
Abstract
Background
Investigation and management of neonatal heart murmurs varies widely and is dependent on local resources. In order to standardise the management of heart murmurs in our hospital a guideline (based on clinical examination with selective cardiology review) was introduced.
Aims
To establish adherence to and safety of the guideline; to review workload implications and to define the causes of neonatal heart murmurs in our population.
Methods
Patients were prospectively identified over a 2-year period (August 2006 to July 2008). Case notes were reviewed and examination findings, investigations, follow up and diagnosis recorded.
Results
89 babies were identified. The guideline was generally well adhered to. In total 51 (57%) of babies were referred for cardiology assessment. In 40 babies this assessment included an echocardiogram. 30 babies (34%) had an underlying cardiac malformation: 25 were identified before discharge home. 15/30 (50%) of the babies with a cardiac malformation remain under cardiology follow up at the age of 1 year. No baby discharged from follow up without cardiology review subsequently presented with a cardiac problem.
Conclusion
A significant minority of babies with a heart murmur have an underlying cardiac malformation. Our guideline appears to ensure the timely identification of these babies and rationalises our use of specialist services.
Keywords
Introduction
Heart murmurs are one of the more common ‘abnormalities’ detected at routine newborn examination. Whilst it is recognised that not all babies with congenital heart disease will have a heart murmur and that some murmurs may reflect normal neonatal cardiovascular adaptation, the presence of a heart murmur can be an important clue to an underlying cardiac malformation. The clinical challenge is to identify those murmurs which are significant.
In the United Kingdom, there are currently no national guidelines for the management of neonatal heart murmurs. Investigation varies widely and is often dependent on local resources. The Queen Mother’s Maternity Hospital in Glasgow was co-located with the Royal Hospital for Sick Children. A cardiology opinion, and echocardiogram if necessary, could be obtained the same day. Prior to 2006 there was no guideline for the management of neonatal heart murmurs and management varied widely depending on the previous experience of the examining doctor. The perception was that a large number of babies were being referred to cardiology, many of whom had normal hearts. In 2006 a guideline was introduced which was based on clinical examination and selective cardiology review (Figure 1). This was designed to ensure safe management of neonatal heart murmurs whilst not overwhelming the cardiology department with unnecessary referrals.
The Queen Mother’s Hospital Murmur Guideline.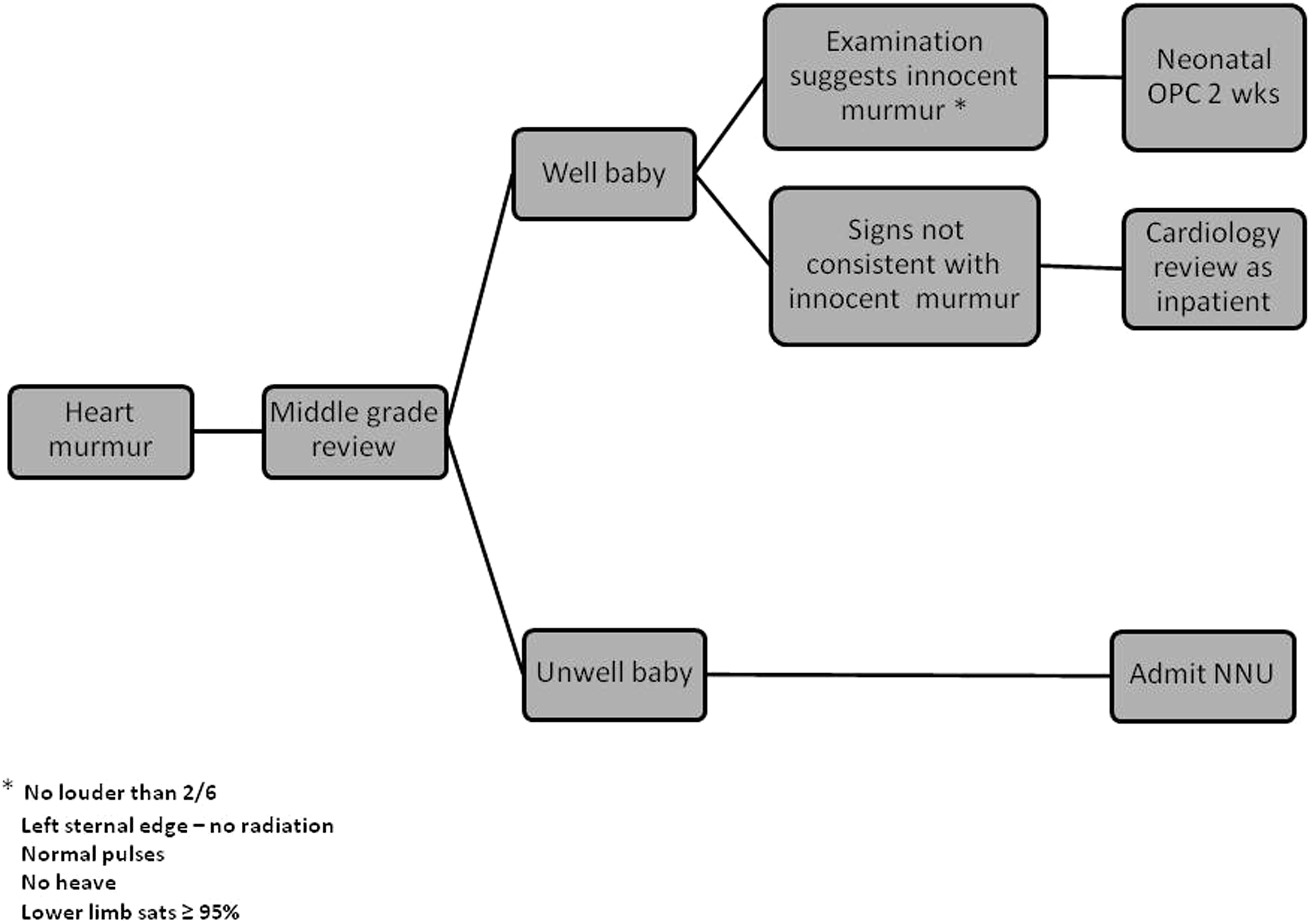
Aims of audit
