
Abstract
Introduction
Lemierre’s syndrome is a potentially fatal condition characterised by spread of an oropharyngeal infection, resulting in thrombosis of the internal jugular vein. This leads to septicaemia and possible metastatic abscesses.
Case presentation
We discuss the case of a previously healthy 17-year-old male who developed Lemierre’s syndrome following dental sepsis. He presented with bilateral submandibular and submental swelling extending into the neck and chest. His management included a tracheostomy; incision and drainage of the abscesses; drainage of a pleural effusion and prolonged anticoagulant therapy.
Conclusion
The incidence of Lemierre’s disease appears to be increasing and early diagnosis is essential. A high index of suspicion is needed in cases of oropharyngeal infection followed by fever, tender swelling of the neck and dysphagia – especially in young patients.
Introduction
Lemierre’s syndrome, as described in his 1936 paper, 1 is a condition characterised by thrombosis of the internal jugular vein resulting from spread of infection from the oral cavity or pharynx. This leads to septicaemia, and often septic emboli which commonly impact in the lungs.
Of the 20 patients Lemierre observed, the condition proved fatal in all but two. The prognosis has improved since the widespread use of antibiotics, but death still occurs in around 5% of cases. 2 Classically, the condition affects young otherwise healthy adults and is caused by anaerobic bacteria – most frequently Fusobacterium necrophorum. 3
Despite being rare (one study reporting 0.8 cases per million per year 4 ), Lemierre’s syndrome is important to consider in cases of oropharyngeal infection as prognosis is dependent on early diagnosis and appropriate treatment. 5
Case presentation: medical history, clinical features
We present the case of a 17-year-old male who was referred to the maxillofacial department with a 2-day history of bilateral submandibular and submental swelling extending into the neck and chest.
