
Abstract
A patient presented having a one-week history of recurrent falls and confusion and weight loss over an unspecified period of time. A chest radiograph revealed bilateral pleural effusions and the patient was treated for community acquired pneumonia. His weight loss and suspicion of malignant disease prompted computer tomography to be conducted. This revealed widespread mediastinal and oesophageal adenopathy. An echocardiogram showed a large hyperechoic mobile mass. Coronary angiography showed complete occlusion of the left anterior descending and right coronary arteries. He underwent two-vessel coronary artery bypass grafting and an atriotomy to excise the myxoma. He experienced no operative complications and no neurological deterioration and was discharged home three weeks later in sinus rhythm. Myxomas can duplicate a broad array of cardiorespiratory symptoms and signs and can often escape detection by being picked up as an incidentaloma.
Introduction
Myxomas are the most common benign cardiac tumours, as lipomas and fibromas occur less frequently, and >75% occur in the left atrium. They are typically pedunculated being particularly anchored to the fossa ovalis of the interatrial septum (IAS). Myxomas can cause a myriad of symptoms and signs, duplicating common cardiac disease processes including congestive heart failure and creating an additional heart sound which quickly follows S2. Echocardiography (ECHO) is a diagnostic medium of choice, as it reveals the shape and any potential valvular obstruction. Complications can include sudden cardiac death, due to obstructing and sealing a valve and by increasing the pulmonary capillary wedge pressure.
Clinical summary
An 82-year-old man presented having a one-week history of recurrent falls and confusion. He had a productive cough and haemoptysis on a background history of ischaemic heart disease (IHD) and type II diabetes mellitus. The patient reported weight loss over several months and intermittent non-specific left-sided chest pain. Attempts by his general practitioner to help him cut down on his alcohol excess and to permit basic investigations had proved unsuccessful. On admission, his observations included a temperature of 38.0℃ and saturations of 93% on 2 L of oxygen. On examination, positive findings included reduced air entry, bilateral crackles up to the mid zones, peripheral oedema but no cervical lymphadenopathy.
An electrocardiogram showed first-degree heart block and a chest radiograph revealed bilateral pleural effusions. Initial bloods revealed a leukocytosis (14.3 × 109) and the patient was treated for community-acquired pneumonia (CURB-65 = 3). Ongoing investigation for his recurrent falls in the form of computer tomography (CT) revealed no intracranial pathology.