The primary aims of the audit were to establish adherence to the new guideline and, as there is no consensus about the management of neonatal heart murmurs, to establish the safety of the guideline. In doing so we were also able to define the causes of heart murmurs in our population, establish the age at diagnosis and to quantify workload implications for both the neonatology and cardiology departments.
Methods
Patients were prospectively identified over a 2-year period (August 2006 to July 2008). Postnatal ward SHOs were asked to complete an audit proforma for each baby in whom they heard a heart murmur. In order to ensure complete capture of all babies with heart murmurs this list was cross referenced with several other sources including neonatal outpatient clinic lists, the neonatal unit admission book and the cardiology database. The medical records were subsequently reviewed to ascertain examination findings, investigations, initial follow up, final diagnosis and outcome at 1 year.
Results
Eighty-nine babies were identified with heart murmurs from August 2006 to July 2008 (1.3% of live births).
Adherence to guideline
Eighty-five (96%) babies were reviewed by a middle grade or consultant paediatrician. Lower limb saturations were recorded in 64 (72%) babies. The majority of babies did not have any other investigations performed by neonatal staff with the exception of two babies who had a four limb blood pressure, one baby who had a chest x-ray and five babies who had an electrocardiogram. There were 30 babies whose documented examination findings were not consistent with an innocent murmur of whom 27 (90%) were referred to cardiology as an inpatient. Of the 58 babies who had neonatal follow-up appointments arranged, 51 (88%) had a 2-week appointment with the remainder having appointments scheduled for 3 to 6 weeks post discharge.
Safety of the guideline
25/30 (83%) babies with congenital heart disease were diagnosed prior to discharge home. Those diagnosed after discharge included four babies referred to cardiology from neonatal outpatient clinic (two ventricular septal defects, one atrial septal defect and one mild aortic stenosis) none of whom have required any intervention and a baby with hypoplastic left heart syndrome who presented to the Emergency Department at the age of 8 days. On review of this baby’s notes it was apparent that the clinical findings at the time of newborn examination were not consistent with an innocent murmur and the fact that this baby was allowed home without cardiology review was a deviation from the guideline. No baby who was discharged from follow up without cardiology review subsequently presented with a cardiac problem.
Cause of murmurs
57/89 (64%) of the murmurs were innocent (Figure 2). Two babies defaulted from follow up. In 30 babies (34%) the murmur was associated with an underlying cardiac malformation, the most common of which was a ventricular septal defect (20 babies). The majority of heart defects were not life threatening and did not require immediate intervention with the exception of a baby with critical pulmonary stenosis who underwent balloon valvuloplasty on day two and the baby with hypoplastic left heart who underwent a Norwood procedure.
Cause of heart murmurs.
