
Abstract
Objective:
To present an extremely rare case of sebaceous carcinoma arising in a mature cystic teratoma of the ovary.
Clinical presentation and intervention:
A 66-year-old woman presented with abdominal discomfort and a pelvic mass. Abdominal and pelvic ultrasound, as well as CT scan, revealed a 27 cm complex right pelvic mass, which was diagnosed histologically as a sebaceous carcinoma arising in a mature cystic teratoma. The patient underwent a total abdominal hysterectomy with bilateral salpingo-oophorectomy, peritoneal washings, appendicectomy and infracolic omentectomy.
Conclusion:
This case adds to the rare reports in the literature of sebaceous carcinoma occurring in a mature cystic teratoma. The clinical behaviour and optimal management of this entity are not well established. The patient has been well for 32 months following surgery with no evidence of recurrent disease clinically.
Introduction
Benign cystic teratoma is recognised as one of the most common tumours in women, which can occur over a wide age range. Malignant transformation of a benign cystic teratoma is a rare event occurring in less than 2% of the cases. 1 The most common malignant transformation seen is squamous cell carcinoma.2–4 This accounts for approximately 75% of malignant transformations.5–7 Pure sebaceous carcinoma is extremely rare with only seven previously reported cases.1,8–13 Along with a brief review of this neoplasm, we report the clinico-pathological and immunohistochemical features of a new and eighth case of a moderately differentiated sebaceous carcinoma arising in dermoid cyst of the ovary.
Sebaceous carcinoma has traditionally been divided into two groups: an aggressive periocular variant comprising about 75% of cases and a relatively non-aggressive extraocular form. The periocular variant presents more in the mid-sixties. It arises in association with the ocular sebaceous glands. 14 It accounts for approximately 1–5% of malignancies of the eyelid.14,15 They have a slight female preponderance and tend to involve the upper eyelid more than the lower.16,17 They often masquerade clinically as a chalazion, delaying effective treatment. Rarely, there is a history of radiation to the area. 17 The metastasis rate with subsequent mortality is high, approaching 25%. 17 Aggressive local behaviour with intracranial extension may also occur. 18 The metastatic and mortality rate can be significantly lowered (to 18%) with early detection and treatment. 19 The organs most often affected include the regional nodes with subsequent involvement of lung, liver, brain and bone. 15 Metastatic disease is a poor prognostic sign with a 50% 5-year mortality in one study. 17 Prognosis is particularly poor when both the upper and lower eyelids are involved. 17
Extraocular sebaceous carcinoma accounts for approximately a quarter of all cases. It commonly presents on the head and neck where sebaceous glands are more concentrated. Approximately a quarter of the extra-ocular tumours arise at other regions including the trunk and thigh and rarely genitalia.20–24 Other exceptionally affected sites include the nasal vestibule, breast, finger, foot and external auditory canal.25–29 The majority of cases are in their seventh decade.30,31 Sebaceous carcinoma can also very rarely arise at non-cutaneous sites. Documented cases have been described in the oral and buccal mucosa, hypopharynx, pulmonary bronchus, parotid and submandibular glands, uterine cervix and in dermoid cysts or benign cystic teratomas of the ovary.1,8–13,32–39 The parotid gland is the most common of the non-cutaneous sites. 37 Recently, extra-ocular cases with nodal and even visceral metastases have been reported, leading to question the previously believed concept that extra-ocular tumours are less aggressive than sebaceous carcinomas of the eyelid.21,40
Clinical presentation
A 66-year-old parous lady was referred to the gynaecology department with abdominal discomfort and a pelvic mass. Ultrasound demonstrated a complex right pelvic mass but no ascites. Subsequent CT scan of the chest, abdomen and pelvis, revealed a large right complex pelvic mass (27 × 12 × 10 cm), which contained small areas of calcification. A smaller left complex pelvic mass (6 cm) was noted with a small amount of ascites. There was no suggestion of metastatic disease. These radiological findings were felt to represent bilateral ovarian dermoid cysts; however, there was suspicion regarding malignant transformation within the right ovarian cyst. The CA125 was 111 kU/L.
A total abdominal hysterectomy, bilateral salpingo-oopherectomy, appendicectomy, infracolic omentectomy and peritoneal washings were performed. At time of laparotomy, bilateral ovarian cysts were noted, both were partially torted. The right ovarian cyst was adherent to omentum and lying in the upper abdomen. The left cyst had partially torted and was lying within the pouch of Douglas. There were no intraoperative complications. The patient was discharged from the department on the third postoperative day. The patient made an uneventful recovery and clinically has no recurrent disease at 32 months.
