
Abstract
Background and aims
Since Glasgow’s Royal Hospital for Sick Children opened in 1882, significant advances have been made in child health. Our aim was to investigate the hospital mortality that occurred in the last decade of the 19th century at Royal Hospital for Sick Children.
Methods and results
Hospital mortality records for the decades, 1890–1899, were collected from the Archives of the Royal Hospital for Sick Children. Data were extracted from the hospital inpatient records and the pathology records. In the decade 1890–1899, there were 731 hospital deaths. The main cause of death at that time in the 19th Century was infection, particularly of the respiratory tract. The age at which death occurred was analysed and the recorded cause were analysed as was the distance patients travelled to the hospital. The ratio of boys to girls and length of inpatient stay was similar to that seen in the hospital currently.
Conclusion
This study records the mortality in a children’s hospital in a large developing industrial city in the 19th century as experienced in a children’s hospital.
Introduction
In the words of Glasgow’s first full-time medical officer (Dr James Russell):-‘There is not merely overcrowding of the ground space with houses and with tenements, but there is overcrowding of the tenements with rooms, and of the rooms with persons.’ 1 On the streets, litter, polluted water, sewage and human excrement predisposed to epidemics, for which mass graves were created. In Victorian Glasgow, the majority of deaths were in children under the age of five years. Children born to the less affluent were delivered in dire conditions, the mothers often inebriated, the deliveries frequently complicated by maternal rickets and the prospect for survivors, bleak. According to an eminent Glasgow doctor of the time, the major causes of death in infants were overcrowding, insufficient exposure to light, poor drainage, inadequate nutrition, neglect, early marriage and the need for a children’s hospital. 2
The development of paediatrics in Scotland, and indeed the UK, was slow compared to other European countries. The second half of the 19th Century was the period in which Britain made significant advances in child healthcare. It was at this time that there was evolution of the term paediatrics and this field progressed without the hesitancy that had affected it previously. The first children’s hospital in the UK was London’s Hospital for Sick Children in 1852; this was half a century after Paris opened its facility and in that half century many large European cities had opened children’s hospitals.
Glasgow was one of the last major British cities to establish a paediatric hospital. Glasgow’s children’s hospital was officially opened in December 1882 in Garnet Hill (Figures 1 and 2) containing two medical wards and a surgical ward housing a total of 58 beds. No significant problems were encountered until after the admission of the first patient in January 1883.1,2 This late start may have been a benefit in a number of ways as the Hospital Board had had the opportunity of learning from the widespread experience obtained in the 21 years from the establishment of the committee which recommended a children’s hospital. Although this committee met with enthusiasm, they were blocked by local obstruction, in particular from the staff of Glasgow Royal Infirmary, the large teaching hospital in the area, resulting in the long delay from conception to delivery.
The Hospital for Sick Children, Glasgow soon after being renamed the Royal Hospital for Sick Children in 1888. This honour passed by Queen Victoria was widely appreciated. Stained glass window donated in 1882 and despite the mobility of the hospital it remains intact in the Archives of the RHSC.

Appointed as the staff of the hospital were distinguished doctors. The two visiting physicians were Professor Leishmann, the Professor of Medicine in the University of Glasgow, and Dr Finlayson, who became President of the Royal Faculty of Physicians and Surgeons. Two visiting surgeons were appointed in 1882, Sir William Macewen, Professor of Surgery, and Sir Hector Cameron, Professor of Clinical Surgery and, for many years the Vice Chairman of the General Medical Council. Hector Cameron was followed in the 1890s by Sir Kennedy Dalzell, the third staff member to have been knighted in the hospital’s history.3,4 Professor Joseph Coats was the pathologist and he had an outstanding career establishing the first Laboratory of pathology in the Western Infirmary (1896), a year before his early and untimely death. The doctors took on the posts as Honorary Visiting Staff.
