
Abstract
This paper will explore the development of medical education in the Soviet Union, its underlying principles and the subsequent migration of this format into the countries of the Soviet Bloc following World War II. The impact of Perestroika and the collapse of the Warsaw Pact on university training and medical education in particular will be reviewed. The need for external funding as a factor in the emergence of English Parallel courses in Hungary, Czechoslovakia and subsequently in other countries will also be considered.
The need for doctors within the Soviet Union was acknowledged shortly after the revolution and was followed by a determined effort to increase the number of medical schools and the number of graduates. The Soviet Union’s approach to medical education was adopted throughout the countries of the Soviet Bloc after World War II. As a result the seven Comecon states were able to double the number of physicians from 568,000 in 1960 to 1,030,000 in 1974.
State support accounted for 90% of university funding but this became scarce with the collapse of the Soviet system. This issue was one of the driving forces, which stimulated an entrepreneurial approach to the search for external revenue, in particular foreign currency-based funding. In 1992 Charles University in Prague started an English taught course, often known as the ‘English Parallel’. This was followed by the development of a number of similar programmes across Central and Eastern Europe. This growth of a trans-national approach, especially across the whole of Europe, has led to the recognition of a need to harmonise higher education within the continent. This was given some structure by The Bologna Declaration of 1999 and the Prague Communiqué of 2001. The need for rigorous academic standards and a new approach to the medical curriculum and its teaching are discussed.
This paper will explore the development of medical education in the Soviet Union, its underlying principles and the subsequent migration of this format into the countries of the Soviet Bloc following World War II. The impact of Perestroika and the collapse of the Warsaw Pact on university training and medical education in particular will be reviewed. The need for external funding as a factor in the emergence of English Parallel courses in Hungary, Czechoslovakia and subsequently in other countries will also be considered. Critical to the development of these programmes was the decision to use English as the medium of instruction and to balance this against the fact that for many teachers and patients this was not their usual method of communication. In contrast, in the United Kingdom, overseas graduates have been required to become fluent in English before they can begin undergraduate training in medicine. Similar approaches existed in most western European countries and in the USA until recently. The development of these medical training programmes using English as the medium of instruction will therefore be examined in the light of work on the nature of international education and classrooms and the role of the educator in such a setting. This paper will provide the setting for a better understanding of those graduates from such schools in Eastern and Central Europe who have chosen to work in the British Isles and the relevance of their education to western European clinical practice.
The literature reviewed in this introduction was identified from a range of sources which included:
A search using PubMed and the terms East Europe Medical Education and substituting Czech, Polish, Hungarian, Soviet and Russian for East Europe. This yielded 1, 93, 154, 41, 17 and 364 references, respectively. An internet search using Google with the same terms in the form ‘East European’ + ‘Medical Student Education’, which yielded 27 references. Substitution of Czech for ‘East European’ yielded 205, Polish 327, Hungarian 158, Soviet 131 and Russian 540. The terms ‘English Parallel’ + ‘Medical Education’ yielded 13 sites. An internet search of the British Library Catalogue. The term Czech Medicine yielded 54 entries, Polish Medicine 1, Hungarian Medicine 33, Soviet Medicine 15 and Russian Medicine 12. An internet-based search of an international used book catalogue provided by AbeBooks yielded 127 used books dealing with Russian Medicine, 188 with Soviet Medicine, 64 with Polish Medicine, 1 with Czech Medicine and 1 with Hungarian Medicine.
These entries were reviewed and the references in appropriate articles also examined to form the basis for the following literature review.
Following the Revolution in Russia universities were opened up to people regardless of gender or race.
1
As a result entrance requirements were low and initial graduates of poor quality. However, by 1922 this situation had been remedied and a new curriculum was introduced. This curriculum puts emphasis on preventive medicine. Further modifications during the First Five Year Plan led to the division of training for medical students into ‘practitioners for therapeutic and general prophylactic work, public health physicians and specialists for the protection of mother and child’.
1
These divisions reflected a concern with health protection and disease prevention which was encapsulated in the slogan: The protection of the health of the workers is the task of the workers themselves.