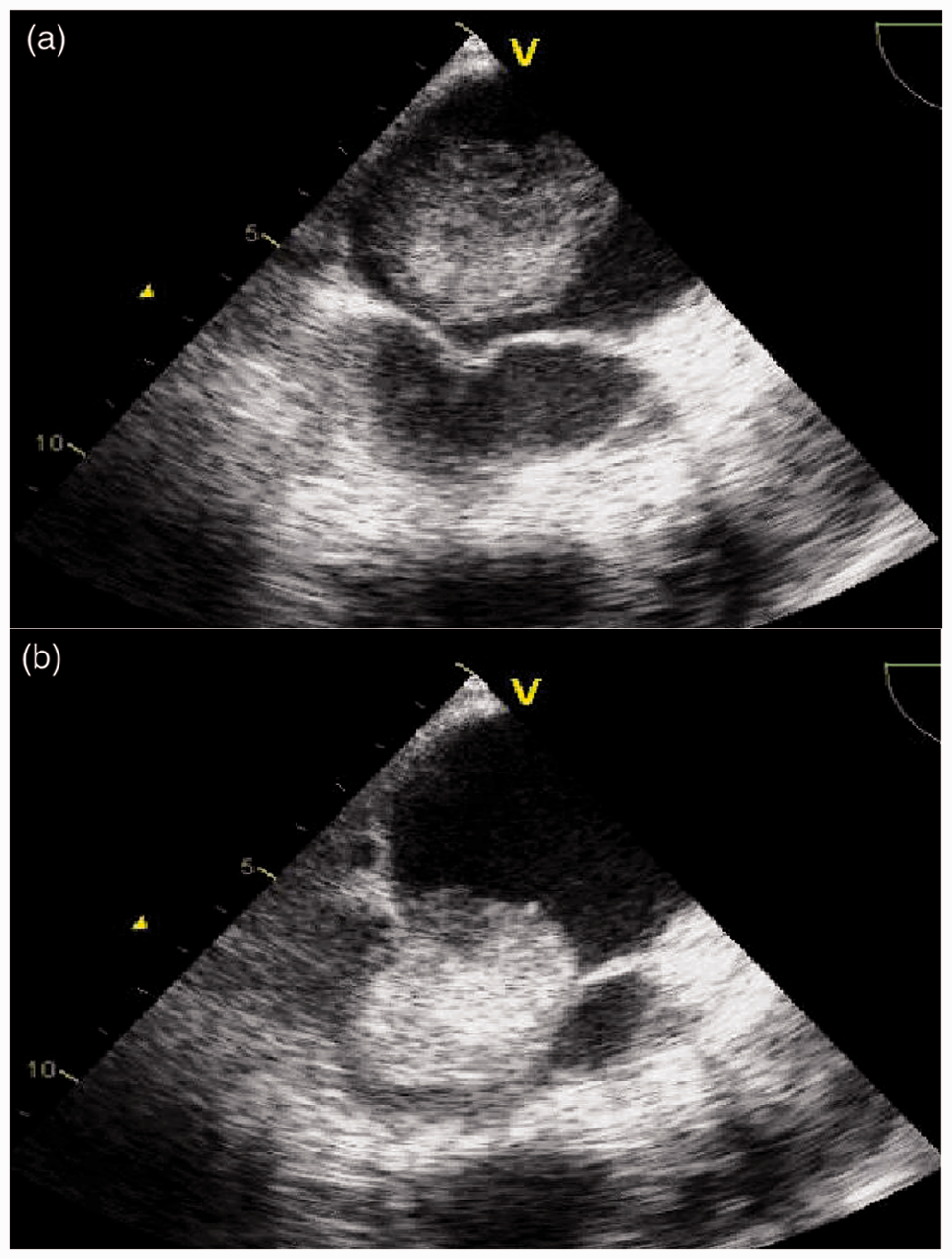
His weight loss and suspicion of malignant disease prompted a CT to be conducted. This revealed widespread mediastinal and oesophageal adenopathy (Figure 1(a)) and a large left atrial lesion (Figure 1(b)). An ECHO showed a large hyperechoic mobile mass measuring 3 × 5 cm (Figure 2(a)). It was attached to the IAS causing severe obstruction of the mitral valve and left ventricular systolic impairment (Figure 2(b)). This was accompanied by dilatation of the left atrium (5.3 cm) and paradoxically of the left ventricle (6.3 cm). The mobile mass was confirmed to be an atrial myxoma.
(a) High-resolution computer tomography (HRCT; coronal) before the operation showing particularly large mediastinal lymphadenopathy and oesophageal adenopathy; (b) HRCT (coronal) before the operation showing an unusual mass in the left atrium that almost occupies the entire chamber. (a) ECHO (trans-thoracic) showing a well-defined left atrial myxoma sitting above but particularly close to the mitral valve; (b) ECHO (trans-thoracic) showing the myxoma completely occluding the mitral valve during cardiac diastole (left ventricular filling).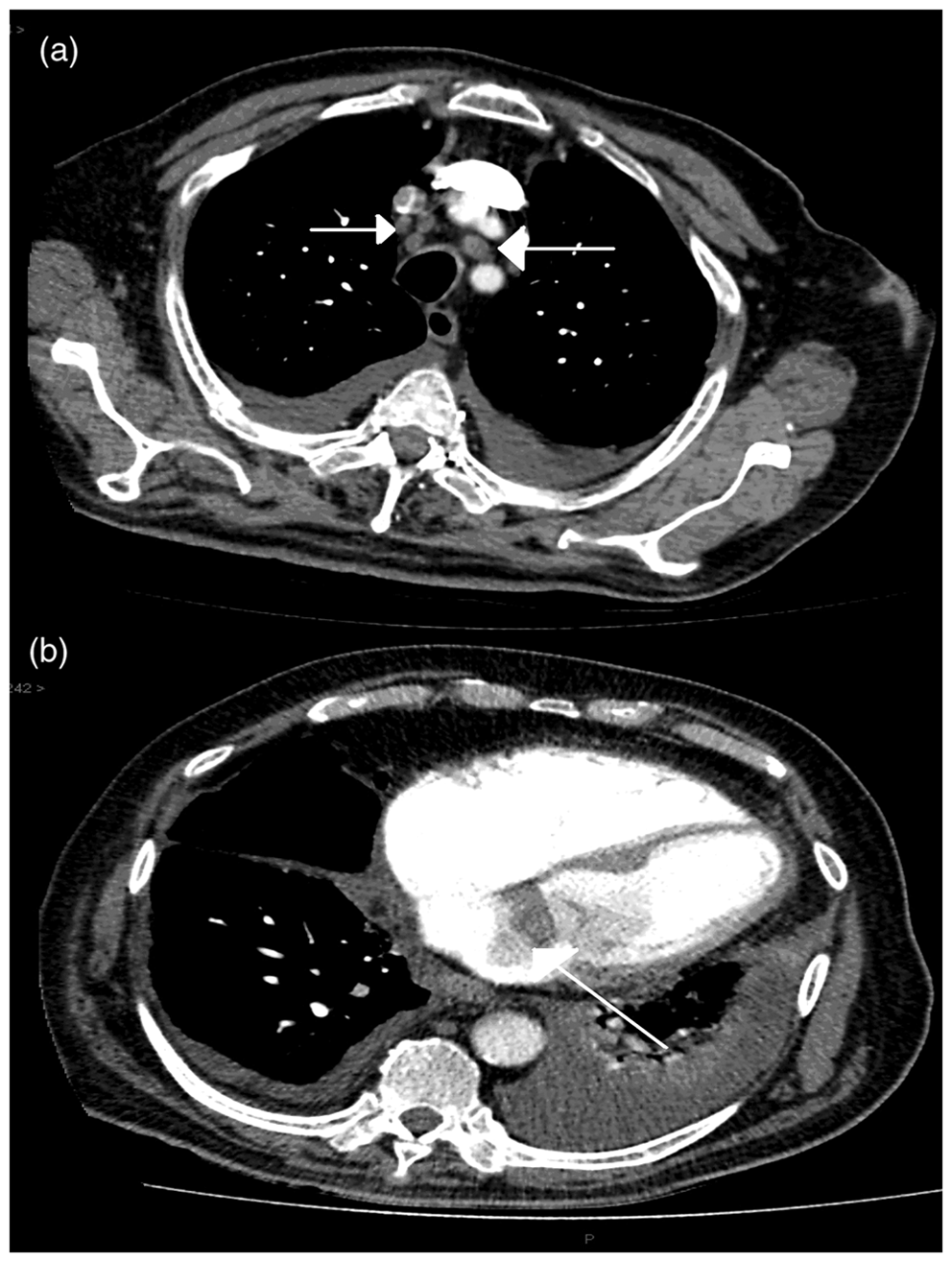
Endoscopy confirmed Barrett’s oesophagus but biopsies did not confirm malignancy. Pathological examination of nodes extracted at mediastinoscopy revealed the nodes to be highly vascular but not malignant. He began to decompensate during this operation enduring a systolic BP <60 mmHg. Due to his rumbling history of IHD, he was discussed at our cardiac and cardiology multi-disciplinary meeting following more invasive investigations.
Coronary angiogram showed complete occlusion of the left anterior descending and right coronary arteries. Despite being 82 years old and presenting as a medical emergency, experiencing cardiac instability during a relatively minor surgical procedure, he was optimised for a coronary artery bypass graft (CABG).
Surgical intervention included great saphenous venous two-vessel CABG and an atriotomy to excise the myxoma (Figure 3(a)). The pathological specimen was gelatinous and nodular in appearance, revealing potential for distant embolism (Figure 3(b)). He was extubated the next day having experienced no operative complications and no neurological deterioration and was discharged home three weeks later in sinus rhythm.
(a) Operative image of the excised myxoma clamped on a pair of Robert’s forceps above the sternotomy and bypass tubing; (b) Pathological image of the excised myxoma against a measuring tape revealing its size and gelatinous consistency.
Discussion