At presentation, he complained of being unable to swallow his saliva, and pain associated with the swelling. A history of toothache from his lower right second molar was noted. The past medical history was unremarkable.
Clinical examination revealed fluctuant bilateral submandibular swellings, the left side being more pronounced. Marked submental space swelling was also noted. The floor of mouth was raised bilaterally, once more the left causing most concern. His temperature (aural) was 36.4°C; blood pressure 119/66 mmHg; heart rate 118; and respiratory rate 14.
Investigations
Of particular note from the blood results were the elevated white cell count of 19.9 × 109/L and C-reactive protein (CRP) of 497 mg/L. Based on these findings, the presence of sepsis was identified and intravenous co-amoxiclav and metronidazole were commenced.
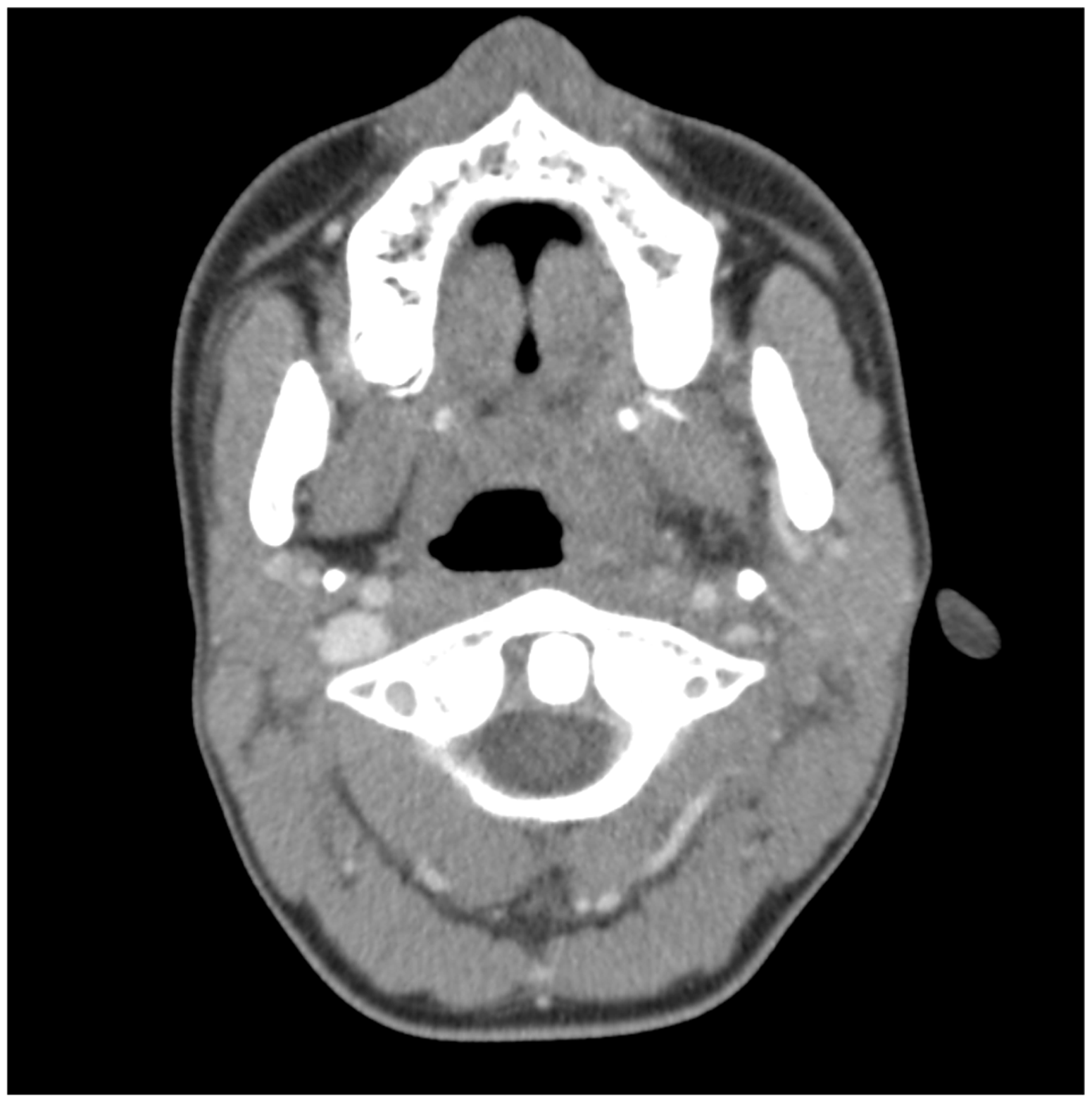
A dental panoramic radiograph (Figure 1) confirmed the lower right second molar to be the likely source of infection. A computed tomography (CT) scan with contrast revealed a large submental collection and a very swollen left submandibular salivary gland. Multiple locules of collection extended into the left parapharyngeal space; with a prevertebral collection from C1 to C7. Furthermore, left internal jugular vein thrombosis was noted from its origin to C1 (Figure 2).
Dental panoramic radiograph demonstrating caries and periapical area associated with lower right second molar tooth. CT scan at level of C1 demonstrating left internal jugular vein thrombosis and left parapharyngeal / prevertebral collection.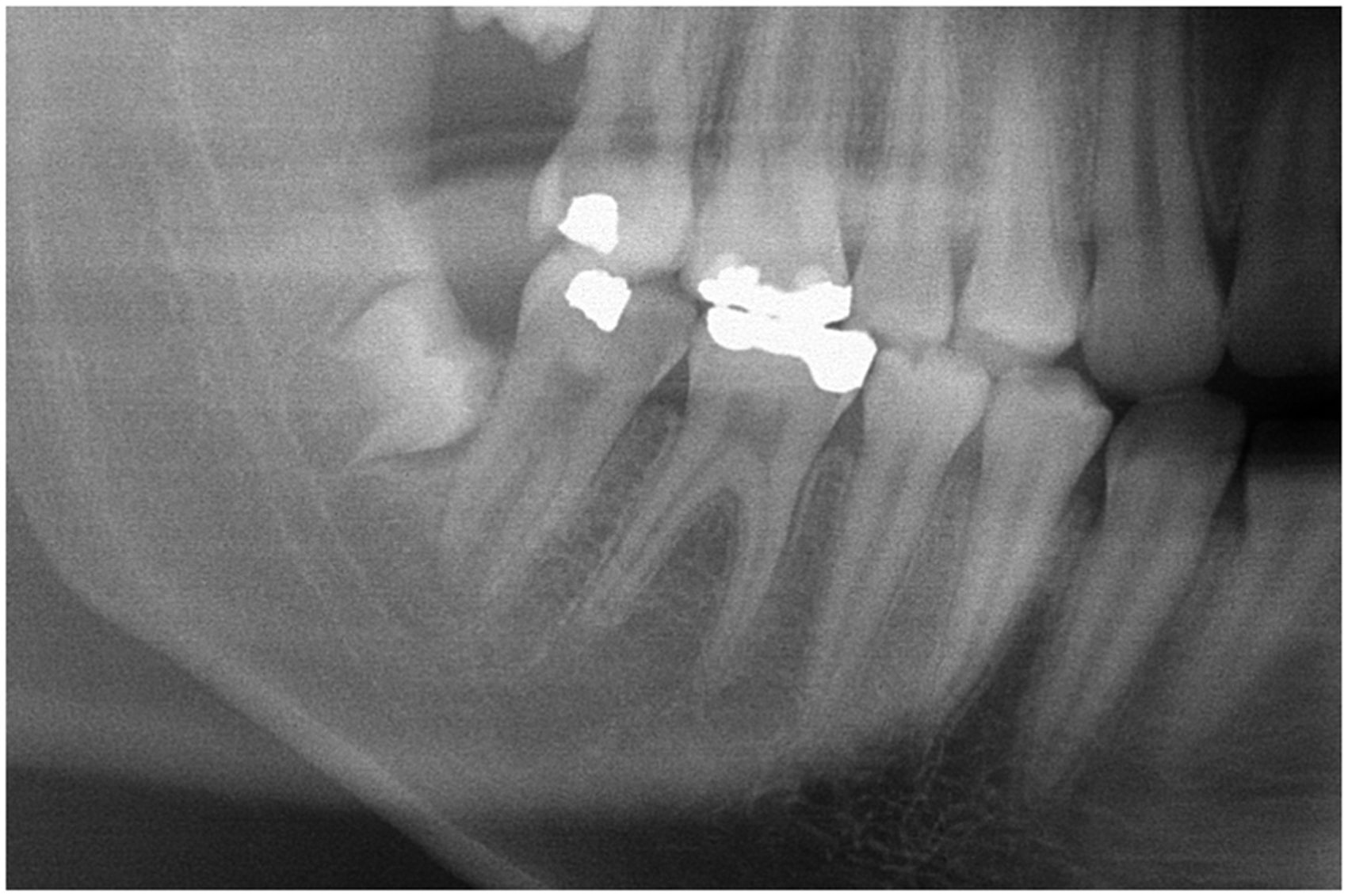
Differential diagnosis
Given the history and presentation, dental sepsis was by far the most likely diagnosis. As such, the differential diagnosis consisted of either dental sepsis or Lemierre’s syndrome associated with dental sepsis.
Treatment
The patient underwent emergency surgery to secure the airway via tracheostomy; extract the lower right second molar; and incise and drain the abscesses. The intravenous antibiotics started previously were continued.