By the beginning of the 20th century, however, the city’s rapidly expanding population proved extremely demanding for the now 74-bed facility and was woefully inadequate. A new 200-bedded hospital was advocated by Sir Kennedy Dalzell and by 1908, the University of Glasgow’s Principal, Sir Donald MacAllister, supported the provision of a new building at Yorkhill. The new hospital opened its doors in 1914 but part was commandeered by the military so that it was not until after World War I that it was allowed to function fully as a children’s hospital. The hospital at Yorkhill was rebuilt and the current building was opened in October 1971 with 324 beds.3–5
The infant mortality rate in Scotland at the time of opening of Glasgow’s children’s hospital was approximately 120 per 1000 live births 6 ; nowadays, the figure is around 5. 7 Numerous advances have been made over the course of the 19th and 20th centuries in healthcare: improved midwifery and obstetric care, the development and introduction of anaesthetics, antiseptics and antibiotics and the public health revolution of vaccination with overall improvements in sanitation, hygiene and housing.1,6,8
Our aim was to investigate hospital inpatient mortality at (1890–1899) the Royal Hospital for Sick Children (RHSC) in the first complete decade after the hospital opened.
Method
Documented in the annual reports of the RHSC are the details of patients who died in hospital. These records were studied for the period 1890–1899. The records from the opening of the hospital were available and the first complete decade was chosen for study of the 19th century mortality. Details extracted included the identification number, gender, date of birth, date of admission to hospital, date of death and cause of death. With this information, we could calculate age at death and total length of inpatient stay.
The distance from patients’ places of residence and their respective hospitals were calculated, measuring the distance ‘as the crow flies.’ The home residence was noted for all inpatients, not only those who died for the 1890–1899 period, listed amongst the mortality data of the decade, 1890–1899
Results
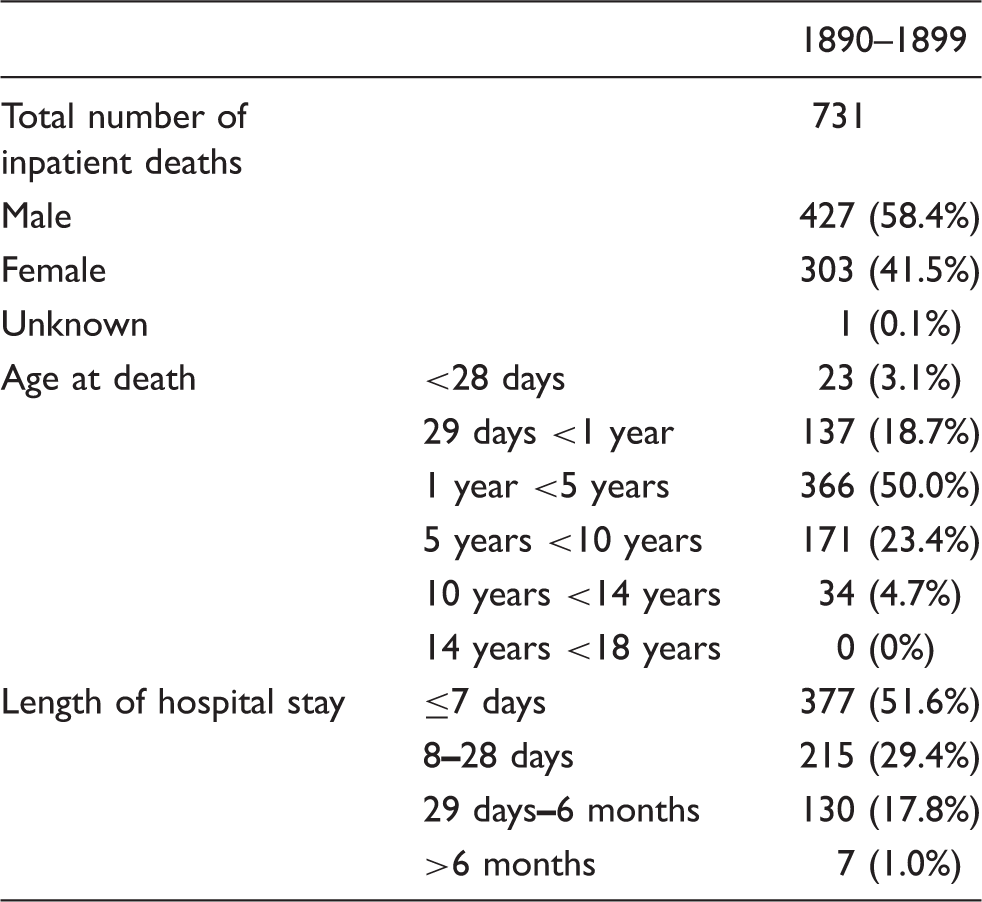
Between 1890 and 1899, there were 731 in-hospital deaths in 1232 admissions to the Royal Hospital for Sick Children (RHSC) – more than half were boys (58.4%). Death in the neonatal period accounted for 3.1% and deaths in the first year of life accounted for 21.8% of the mortality. The length of hospitalisation prior to death was that approximately half of patients’ deaths occurred within a week of admission (51.6%).