Congestive heart failure secondary to myxomatous disease can be asymptomatic and remains undetected for an unknown period of time. 1 Myxomas constitute the most common primary cardiac tumours, occurring at an incidence of 0.0017–0.19%, being often solitary arising in any chamber but having 75% preponderance for the left atrium and 20% for the right atrium. They usually occur during the fourth and seventh decades and ∼ 7% of cases form a part of an autosomal dominant syndrome known as Carney complex, which is characterised by myxomas, hyperpigmented skin lesions and extracardiac tumours including pituitary adenomas, breast fibroadenomas and melanotic schwannomas. 2
The clinical presentation encompasses a triad characterised by valvular obstruction, emboli and constitutional symptoms including fever and weight loss. 3 Myxomas can be lethal depending on their size, mobility and anatomical position and often mimic common cardiac diseases including dyspnoea due to heart failure, sudden death due to complete mitral valve obstruction and rarely neurological symptoms due to embolic stroke. 4 An ECHO is the most important diagnostic investigation due to ease of access but it does possess some disadvantages including comparative operator experience, limited cardiac views and patient positioning. 2 Coronary angiography should be considered in patients over 40 years of age. Once surgical excision is conducted, the long-term prognosis is excellent and recurrences are rare.
Myxomas are spherical lesions being lobular or smooth and are often heterogeneous possessing cystic areas of a polysaccharide myxoid substance, haemorrhagic phenomena and haemosiderin, fibrosis and calcification. 2
On occasion myxomas may undergo malignant transformation. Our case shows that a myxoma almost occupying the entire left atrial cavity and causing severe mitral valve stenosis, left atrial diltation, severe pulmonary hypertension, an increased risk of valvular obstruction, neurological disease due to embolic phenomona and sudden respiratory and cardiac death can go undetected for an unspecified period of time. His relative asymptomatic history highlights the silent nature of myxomas and their often incidental diagnosis.
Conclusion
Our case highlights the value of ECHO in the investigation of the breathless patient and the importance of considering rare diagnoses in everyday practice. 5 Elderly patients have a myriad of underlying disease processes that can be simply benign. In an increasingly ageing population, the potential for unexpected diagnoses and surgical management from a seemingly common medical presentation is becoming more apparent.
Footnotes
Acknowledgements
The authors wish to thank NHS Lothian and the Department of Cardiothoracic Surgery at the Royal Infirmary of Edinburgh.
Declaration of conflicting interests
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.