Pathological findings
There was an intact large multicystically dilated right ovarian tumour that measured 30 cm in maximal dimension. The cysts contained abundant dark brown fluid admixed with cheese like material and hair. There were also multiple small white friable solid areas with haemorrhage up to 5 cm in diameter. The cyst lining and solid areas were extensively sampled for microscopic evaluation. The left ovary was also cystic measuring 6 cm in maximal dimension. It contained greasy materials and cartilaginous parts.
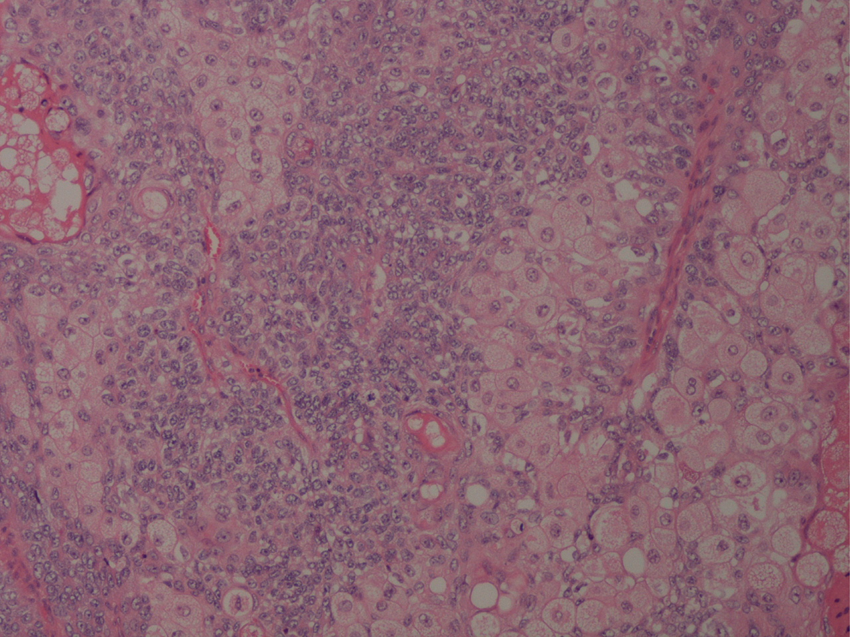
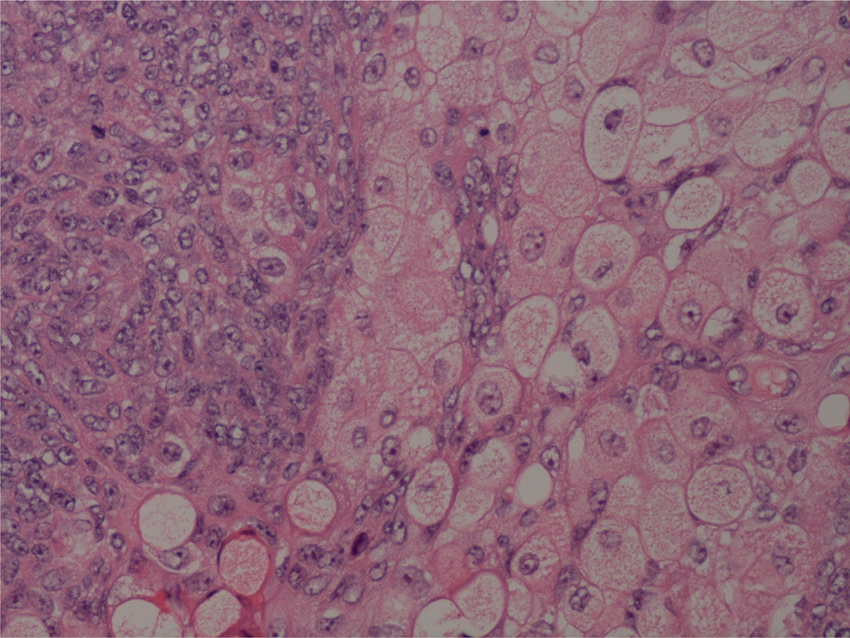
Microscopic examination of the right ovary showed a mature cystic teratoma with thyroid and cartilage tissue formation. In areas the cyst walls were denuded, lined by macrophages and contain cholesterol crystals. There was a 2.5 cm infiltrating tumour with a predominantly lobulated and nested growth pattern (Figure 1). The majority of the cells had vacuolated sebaceous cell morphology surrounded by basaloid cells. There was occasional so-called holocrine necrobiosis9 characterised by the presence of large areas of eosinophilic material admixed with ghost outlines of mature sebaceous cells (Figure 2). A moderate amount of hyperchromasia and nuclear pleomorphism were present. Mitotic figures were readily identifiable (Figure 3). The stroma was desmoplastic. The tumour was restricted to the ovary and did not infiltrate the capsule, vessels, adjacent structures or the omentum. The left ovary showed a benign mature cystic teratoma with skin, cartilage and focal bone formation. Peritoneal washing was negative for tumour cells. The uterus, cervix and both fallopian tubes were within normal limits histologically. The appendix showed a hyperplastic polyp but otherwise unremarkable.