Operative findings
Exploration of the left and right submandibular, submental and parapharyngeal spaces revealed large quantities of pus. In addition, the left prevertebral space was explored via blunt dissection anterior to the sternocleidomastoid reaching between the internal jugular vein and carotid artery. A further collection of pus was drained which filled a cavity 5 cm deep. Five drains were placed and the patient was monitored closely in the intensive therapy unit (ITU) for 3 days. Microbiological analysis of the pus samples revealed Streptococcus anginosus to be the most likely causative organism.
Outcome, prognosis and follow-up
During recovery, paresis of the left hypoglossal nerve was identified. Upon discharge from ITU, a thrombophilia screen was organised and reported no abnormalities. Treatment dose low molecular weight heparin was commenced given the internal jugular vein thrombosis. A second CT with contrast of the head and neck revealed continued thrombosis of the left internal jugular vein to its junction with the subclavian vein, but no extension intracranially. Some oedema of the superior mediastinum was noted.
Six days after leaving ITU, the patient was recovering well with the CRP falling accordingly. However, he began to complain of pleuritic chest pain localised to the base of the left lung. A chest X-ray showed consolidation and effusion in this region: the differential diagnosis included a septic pulmonary embolus or hospital acquired pneumonia with para-pneumonic effusion. A CT pulmonary angiogram (Figure 3) was carried out reporting: a large left-sided pleural effusion; fluid collection in the superior mediastinum and an enlarged main pulmonary artery. However, no evidence of a pulmonary thromboembolus was present. Based on the suggestion of an enlarged pulmonary artery, a transthoracic echocardiogram was performed which revealed no abnormalities.
