
Abstract
Background
CT coronary angiography (CTCA) is an emerging diagnostic tool in the assessment of patients with suspected coronary artery disease. It has several advantages over conventional coronary angiography (CCA); however, its use is not yet widespread in large teaching centres.
Aims
To determine what proportion of patients who have CTCA, do not require subsequent CCA.
Methods
A prospective analysis of all patients referred for CTCA from the start of the service in January 2008 to April 2010.
Results
CTCA provided definitive diagnostic images in 85% of patients. Overall only 12% (n = 33) of patients had subsequent CCA. The proportion of patients who subsequently had CCA reduced with time reflecting increasing confidence with the clinical service.
Conclusions
A CTCA service can be successfully established out with a large teaching centre hospital. Close working between cardiologists and radiologists leads to increased confidence in the service and obviates the need for CCA in a large proportion of patients.
Introduction
Coronary heart disease (CHD) is a significant health care problem with almost 100,000 deaths per year from CHD in the UK alone. A further 200,000 people have had a myocardial infarction (MI), and it is estimated that approximately 2 million people suffer from angina, with its incidence growing as more people survive acute coronary events. 1 Thus, demands on cardiology services are high and due to an ageing population are increasing despite population benefits from primary prevention.
In our region we responded by utilising locally available technology and initiated a CT coronary angiography (CTCA) service. While coronary catheter angiography (CCA) has been the anatomical ‘gold standard’ investigation for obstructive coronary heart disease (CAD), substantial evidence now supports the role of CTCA in certain patient groups.2–9 CTCA has a sensitivity of 85–95%, specificity of 95–95% and a negative predictive value of 96–100% for assessing coronary artery disease.3,10 It is particularly useful for patients with low or intermediate risk of having coronary artery disease, thereby avoiding the risks associated with catheter angiography. Furthermore, recent guidelines support a greater use of CTCA for the assessment of patients with new onset chest pain. 11
However, there are some pitfalls with CTCA and several elements should be considered when establishing a new service (Table 1). Optimal imaging on the now standard 64-slice CT scanner requires a stable, sinus bradycardia and a breath-hold of 8–15 seconds preferably in a non-obese subject. There is a radiation burden to the patient of 1–5 mSv for prospective ECG gated scans and 7–15 mSv for retrospective ECG gated scans. The latter dose is similar to CCA and nuclear scintigraphy. The radiation dose can be reduced by up to 90% with judicious scanning technique and the use of the most recent software. 9 CTCA can cost as little as 20% of the total cost of a catheter study.
This study aimed to prospectively determine what proportion of patients who undergo CTCA, do not require subsequent CCA and thus assess the clinical utility of CTCA in a regional hospital, which also provides cardiac catheter angiography and coronary angioplasty.
Methods
Design
A prospective analysis of all patients referred for CTCA from the start of the service in January 2008 to April 2010 was carried out. All patients referred by cardiologists for assessment of coronary arteries were included.
CTCA protocol
Patients were rehearsed immediately prior to the CT about breath-holding technique and had received a detailed information sheet at home. Metoprolol (50––200 mg) was administered orally 1 hour prior to imaging and additional intravenous Metoprolol was titrated in 10 mg aliquots to obtain an optimal heart rate of ≤62 bpm. All scans were performed on a 64-slice scanner (GE Lightspeed VCT XT). Initial patients were scanned with retrospective gating and from June 2008 were scanned preferably by prospective ECG gating. Iodinated intravenous contrast media of 350 mg/mL strength and 60–90 mL volume was administered via an antecubital vein at a rate of 5 mL/s. Scanning was performed at 100–140 kVp, effective tube current at 550–800 mA, slice collimation 64 × 0.625 mm and 0.35/ s rotation time. Image reconstruction was typically performed at 75% of the RR interval with further phases if available. Scans were jointly reported by a consultant cardiologist (SJL) and a consultant radiologist (JHM).