Summary of the causes of death amongst inpatients at Glasgow’s Royal Hospital for Sick Children (RHSC).
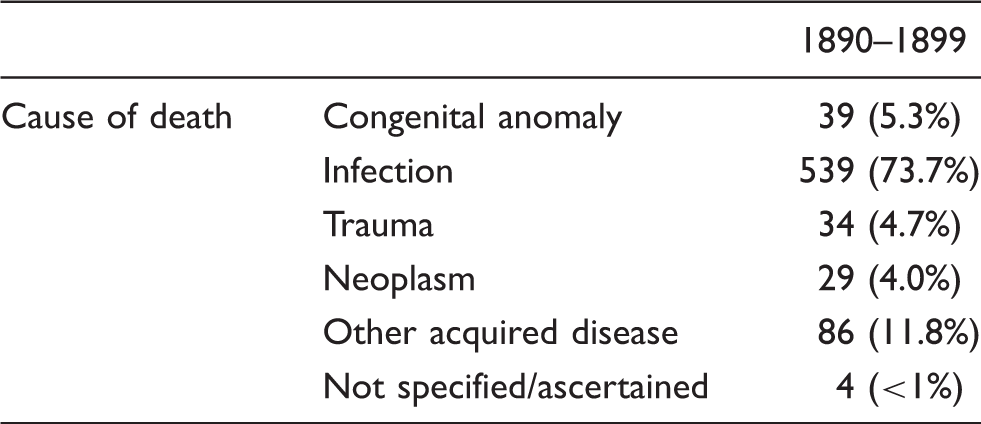
Cause of death of children (1890–1899) in Royal Hospital for Sick Children (RHSC).

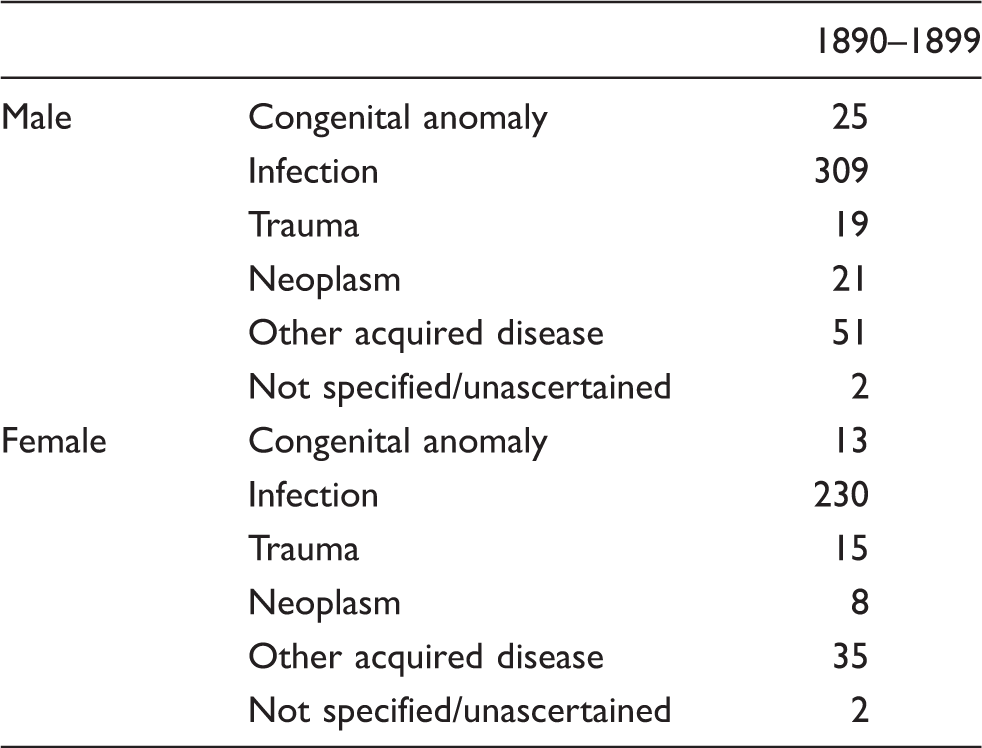
Cause of death by children by gender.