2
This approach to health care and medical training persisted through the decades and was often reflected in the medical education programmes of countries included in the Soviet Bloc after World War II. The changes introduced during the 1920s were accompanied by a movement towards integrated teaching of medicine, including social and economic factors. 2 This approach placed an emphasis on preventive education for the general population and such a role is now recognised in Western medical education. 3 Indeed, even as early as 1922, the General Medical Council in the UK resolved that the medical curriculum should include preventive aspects of medicine. 4 This was not the case generally in countries such as Germany, Austria, Netherlands, Sweden, Denmark and Switzerland. 4
Medical schools and student in the Soviet Union before World War II. 1
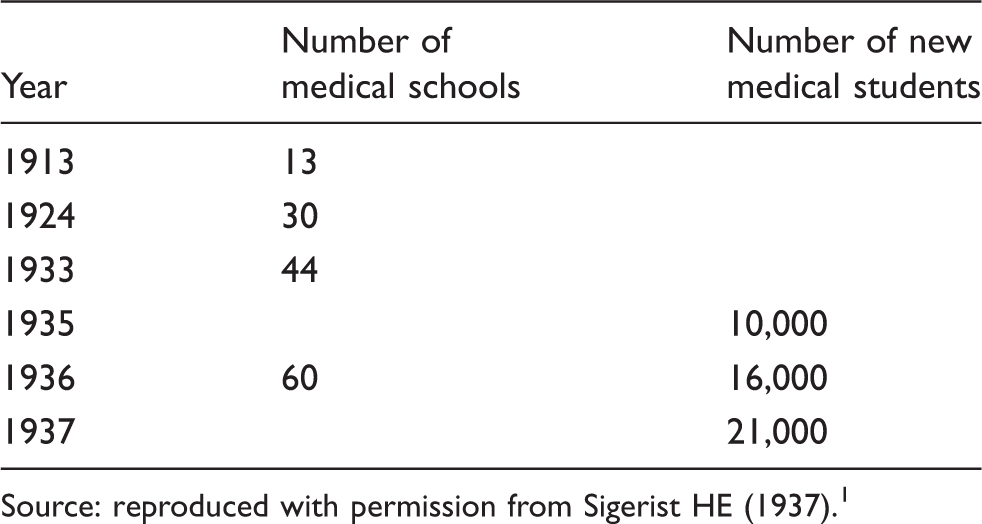
Source: reproduced with permission from Sigerist HE (1937). 1
No data were provided on the number of medical students in 1913, 1924 and 1933 or the number of medical schools in 1935 and 1937.
This drive to increase the number of medical graduates was also linked to a determination to increase the proletarian background of those trained in medicine. In 1930 in a directive of the Commissariat of Education the quota for medical schools was 60%. 5 By 1967, 28,000 new doctors qualified each year, with a total of just under 600,000 doctors in the country. 6 In 1974, there were 31.5 doctors per 10,000 population. 7 From 1994 the admission rate was fixed at 21,200 per year with some students being targeted to specific regions or programmes. Competition was high with 5 candidates for each place. 8 During this period the course length was extended from 6 to 7 years with more attention being given to the training of specialists. The last two years were spent in supervised clinical practice as a subordinat on a student stipend and then as an internat on a salary. 9 However, it was at this time that Chazov, a cardiologist who was minister of health, drew attention to the inadequate funding of both medical care and medical education. He contended that more attention was given to the number of students graduating than to their level of competence. 10 This was reflected in a lack of clinical experience amongst new graduates in basic clinical and investigative skills.