Coronary angiography
The decision to proceed to CCA was at the discretion of the cardiologist. Some patients had already had a CCA. In these cases CTCA was used to clarify native coronary or bypass graft anatomy that had been difficult to define during CCA.
Data handling and statistical analysis
Data were prospectively collected on all patients. Details included age, gender, indication for scan and subsequent coronary angiography result. CT scans were considered abnormal if there was any evidence of coronary artery disease and were further divided into 3 groups based on assessment of luminal stenosis <50%, 50–75% and >75%. Low-grade disease including calcification score and mild soft plaque was commented upon. Data were divided into quintiles for date of scan (to assess learning curve) and patient age (to assess impact of advancing age on scan quality).
Results
During the study period, CTCA was performed on 269 patients for assessment of coronary arteries or bypass grafts of whom 157 (58%) were female. About 256 were performed for native coronary vessel disease, 12 for bypass graft disease and 1 specifically to assess for coronary stent patency.
Elements to be considered when setting up a service.
Causes for non-diagnostic CTCA (n = 41).

Temporal effect on new service
There was consistency over time in terms of the age of patients referred for CTCA, and the proportion of scans that were found to be normal. However, there was an incremental increase in the proportion of patients who did not have CCA following a CTCA (Figure 1).
CTCA result and subsequent CCA by time.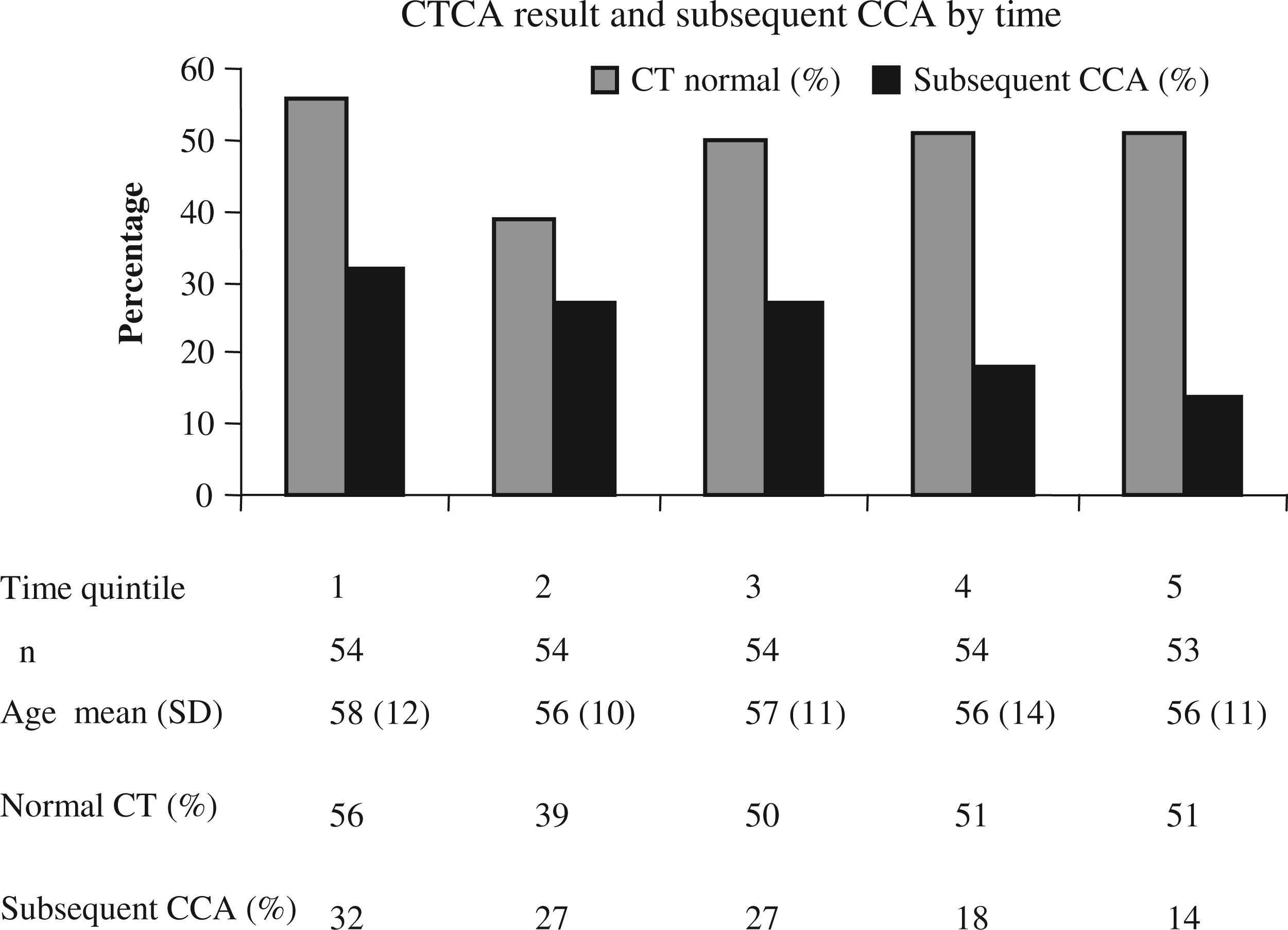
Effect of patient age on CTCA results
With increasing patient age there was an expected increase in the proportion of patients with an abnormal CTCA and a corresponding increase in the proportion of patients who did require a CCA (Figure 2).
CTCA result and subsequent CCA by age.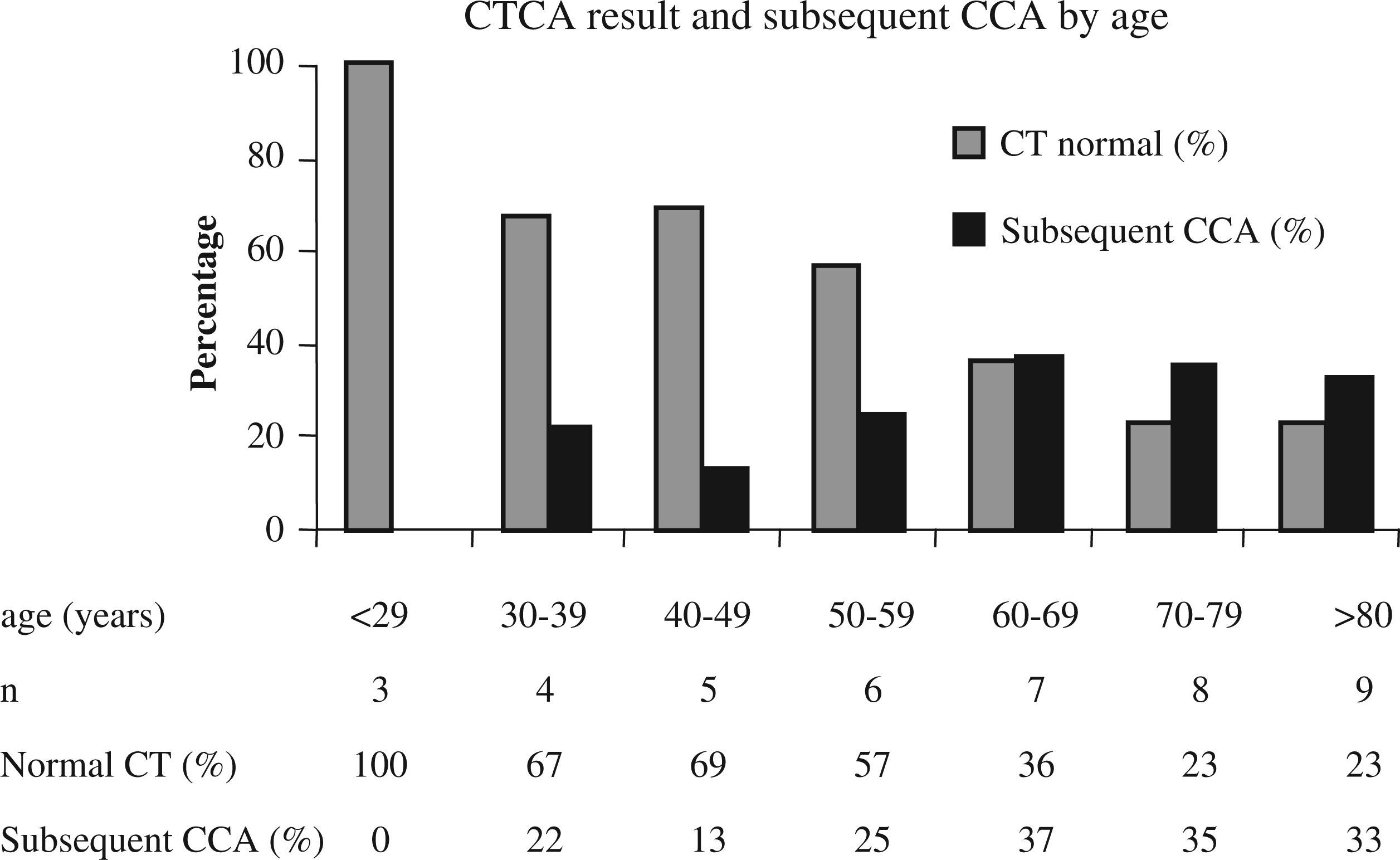
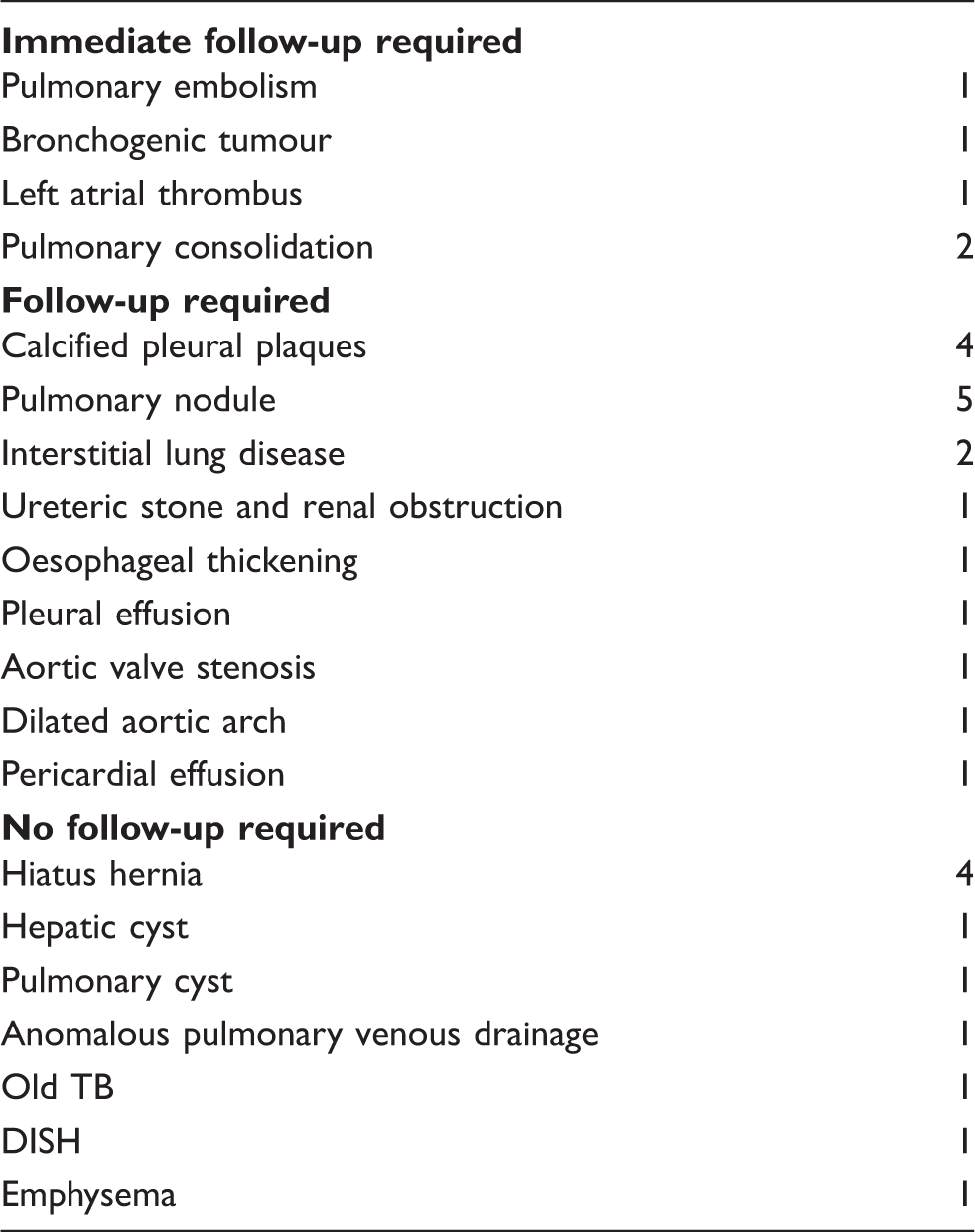
Incidental findings
Incidental findings.
Discussion
This study describes the early experience of CTCA in a remote Scottish regional centre. The main finding was that over a short period of time there was increased referrer confidence in the CTCA results leading to a marked reduction in the proportion of patients who subsequently proceeded to CCA. This study also found that with increasing age the proportion of patients with a normal scan was reduced and a higher proportion of older patients went on to CCA. Therefore it is likely that in older patients that CTCA is less useful at giving a definitive diagnosis and avoiding CCA.