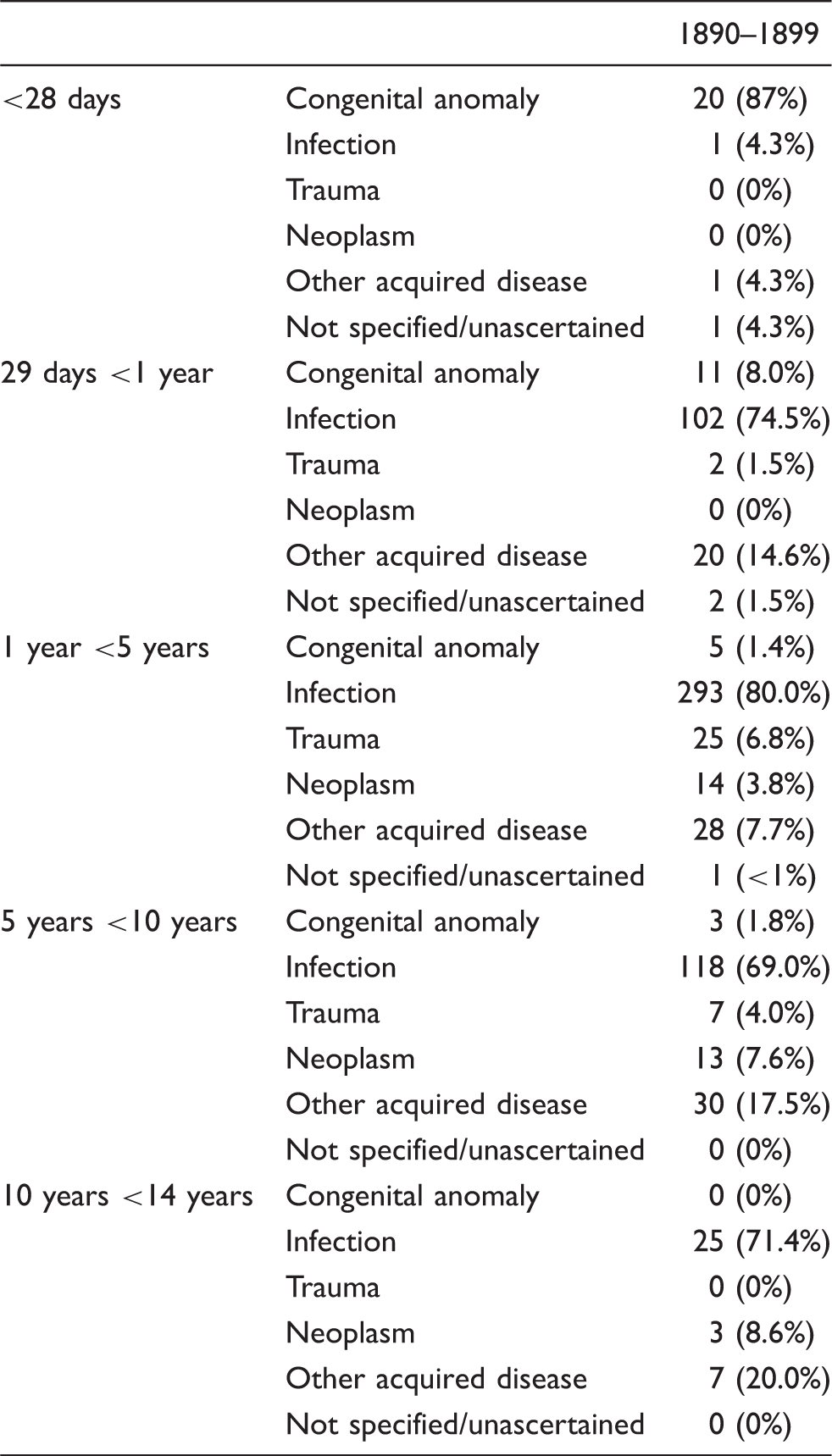
Cause of death of children by age (including % frequency amongst given age range.