CT pulmonary angiogram demonstrating large left-sided pleural effusion.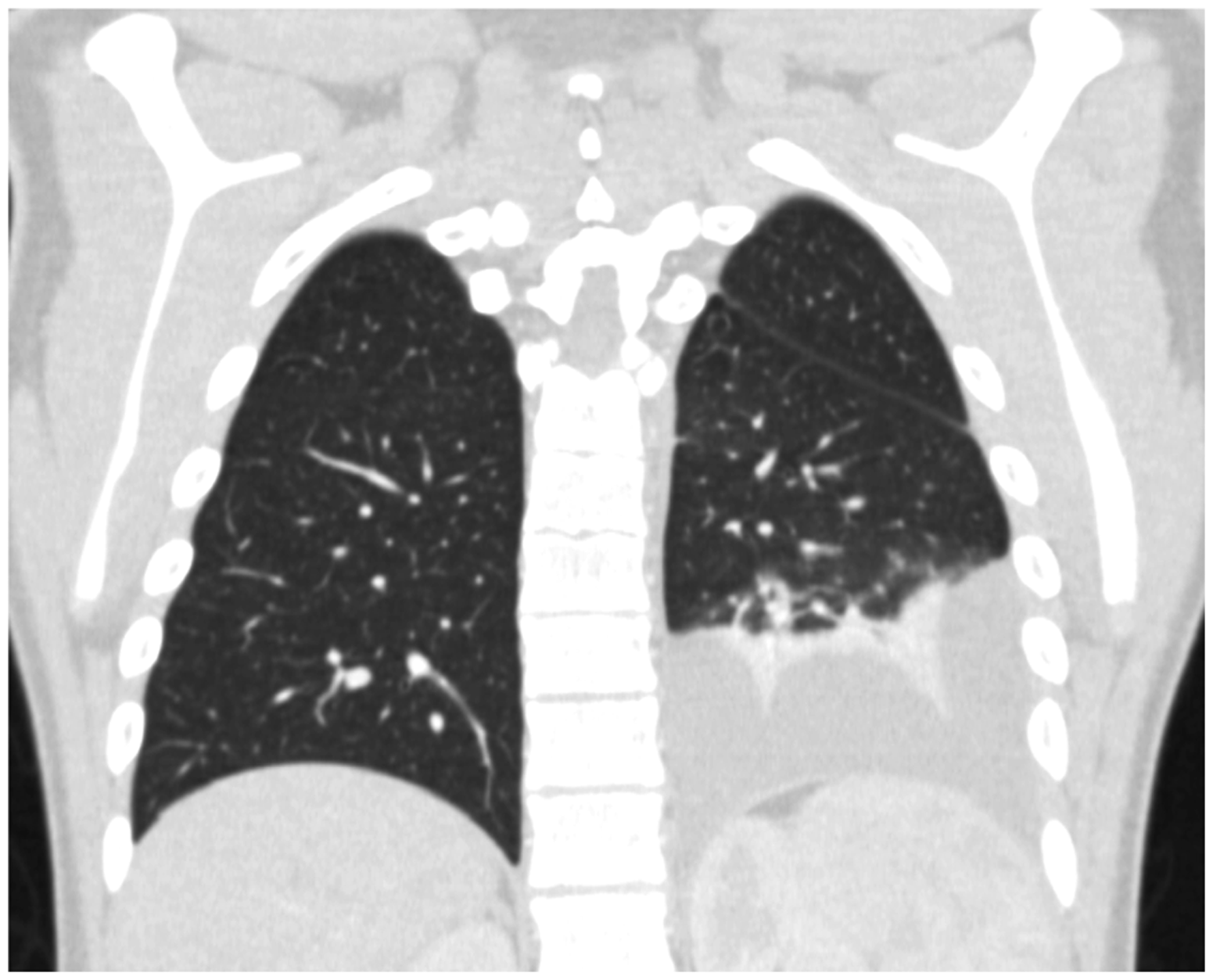
Draining 600 mL of sterile fluid via a chest drain soon improved the appearance of the effusion on chest X-ray and the patient’s symptoms slowly resolved. After spending almost 1 month in hospital, the patient had made a good recovery and was discharged on warfarin for 3 months and co-amoxiclav for 1 month.