Confidence in CTCA
Worldwide, there is increasing use of CTCA. However, despite this, there remains a certain lack of confidence in this technology among cardiologists and cardiac surgeons who may be unfamiliar with this technique. For example, many hospitals still do not offer this service and even where this technology is available the majority of cardiac surgeons would be unlikely to operate on patients even for an isolated heart valve without confirmation of findings by CCA. In our study we found a similar phenomenon within referring cardiologists, but over time there was a reduction in the proportion of patients who underwent CCA following CTCA as local cardiologists gained confidence in the technology, image acquisition and reporting. Dual reporting and close clinical working are vital to establishing this clinical confidence.
Clinical utility of CTCA
CTCA has an excellent negative predictive value for coronary artery disease, i.e. it is an excellent test for excluding coronary artery disease in patients, under investigation for chest pain, with normal coronary arteries. The proportion of patients with abnormal CTCA in our cohort was much higher than most patient cohorts in the USA reflecting our continued conservative approach to the investigation of patients with chest pain in the UK. Increasing evidence supports the use of CCTA for the evaluation of patients with stable intermediate risk coronary disease3,10,12 as there are significant potential benefits of avoiding the associated risks and complications of CCA. In addition, there are potential cost savings by performing CCTA over CCA in patients with intermediate risk. 5 The cost savings associated with CTCA in low-risk patients has not been evaluated as yet.
Patient selection
Patient selection is important, especially in the early stages of a new CTCA service to ensure high quality scans. Patients require to breath-hold and image quality is greatly reduced if patients are not in a stable sinus bradycardia. CTCA is probably of most use in the investigation of normal or near normal coronary arteries (reflected by its high negative predictive value). However, it is also has great utility in assessing coronary artery bypass graft patency. 13 In patients with previous coronary stenting, CTCA can demonstrate coronary artery stent patency; however, stents and coronary calcification can obscure luminal detail and it would be wise to avoid scanning such patients in the early stages of a local service development.