Representative section of the tumour showing infiltrative lobules and nests of sebaceous carcinoma. A section showing atypical and infiltrating sebaceous cells surrounded by basaloid cells and blending with eosinophilic secretions. A high-power view from the tumour showing moderate nuclear pleomorphism, hyperchromasia and readily identifiable mitotic figures.
Immunohistochemistry: In our case, the tumour cells stained diffusely for Cytokeratin 5, p63, Androgen Receptor and focally for Epithelial Membrane Antigen (EMA), whereas they were negative for Cytokeratin 7, Cytokeratin 20, Carcinoembryonic Antigen (CEA), CA125, Wilms’ tumour gene (WT1), Inhibin, CD99, Anti mullerian hormone and CD56.
Discussion
We have described the eighth case of sebaceous carcinoma arising within a mature cystic teratoma of the ovary. In the dermatopathologic field, there are lesions of sebaceous differentiation, such as nevus sebaceous, sebaceous hyperplasia, sebaceous adenoma, sebaceous epithelioma, and sebaceous carcinoma.41–45 Based on the degree of differentiation, sebaceous adenoma is categorised between sebaceous hyperplasia, in which the sebaceous lobules appear fully or early matured, and sebaceous epithelioma, in which the tumour is not made up of lobules but rather is composed of irregular cell nests and the percentage of the sebaceous cell component is much less than 50%. 15 The presence of certain pleomorphism and mitotic activity in sebaceous adenoma sometimes makes it difficult to distinguish from sebaceous carcinoma. Clearly infiltrative pattern of tumour cell nests, obvious cytological atypia, conspicuous mitotic figures and a desmoplastic stroma are helpful morphological features for the diagnosis of sebaceous carcinoma. Basal cell carcinoma with sebaceous differentiation must also be considered in the differential diagnosis. However, the presence of obvious sebaceous differentiation in nearly every tumour nest, the lack of peripheral palisading and peri-tumoral myxoid stroma excluded this diagnosis. Moreover, focal EMA staining in our case is helpful in distinguishing sebaceous carcinoma from basal cell carcinoma in which the expression of EMA is exceptional.
With regards to the behaviour of sebaceous carcinomas arising in ovarian mature cystic teratomas, no definite conclusions can be made due to the very small number of cases reported to date. In general, the prognosis of teratomas with malignant transformation is affected by the degree of tumour extension, capsular and blood vessel invasion. In our case, the tumour was restricted to the ovary and did not infiltrate capsule, blood vessels, adjacent structures or omentum. None of the sebaceous carcinomas arising in mature cystic teratomas reported until now developed recurrent disease or metastasis. One patient died due to urinary obstruction and sepsis 3 months postoperatively. 11 The other cited cases were alive at 19, 24, 16, 54 and 60 months after surgery.1,8,9,12,13
The rarity of cases with malignant degeneration within an ovarian cystic teratoma precludes a final conclusion about the optimal management of these kinds of the neoplasms. However, the main therapeutic approach of these patients remains surgery. The role of chemotherapy or radiotherapy remains unclear. Neither postoperative radiation nor adjuvant chemotherapy in patients with extracapsular disease appears to improve the survival time.19–21 Adjuvant chemotherapy with single-agent carboplatin was administered in a case of a patient with stage IIB of the disease, who remained in complete remission 24 months after treatment. 13 Post-operative chemotherapy with cyclophosphamide and adriamycin has also been given to a patient diagnosed at stage IIIB, who subsequently died due to urinary obstruction and sepsis. 11 The decision regarding treatment is more difficult when the patient is young and in earlier stages of the disease. 9 Also, in case of presumed benign dermoid cysts, care should be taken not to open the tumour and permit spillage of its content during surgical or any laparoscopic intervention. 1
In our case, the patient was at stage IA and underwent a total abdominal hysterectomy with bilateral salpingo-oophorectomy, omentectomy and appendicectomy with no adjuvant chemotherapy. The patient is well 32 months after the surgery with no evidence of recurrent disease clinically.
Footnotes
Declaration of conflicting interests
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.