Number of physicians per 100,000 population in Poland, Hungary and Czechoslovakia. 12
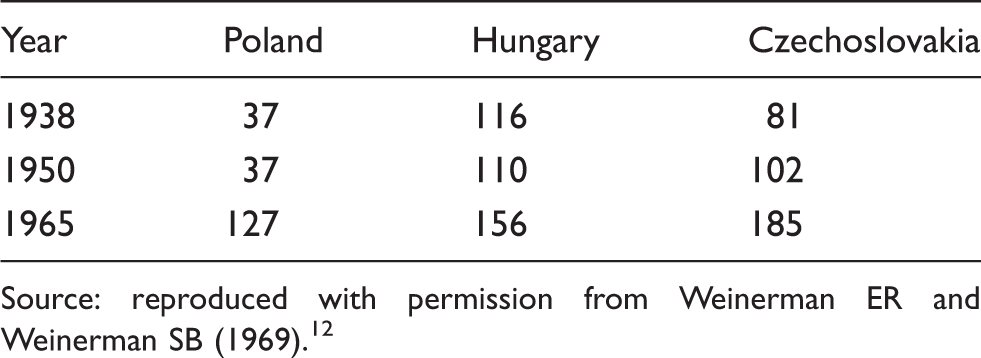
Source: reproduced with permission from Weinerman ER and Weinerman SB (1969). 12
Courses in Czechoslovakia, Hungary and Poland followed a 6-year programme. The first half was concerned with preclinical sciences and the second with clinical disciplines. 12 The average number of students in each class was about 250. 12 This approach was adopted because of the shortages in medical manpower caused by World War II and the introduction of the Soviet model for an increased proportion of doctors in the population. As a result the seven Comecon states were able to double the number of physicians from 568,000 in 1960 to 1,030,000 in 1974. 13 In countries, such as Poland, the increase was dramatic at 84% and depended mainly on training significantly more women. 13
By the late 1980s independent activism was spreading throughout Eastern Europe. The transformation was most marked in Poland, but significant changes were also taking place in Czechoslovakia, Hungary, Romania and East Germany. 14 In Prague high school and college students led the way with demonstrations under banners such as ‘Parents come with us, we are your children’. 14 By December 1989 democracy was in sight and free elections were promised for June 1990. 14 The Velvet Revolution led to fundamental changes in the health service with people having a right to choose their own doctor. 15 In addition it led to significant changes in the management and financing of Czech universities. State support accounted for 90% of university funding and this became scarce with staff pay increasingly poor. 16 This issue was one of the driving forces which stimulated an entrepreneurial approach 17 to the search for external revenue, in particular foreign currency based funding. The fact that there were many young people who had failed to achieve a place in a medical school, particularly in the USA, and that many had sought training in off-shore medical schools formed the basis on which universities such as Debrecen in Hungary and Prague in the Czech Republic decided to develop courses which would appeal to this market. The critical element was that the language of instruction would be English rather than Hungarian or Czech.
In 1992 Charles University in Prague started such an English taught course, often known as the ‘English Parallel’.
18
It follows the traditional pattern of a 6-year course, with 3 years of preclinical sciences prior to entering clinical rotations.
19
The style of teaching is didactic, but self-directed learning is also encouraged. Initially 5 or 6 students enrolled each year. By 2004 the figure had risen to 60 and now runs at more than 100.
20
Admission is through an entrance examination with a success rate of about 50%. The motivations behind prospective students appears to vary from country to country, but includes the university’s prestige, the nature of the course,
19
cost of living as well as failure to achieve a place in one’s own country. About 30% of students fall into this latter category.
20
The response by bodies such as the General Medical Council was not encouraging. In 1993 a brief news review of the course was published in the British Medical Journal.
21
At the time of the review four students had completed their first year and one reported concerns about his ability to master the Czech language with sufficient fluency to allow meaningful patient contact. Within 2 weeks the GMC responded with a letter which included the following comments: The acceptance of these qualifications is currently under review, partly because of anxieties about the difficulties of giving satisfactory clinical training to English speaking students, characterised by the example in the article. The General Medical Council has asked for further information about several matters; when it has received this information it will decide whether the degrees should continue to be accepted.
22
The attitude embodied within this letter failed to recognise two salient points. Firstly Britain had been selling medical education to overseas students for many years. Students for whom English was a second language were not given special tuition to ensure that they were understood or could be understood by people with a wide range of regional English accents. Secondly the Czech Republic was a candidate country for EU admission and once a member the GMC would be required to accept its graduates as it was of other EU member states. A more sensible approach might have been to support the development of the programme and to have had an effective input into the training offered.