Non cardiac findings
The finding of urgent, non-cardiac incidental findings which required immediate intervention or onwards referral demonstrates the importance of ensuring that the reporting individual reviews all images in all window settings and all fields of view and has the skill to do so. This has been highlighted as a potential issue when a non-radiologist reports alone. 14 In this study other less urgent, incidental findings such as five pulmonary nodules required further investigation and were found to be benign or resolved. One bronchial carcinoma was identified and represents 0.05% of our study group, below the level found by Kim et al. 15 who reported a detection rate of 0.31%. In our centre, the full transthoracic field of view images are reviewed also to avoid missing detectable lesions not seen on ‘heart only’ image. Joint reporting is to be encouraged to foster education, communication and sharing of facilities and staff. 2
Calcium scores
The utility of calcium scoring is much debated.7,11,16 Initially all patients in this series had a CT calcium score which helped plan the CTCA. As further large radiation dose reductions became possible with prospective ECG gated scans then the dose from the calcium score became a significant duplication. We disagree with recent guidelines 11 about the use of CTCA with differing calcium scores. The risk of cardiac events with zero calcium score is not negligible as unstable, obstructive soft plaque is seen in symptomatic younger patients in our limited experience (n = 5). Also it is possible to produce a diagnostic CTCA with a calcium score of over 400 Agaston units but admittedly a little more difficult when post processing the data on a workstation. CT calcium scores, however, have a valuable prognostic contribution worthy of further comparative investigation with other tests such as dual energy CTCA and perfusion scintigraphy. 8
Cost and accessibility
CTCA costs 250 UK pounds versus a CCA of 1400 UK pounds as per local NHS accounting. However, there is no doubt that the threshold for CTCA will appropriately be lower than CCA and thus the overall service costs with the introduction of a service are less clear. However, in areas which have a CT scanner but no local CCA service, CTCA has the potential to improve access to anatomical investigation of patients with suspected coronary artery disease and address the geographical gradients seen in patients who are remote from a cath lab. 17
Training issues
Current accreditation in the UK and USA for an individual to perform and interpret CTCA is rigorous and rightly onerous to ensure competence and patient safety.2,18 It is also supported by the National Imaging Board on Cardiac Imaging (DoH Eng), which recommends at least two level 2 accredited consultants per site. 2 For new centres who are establishing this service, training courses are available in the UK and USA.
Limitations of the study
Patients were limited to non-asthmatic patients who are able to comply with breathholding and in whom the heart rate could be pharmacologically controlled and thus this was selected patient cohort. These criteria were adhered to, to ensure optimal imaging in the setup phase of this service. With increased experience and faster scanners these selection criteria may change. Another limitation is that we did not collect comprehensive data on our study group with regard to clinical risk scores and myocardial stress testing either by perfusion scintigraphy or exercise test. Nevertheless, this represents a real world cohort of patients referred for CTCA by a cardiologist for the assessment of coronary anatomy. This study was performed in a single site, non-teaching centre and may well be applicable to other similar hospital settings.
The future
Profound technological advances in CT are already here with the use of new detector substrates, dose reducing iterative reconstruction algorithms and faster scanners with longer z-axis coverage. Temporal and spatial resolution issues are being resolved so that assessment of plaque morphology will become routine. The clinical pathways of CAD management are in a state of flux as these innovations find their place in a financially constrained health care sector. The intuitive simplicity and beauty of the CT angiograms produced may soon gain acceptance even for surgical re-vascularisation decision making.
Conclusion
Our single centre experience demonstrates that a successful CTCA service can be confidently established in a regional location with standard equipment augmenting and replacing traditional, more expensive and invasive CCA in a significant proportion of patients.
Footnotes
Declaration of conflicting interests
JHM has spoken at conferences at request of GE plc and received honoraria.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Note
As this was a review of a clinical service, no formal ethical approval was required.