Discussion
The case presented above has a number of interesting features. Firstly, a dental source of infection in Lemierre’s syndrome is rare. According to one systematic review of the literature, 2 which studied 84 case reports from 1950 to 2007, dental infection accounts for only 1% of cases. This compares to 37% of cases being related to infection in the peri-tonsillar tissues. An interesting feature in this case was the lack of demonstrable infection by Fusobacterium necrophorum, the most frequent cause of Lemierre’s syndrome, on microbiological specimens. Here, Streptococcus anginosus appeared to be the causative organism.
In Lemierre’s syndrome, it would seem logical that the ipsilateral internal jugular vein to the source of infection should become thrombosed. Indeed, this is supported by other case reports. 6 However, in the case we present, a more unusual pattern of spread is apparent: the infection originating in the lower right second molar, then proceeding via the submandibular space to the left prevertebral space and internal jugular vein. Another unusual finding was that of hypoglossal nerve paresis, presumably linked to the deep pus-filled cavity in the region of the left internal jugular vein and carotid artery. We were unable to find any other reports of this complication in the literature.
Mention should also be made of the lack of pulmonary thromboembolus on the CT pulmonary angiogram, the presence of which is often a feature of Lemierre’s syndrome. Malis et al. 7 also note the lack of this finding stating: the ‘…presence of jugular vein thrombosis along with pulmonary infiltrates with effusion…’ remains characteristic of the syndrome. They attribute the lack of the classical clinical picture of cavitating pulmonary lesions to the introduction of antibiotics.
Controversy exists regarding the evidence base for use of anticoagulation in cases of Lemierre’s syndrome, mainly due to its low incidence which precludes randomised controlled trials. 2 A potential advantage of anticoagulation is earlier resolution of the internal jugular thrombosis and its resulting bacteraemia. 8 However, it has been noted that haemorrhage from the sites of septic emboli may be related to its use. 9
Conclusion
As noted in the literature, 2 the incidence of Lemierre’s syndrome may be increasing in recent years. This could be related to reduced antibiotic prescribing 10 or perhaps antibiotic resistance of causative organisms. Renewed emphasis must therefore be placed on the need to be vigilant for the signs and symptoms of this potentially fatal condition.
In particular, a young fit patient (the average age being 16–19 years 11 ) with localised oropharyngeal infection followed by fever, tender swelling of the neck and dysphagia should raise suspicion. Tenderness and swelling, usually unilateral, at the angle of the mandible and running parallel and anterior to the sternocleidomastoid is strongly suggestive of internal jugular vein thrombosis. 8
Pleuritic chest pain, dyspnoea and haemoptysis may accompany these symptoms, 7 indicating pulmonary involvement due to septic emboli. It should be noted that while pulmonary septic metastases are the most common, the condition can exhibit spread to any site. 12 The second most frequent sites of metastatic spread are the joints, whilst infection of the liver, kidneys and peritoneum have also been commonly reported. 13
Diagnosis is primarily on clinical grounds, and may be supported with radiographic or microbiological evidence. 14 Differential diagnoses may include pharyngitis, infectious mononucleosis, pneumonia, endocarditis and intra-abdominal sepsis. 15 A contrast enhanced CT of the neck is the imaging modality of choice to confirm internal jugular vein thrombosis, 16 while a chest X-ray and/or CT may show pulmonary consolidation, pleural effusion or a septic thromboembolus. Treatment comprises aggressive use of antibiotics (typically a penicillin combined with clindamycin or metronidazole) and surgical drainage of abscesses. 13
Learning points
The incidence of Lemierre’s disease appears to be increasing. Early diagnosis leads to a better outcome. A high index of suspicion is needed in cases of oropharyngeal infection followed by fever, tender swelling of the neck and dysphagia – especially in young patients.
Author’s contributions
Deborah Boyd: Selection of case, proofreading
Paul Paterson: Report text, literature search
Louise Dunphy: Literature search
Andrew Carton: Consultant in charge of patient’s care and review of case
Nicholas Hammersley: Consultant in charge of patient’s care and review of case
Patient consent
A signed consent form is available.
Footnotes
Declaration of conflicting interests
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.