Workload implications
51/89 (57%) babies were seen by cardiology at some point: in-patient referral (30); referral from neonatal outpatient clinic (18), emergency department presentation (1); self-referral (1); GP referral (1). The majority of babies reviewed by cardiology (59%) had an underlying cardiac malformation. 40/89 (45%) of babies had an echocardiogram at some point as part of the assessment of their murmur. 55/89 (61%) babies attended a neonatal outpatient appointment of whom 51 (93%) had innocent murmurs.
Age at diagnosis
25/30 (83%) babies with congenital heart disease were diagnosed prior to discharge home. Of the babies with innocent murmurs, 40/57 (70%) had the diagnosis confirmed by 6 weeks but 11(19%) were over 10 weeks old with three babies being over 6 months of age before diagnosis.
1-year follow-up data
In 15/30 (50%) of the babies with congenital heart disease the abnormality had resolved and they have been discharged. 15/30 (50%) remain under cardiology follow up of whom three have required surgery or catheter intervention. Of the 36 babies who were discharged without cardiology review, 32 (89%) are alive and well at 1 year with no known cardiac problems. Four babies could not be traced.
Discussion
It is recognised that newborn clinical examination as a screening test for the detection of congenital heart disease has low sensitivity. 1 However, the presence of a neonatal heart murmur has been reported to be associated with congenital heart disease in up to 75% of cases. 2 In our population, 34% of babies with heart murmurs had congenital heart disease. The optimal investigation of neonatal heart murmurs is still debated with practice varying widely, including chest x-rays, electrocardiograms, pulse oximetry, four limb blood pressure monitoring and echocardiography. Our guideline is based on clinical examination which has been shown to be effective in identifying pathological murmurs with grade, quality, location and timing of the murmur being highly significant. 3 Universal saturation monitoring has been proposed as a screening tool for congenital heart disease in the hope that this will increase the sensitivity of clinical examination alone and help identify those infants with a duct-dependent circulation before they collapse. 4 Although we have not adopted this as a policy in our hospital it seemed prudent to measure lower limb saturations in babies with a heart murmur.
The guideline was generally well adhered to with the exception of documentation of saturations. Almost all of the babies were reviewed by a senior paediatrician and the vast majority of the babies with findings not consistent with an innocent murmur were reviewed by cardiology prior to discharge. Consequently, babies in whom the murmur was associated with congenital heart disease were usually diagnosed before discharge home. It is disappointing that the only baby with a duct-dependent systemic circulation was discharged home before diagnosis. As already mentioned, this represents a deviation from the guideline rather than a guideline failure. Importantly, the parents had been advised of the warning signs to look for and to seek urgent medical advice if the baby became unwell, which they subsequently did. Interestingly, this baby had normal lower limb saturations at neonatal examination, which supports the finding that screening with pulse oximetry will still miss some left heart obstructive lesions. 4
Use of the guideline splits the workload evenly, with cardiology services appropriately seeing a higher proportion of significant murmurs. Of the babies discharged from follow up without cardiology review none subsequently presented with a cardiac problem.
This audit enabled us to identify some areas for service development. As a number of babies with heart murmurs are discharged home without a definitive diagnosis it is essential that parents are able to recognise warning signs and know who to contact if their baby becomes unwell. We have therefore designed a written information leaflet for parents to take home. Although most babies with congenital heart disease were diagnosed prior to discharge home, babies with innocent heart murmurs often had to wait several weeks or months before the diagnosis was confirmed. As these are well babies this is not a clinical problem but the delay in diagnosis could potentially lead to increased stress and anxiety for parents. A new, streamlined referral process has therefore been introduced which allows babies seen at neonatal outpatient clinics and thought to require cardiology review to be seen the same day at a cardiology clinic. This should ensure that all babies with heart murmurs will have a diagnosis by the age of 3 weeks.
This audit has shown that adherence to the guideline identifies murmurs, which require further investigation, ensuring the timely diagnosis of those murmurs which represent underlying cardiac disease and rationalises our use of specialist services. Although in our hospital we are fortunate to have access to paediatric cardiology services we believe that our guideline could also be used in units with a paediatrician/neonatologist with expertise in cardiology who has echocardiography skills or in hospitals with access to cardiology telemedicine links.
Footnotes
Acknowledgements
The authors thank Sister Rhona Robinson, Queen Mother’s Hospital, Glasgow and Lorraine Leask, Department of Cardiology, Royal Hospital for Sick Children, Glasgow, for their assistance.
Declaration of conflicting interests
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.