Subsequent to the opening of the English Parallel course in medicine at Charles University further programmes have been developed at other institutions,23,24 which are now within the European Union. They include:
Czech Republic: Palacky University Olomouc
25
Masaryk University Brno
26
Slovakia Pavol Jozef Safarik University, Kosice
27
Comenius University, Bratislava
28
Poland Uniwersytet Medyczny, Lodz
29
Bialystok Akademia Medyczna
30
Akademia Medyczna im. Karola Marcinkowskiego W.Poznan
31
Jagiellonian University Krakow
32
Academia Medyczna w Gdansku
33
Medical University of Silesia, Katowice
34
Hungary University of Pecs Medical School
35
University of Szeged
36
Debreceni Orvostudomanyi Egyetem
37
Estonia Tartusskogo Universiteta
38
There are other English Parallel courses, which exist outside the European Union. The feature which distinguishes courses at the above institutions from these other programmes is that graduation entitles the successful student to register in any European Union country without further assessment, at present. English Parallel courses have an attraction for universities in need of external sources of revenue and their number is expanding, with recent openings at the University of Tartu, Estonia in 2006. In addition, with the expansion of the European Union in 2007 the following medical schools have also been brought within the fold:
Romania Facultatea De Medicina Universitatea Din Oradea (Established 1991)
39
Victor Papilian Faculty of Medicine, Sibiu
40
Bulgaria Pleven Medical University
41
In the longer term potential other entrants to the EU include: Croatia University of Zagreb Medical School
42
Turkey Cerrahpaşa Medical Faculty of İstanbul University
43
Ukraine Crimea State Medical University
44
Lugansk State Medical University
45
This growth of a trans-national approach, especially across Europe, has led to the recognition of a need to harmonise higher education within the continent. This was given some structure by The Bologna Declaration of 1999 and the Prague Communiqué of 2001. Amongst their main objectives was the need to increase mobility and improve conditions for it.
46
Amongst the signatory countries were the Czech Republic, Estonia, Hungary, Poland, the Slovak Republic and the UK.
47
The principles espoused by this declaration include:
Adoption of a system of easily readable and comparable degrees Adoption of a system based on two main cycles, undergraduate and graduate Establishment of a system of credits which will allow student mobility Promotion of mobility by overcoming obstacles to the exercise of free movement Promotion of European co-operation in quality assurance Promotion of the European dimensions including curricular development, mobility schemes and integrated programmes of study
47
These changes towards a trans-national European style of higher education have necessitated the recognition by staff that ‘non-nationals’ are part of the daily scene.
48
The curriculum in such institutions will need the input of both foreign and domestic students to give added international and intercultural value. According to Teekens the lecturer becomes a core player in the internationalisation of the institution.
48
Such lecturers need to be committed to the principle and to be at home in an environment where the language of instruction is not their own or indeed that of many of the students. Teekens has proposed that for such institutions to be successful both teachers and students need to have certain attitudes in common. These include:
Paying attention to good academic standards Having a good command of the language of instruction while paying sufficient attention to individual differences Increasing their cultural awareness Acknowledging that various teaching and learning styles have conditioned people in different traditions of education Making use of multimedia in an integrated way in the communication process of teaching and learning Recognising that job qualifications and periods of probation are differently organised and valued in different countries
48
Teekens has further emphasised the need for lecturers in the international classroom to reflect on their own backgrounds and perceptions and the ways in which their own culture has helped formulated these while becoming familiar with basic educational theory. This will allow them to cope better with a range of teaching and learning styles, which will be different for many of their students. 49 This will be particularly the case with medical students where they will also need to understand the culture and attitude of the patients from the host country.
The EU had at an earlier date defined the criteria which were necessary for a medical graduate to be recognised as having the necessary qualifications and experience to practice clinically. The directive states that before students can receive a primary medical qualification (PMQ) they must have:
Adequate knowledge of the sciences on which medicine is based and a good understanding of the scientific methods including the principles of measuring biological functions, the evaluation of scientifically established facts and the analysis of data. Sufficient understanding of the structure, functions and behaviour of healthy and sick persons, as well as relations between the state of health and physical and social surroundings of the human being. Adequate knowledge of clinical disciplines and practices, providing the student with a coherent picture of mental and physical diseases, of medicine from the points of view of prophylaxis, diagnosis and therapy and human reproduction. Suitable clinical experience in hospitals under appropriate supervision.
50
The reported experience of students in Czech universities is yet to meet the standards advocated by Teekens for international classrooms. In contrast Healey describes the relationship between professor and student as ‘stiff and stern’ with academics failing to accept responsibility for the welfare of their students.
16
Some equate high standards with high failure rates and fail to recognise the possibility of their poor presentation of the courses. Such attitudes may contribute to the high prevalence rate for a study of self-reported cheating from Croatia.
