Group: May 2010. Clin Endocrinol 2011; 74: 9–20.
Patient satisfaction in the acute assessment unit: comparison to the emergency department
M Penton, J Blackburn, A Cameron and G McKay
Acute Medical Unit, Glasgow Royal Infirmary, UK
Introduction: An Acute Assessment Unit (AAU) was opened in March 2011 as part of the modernisation of acute hospital services in the North-East of Glasgow allowing GP referrals to bypass the Emergency Department (ED) and be seen in a custom built facility by nurses and physicians with specialist training in acute medical care. We aimed to assess patient satisfaction with this new model of care as compared to those admitted through the ED. Patients and methods: A modified version of the Scottish Inpatient Patient Experience Survey1 was administered over a one week period to a random sample of patients admitted through the AAU or ED and completed anonymously after being moved from the respective units. A fixed proportion of admissions (20%) were identified from each day, ensuring busy days were not under-represented. A power calculation suggested approximately 60 responses were needed to detect a 1-point shift on the Likert scale for each question with statistical analyses done using the Mann–Whitney U-test. Results: 51 patients (AAU, n=22; ED, n=29) gave responses to a total of 33 questions covering all aspects of care including adequacy of information provided, time to assessment and admission, adequacy of care, maintenance of privacy and overall satisfaction. There were no significant differences in the distribution of any of the answers in patients admitted from AAU compared to ED. The majority of responses to each statement were positive (‘strongly agree’ or ‘agree’). Conclusions: Despite differences in layout, approaches, durations of stay and functions of the AAU and ED we have shown that patient satisfaction with care is similar. The positive responses suggest that patients were satisfied with their care regardless of route of admission. The modified Scottish Inpatient Patient Experience Survey represents a useful tool that could be used longitudinally within both the AAU and ED to ensure that the quality of care is maintained.
Role of urinary dopamine in investigation of phaeochromocytoma/paraganglioma
C Smith1, M Freel1, C Perry1, F Davidson2, K Smith3 and Y Tautphaus4
1Western Infirmary, UK
2Crosshouse Hospital, UK
3Glasgow Royal Infirmary, UK
4University of Lubeck, Germany
Introduction: There is controversy over which form of biochemical testing is best for screening for phaeochromocytoma/paraganglioma (PHAEO/PGL).1 Measurement of plasma metanephrines is the most sensitive test but is less specific and lacks widespread availability, and so many centres opt to measure 24-hour urinary excretion of catecholamines and metanephrines. However, the standard 24-hour urinary catecholamine profile also includes dopamine (DA), VMA and HVA. The aim of the current study was to determine the additional value of measuring urinary DA in the diagnosis of PHAEO/PGL by reviewing patients who had elevated DA in isolation. Patients and methods: We reviewed 2161 (1118 cases) 24-hour urinary catecholamine profiles analysed by HPLC and electrochemical detection at Crosshouse Hospital, Ayrshire between 2007 and 2010. We then reviewed the cases where an isolated DA elevation was seen. Results: Ninety-one samples (4.2%) demonstrated an elevation in 24-hour urinary DA, which corresponded to 51 cases (4.6%). 18 cases (1.6%) demonstrated elevated urinary DA in isolation. None of these had current evidence of PHAEO/PGL. Conclusions: Elevated 24-hour urinary DA excretion in isolation is unusual and of the cases we identified, there was no situation where this was of clinical relevance. These data would support the removal of urinary dopamine from the conventional urinary catecholamine profile (unless there is high suspicion of a DA secreting PGL) as in our series it had no impact on diagnostic yield and may lead to unnecessary investigations.
Reference
Peatson RT and Ball S. Biochemical detection of phaeochromocytoma: why are we continuing to ignore the evidence? Ann Clin Biochem 2008; 45(1): 6–10.
Syncope and driving recommendations
Ulf Neisius
Forth Valley Royal Hospital, UK
Introduction: According to the European Society of Cardiology syncope is defined as ‘a transient loss of consciousness due to global cerebral hypoperfusion characterised by rapid onset, short duration and spontaneous complete recovery’.1 Current DVLA guidelines require a 6 months driving ban in case of a solitary loss of consciousness likely to be cardiovascular in origin and unexplained by reflex vasovagal syncope. The implementation of those guidelines in clinical practice was investigated in Forth Valley Royal Hospital, Larbert. The audit loop was closed after an education and information campaign. Patients and methods: The local online database for discharge letters was search over 61 days for patients registered with a diagnosis suggestive of syncope. To improve the percentage of letters containing driving recommendations, lectures for junior and middle grade doctors were given, the topic was highlighted during and MDT meeting and information material was provided in the acute assessment unit. The effect was measured by screening discharge letters of a 30 days period. Results: During the 2 months period, in at least 21 cases (33% of all syncope patients) driving recommendation would have been required. Of those 44 patients were discharged from the receiving unit and 19 patients were admitted to hospital wards. In 1 case a written advice was given. After the education and information work, at least 14 cases (45% of all syncope patients) required recommendations. Of those 22 patients were discharged from the receiving unit and 9 patients were admitted to a hospital wards. Such were given in 5 patients (36%). This number of recommendations was statistically significant different (p=0.03) in comparison to the baseline period. Conclusions: A certain number of patients admitted with syncope require driving recommendations. The number of those as documented in discharge letters can be increased by educational and information measures.
Reference
Task Force for the Diagnosis and Management of Syncope; European Society of Cardiology (ESC); European Heart Rhythm Association (EHRA); et al. Guidelines for the diagnosis and management of syncope (version 2009). Eur Heart J 2009; 30(21): 2631–2671.
The use of abbreviations and acronyms in medical documentation
C. Smith1 and Robynne Struthers name>2
1Specialty Registrar, Western Infirmary, UK
2Foundation Doctor, Western Infirmary
Introduction: In typical busy receiving units, clear written documentation is vital for communication between different members of the multidisciplinary team. If medical staff use abbreviations not universally understood by the multidisciplinary team then this will lead to potentially dangerous miscommunication and misinterpretation. We wanted to study the frequency of abbreviations in medical documentation. We also wanted to assess how well understood abbreviations are by those who are using medical documentation. Patients and methods: We selected 40 case sheets at random from medical wards including the acute receiving unit and listed the abbreviations used in ‘“clerk-ins’” and consultant entries. Twenty abbreviations were selected to assess what different groups of health professionals understood by them. Results: We found 125 different abbreviations and acronyms in the case sheets we studied. Of the 20 abbreviations tested: Medical students got an average correct score of 15.5/20 (77.5%); staff nurses average score was 13.75/20 (68.8%); foundation doctors average score was 18.75/20 (93.8%); therapists average score was 10.3/20 (51.7%). Conclusions: We ha’ve shown that abbreviations are commonly used in medical notes. Notably professionals relying on these documents, like nurses and therapists, do no’t necessarily know these abbreviations. Interestingly, doctors in training do no’t know all the abbreviations. It would appear they are learnt when starting professional life as foundation doctors. We would discourage the use of abbreviations/acronyms based on our results.