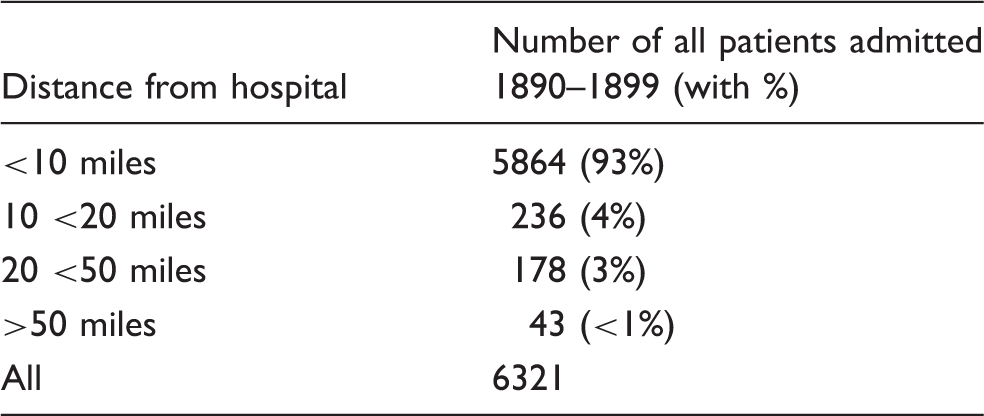
Distance families travelled to attend the Royal Hospital for Sick Children (RHSC) (N.B. the 1890
Discussion
The archives of the RHSC contain a remarkable amount of detail on the disease patterns in the 19th century and these records have been studied for the period 1890–1899. The mortality of patients admitted to the RHSC was 16% amongst the medical patients and 8% in the surgical wards. Attendances and admissions in the first two decades of the hospital show that more patients attended the physicians than the surgeons but that pattern had changed by the start of the 20th century. Thereafter, there were consistently more patients attending the surgical services than the medical.
The Board of Management of the hospital had determined that the hospital should serve children aged between 2 and 12 years. Children under 2 years presented difficulties in management and their admission was therefore discouraged but the clinicians did not strictly follow that direction. The number of infants where there was such a high mortality in the 19th century was slowly falling. Restrictions by the Board on the under 2s was justified by the difficulties experienced in other children’s hospitals before the RHSC was opened. The clinicians did accept an increasing number of patients under two years and the surgeons were the greater ‘sinners’ in this respect.
Gradually, the recommendation was so frequently ignored that it was informally dropped from the regulations. Teenagers were expected to attend adult facilities. This limit did not change for decades. Thus these limitations did affect the mortality recorded in hospital which was not representative of the general population. It explains the low number of infants recorded as dying from congenital anomalies. The infant mortality rate was twentyfold that of the 21st century, but infants with congenital anomalies were largely excluded from admission to the RHSC. The congenital anomalies recorded infrequently in the RHSC figures did not reflect their true incidence in the community. The infant mortality rate was gradually falling in the latter part of the 19th century and this was related to other factors rather than simply the addition of a children’s hospital. A variety of other social factors at that time were being contributed to the modest overall reduction in childhood mortality in the latter part of the 19th century.
Respiratory diseases, particularly tuberculosis, accounted for much of the disease burden and deaths in Victorian Glasgow. In 1870, William Gairdner stated that, ‘…the disease of the respiratory organs, which, taken in aggregate, caused considerably more than a third of the whole mortality.’6,8 This is certainly reflected in the mortality records of the first decade of Glasgow’s children’s hospital where approximately 1 in 4 inpatient deaths were attributed to tuberculosis. Viral infections of the respiratory tract, such as pertussis, as well as bacterial infections like Scarlet fever, along with their complications, were other major causes of death. Many lethal infections of other bodily sites were attributed to tuberculosis, such as meningitis and osteomyelitis. The second half of the 19th century had been a period in which there was a great expansion in the knowledge on infection but in which there were limited therapies available to combat infections.
In the 19th century, the development and introduction of widespread vaccination programmes and massive improvements in standard of living have likely been responsible for the noteworthy decline in infectious diseases into the 20th century. The controversial introduction of vaccination which in retrospect such outstanding results was supported by the Royal faculty of Physicians and Surgeons in Glasgow for many decade and was then also supported by the Royal Infirmary in the city.