51
Thirty-nine per cent of these medical students reported:
Altering class attendance lists Using a crib sheet during an exam Arranging with administrative personnel to be assigned to a lenient examiner Copying answers during an exam
51
Thirteen per cent admitted to:
Submitting other student’s work as their own Using a mobile phone to exchange answers during an exam Finding out about test questions in advance
51
Indeed a study of non-medical students in Russia, Israel, Netherlands and the USA has shown that Russian students were more tolerant of cheating and had very negative attitudes towards reporting this behaviour to school officials.
52
Prior to accession to the EU a study of corruption and anti-corruption policy in Slovakia reported that: Corruption also appears to be widespread in the education system, especially at the level of higher education
53
Twenty-three per cent of students in higher education reported paying a gratuity or bribe in the previous year, usually with an average cash payment of Є163. This was often linked to admission to a university and 86% of respondents believed it was essential to gain acceptance into a medical school.
53
Similarly in Poland in 2001 high school students in Lodź, Bialystok and Lublin were caught buying entrance examination papers for medical school.
53
Concerns about the role of such activities within medical schools in Central and Eastern Europe are widespread. In a study of plagiarism amongst 295 second-year medical students conducted over a 3-year period at the University of Rijeka, Croatia Bilić-Zulle found the attitudes of medical students towards academic integrity disturbing. She reported that: A quarter of the students found the case of cheating appropriate and half of them thought it was justified and deserved no penalty. Approximately half of the students (39–66%) would act as described in the scenarios, if they deemed it to be necessary. In addition, 33–45% reported to have witnessed similar cases in their environment.
54
Of course, such behaviour is not limited to universities in Eastern Europe. In a comparative study of 443 business students in the USA and 192 in Poland both groups admitted to significant levels of cheating. In the case of the Polish students it was 84% and 55% amongst the Americans. 55 In a study of the moral attitudes of 310 Czech and Slovak and 70 foreign national students at Charles University in Hradec Králové, examined moral judgement competence and moral attitudes using Lind’s Moral Judgment Test. 56 She found that moral judgement competence decreased significantly in the Czech and Slovak medical students as they grew older and completed more semesters; in medical students from other countries it did not significantly increase. Although the use of questionnaires to investigate such attitudes has limitations the findings are consistent with those described in studies of cheating and plagiarism amongst universities in Eastern Europe. In support of these views, Horak, who headed the first internal medicine department at Kralovske Vinohrady Hospital in Prague, has questioned whether the teaching standards at most Czech medical schools are comparable with those in other EU countries. In particular, Stahalova, an oncologist from Bulovka, has suggested that the training of communication skills, both with patients and other health care professionals, needs sharpening. 57 These issues have been recognised in the Second Medical Faculty at Charles University where 106 students were exposed to early patient contact in the community, following sessions with a general practitioner as trainer and subsequent seminars about communication skills. However, the study lacked objective measures as to its value and was assessed in such terms as ‘continuing interest’ and ‘positive response’. 58 A not too dissimilar approach has been adopted in Gdansk, although the assessment by students and staff was more formalised. 59 Interestingly in neither case was any attempt made to involve patients in these assessments of student performance.
Such reports from individual medical schools emphasises the need for the development of common standards in medical education across the European Union. The National Unions of Students in Europe (ESIB) has espoused this cause in a more general way for the whole of higher education. It has recognised the value of transnational education which allows student mobility, but demands an international curriculum. 60 It also recognises the need for true mobility and not its simple substitution by e learning. Clearly there has been a long tradition of international medical education with students travelling to distant centres to experience different teaching and to learn of new developments.61–63 However, the provision of courses by medical schools in English is a recognition of an international demand for training by students and this is matched by a requirement by countries throughout the world for properly trained clinicians who can deliver a high quality service. The opening up of courses directed at both these requirements means that they cannot simply be a foreign language version of the indigenous programme. Rather they will need to subscribe to a wider philosophical basis, which will take into account both the nature of the students attending such courses, the type of teaching provided and the methods of assessment used. The need for an internationally mobile work force and the concept of ever greater European integration makes these requirements mandatory. There is no longer a place for isolationism within medical education, if there ever was.
Footnotes
Declaration of conflicting interests
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.