A lack of diagnostic precision is undoubtedly present amongst the mortality records of the 19th century. Investigations were few, and for instance, the first X-ray machine, donated by Dr Fleming, was not given to the children’s hospital until 1900. The first ‘radiologist’ was Dr John Gilchrist who had introduced radiology to Scotland and he was appointed as the Honorary Medical Electrician to the RHSC. There was a similar lack of laboratory support and the first Professor of Pathology was appointed by the University of Glasgow in the Western Infirmary in 1893. Joseph Coats MD was the Honorary Pathologist at the RHSC having been appointed in 1882. His first pathological department was opened in 1896 in the Western Infirmary and laboratory medicine gradually developed.1,3–6 There was a much greater number of post-mortem examinations in the late 19th century, compared with the present day where their value has often been forgotten.
Disease patterns change, but it is difficult to dispute that some conditions emerge and become more prevalent. In the decade 1890–1899, the total number of cases of acute appendicitis diagnosed in the children’s hospital did not exceed single figures. Appendicitis was rarely diagnosed before the 20th century, but then the prospective King, Edward VII, developed the disease in 1902 and his coronation was postponed until he recovered from removal of his inflamed appendix. 9 This diagnosis rapidly increased over the succeeding generations. A further example is nephroblastoma. The original description by Wilms on the tumour widely known by his eponym was only published in 1900. 10 Prior to this, the malignant tumour was often confused with a kidney infection. It is likely that this was a result of misdiagnosis in the 19th century rather than a natural increase in the incidence of the disease.
The tumour deaths presented suggest that there has been little, if any, progress in the management of malignancy over the 20th century; however, this likely reflects the lack of diagnostic facilities in the first series. Leukaemia is today the most frequently diagnosed childhood malignancy but accounted for less than 1% of all childhood deaths in the 1890s. Even in much later decades, the mortality associated with malignancy was so rapid that death occurred in patients before they even attained hospital admission. In fact, recent decades have shown remarkable improvement in survival in all groups of tumour patients though cancer still does result in a number of childhood deaths annually, but the apparent high mortality is from aggregation of patients into specialised units.
Whilst trauma still accounts for almost 1 in 20 childhood deaths, the mechanism of lethal injury has changed dramatically. The vast majority of inpatient trauma deaths were attributable to burns in the 1890s; but the fall in the current decades may be attributed to the introduction of flame-proof clothing, central heating and fire safety legislation, such as that on, the Buildings Act 1959 and the Oil Heaters (Safety) Regulations 1977, the latter being notorious for causing paediatric burns historically. Polytrauma is the cause of the current traumatic deaths. Despite the introduction of road safety legislation, the ever-expanding popularity of the automobile over the 20th century is undoubtedly responsible for the higher number of fatal RTAs.
This exponential rise in road users and better public transport explain the fact that the distance that patients have travelled to reach their respective hospital site has increased. Furthermore, Glasgow’s RHSC is now a tertiary paediatric centre, so families travel afar to access services not available elsewhere in Scotland. But it was surprising how far many travelled in the 19th century.
This study has recorded the hospital mortality in a children’s hospital in the latter part of the 19th century with the gradual development of paediatrics – a new specialty – designed to care for the health needs of the younger generation in society. The development of paediatrics over the course of Glasgow’s RHSC’s 130-year history as the hospital undergoes a further relocation over the next few years. It remains uncertain whether improvement in child healthcare in Glasgow can continue at the rate it did in the last century as the children’s hospital becomes part of a large medical facility in the Southern General Complex and Dr James B Russell’s opinion in the 19th century be proven wrong. His view was ‘thoroughly disagreeing with the medical establishments view that children should be treated in general hospitals, he had played an energetic role in the new hospital from the outset, travelling to England to interview the short leet of candidates for the post of matron, and constantly testing the milk supplies – finding, for example, the level of boracic acid to be perfectly intolerable.’ 11
Conclusion
This investigation shows a clear difference in disease patterns and in causes of death over the century to the present day. Although the proportion of deaths fell into similar groups further breakdown showed the marked change in the causes of infection or in the aetiology of trauma.
Contributors
PSC collected the study data and contributed to all sections of the article. DGY conceived the study concept and contributed to the introduction and discussion. We declare that we have no conflict of interest nor did we receive funding.
Footnotes
Declaration of conflicting interests
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.