
Abstract
Background
Transperineal prostatic biopsy is firmly established as an important tool in the diagnosis of prostate cancer. The benefit of additional imaging (magnetic resonance imaging) to target biopsy remains to be fully addressed.
Methods
Using a cohort of consecutive patients undergoing transperineal template mapping biopsies, we studied positive biopsies in the context of magnetic resonance imaging findings and examined the accuracy of magnetic resonance imaging in predicting the location of transperineal template mapping biopsies-detected prostate cancer.
Results
Forty-four patients (mean age: 65 years, range 53–78) underwent transperineal template mapping biopsies. Thirty-four patients had 1–2 and 10 patients had ≥3 previous transrectal ultrasound scan-guided biopsies. The mean prostate-specific antigen was 15 ng/mL (range 2.5–79 ng/mL). High-grade prostatic intraepithelial neoplasia was found in 12 (27%) patients and prostate cancer with Gleason <7, 7 and >7 in 13, 10 and 8 patients, respectively. Suspicious lesions on magnetic resonance imaging scans were scored from 1 to 5. In 28 patients, magnetic resonance imaging detected lesions with score ≥3. Magnetic resonance imaging correctly localised transperineal template mapping biopsies-detected prostate cancer in a hemi-gland approach, particularly in a right to left manner (79% positive prediction rate), but not in a quadrant approach (33% positive prediction rate).
Conclusion
Our findings support the notion of magnetic resonance imaging-based selection of patients for transperineal template mapping biopsies and that lesions revealed by magnetic resonance imaging are likely useful for targeted biopsies.
Introduction
Prostate cancer (PC) is a global health issue and a very common cause for premature death in men worldwide, with approximately 900,000 new cases identified in 2008. It is currently the second commonest cancer-related death in men. 1 Digital rectal examination, serum prostate-specific antigen (PSA) measurement and transrectal ultrasound scan (TRUS)-guided prostate biopsies have been the standard approach in the detection of PC. More recently, important developments have been made in functional imaging and in techniques to perform prostate biopsies, including transrectal saturation biopsies 2 and transperineal template prostatic biopsies.3,4 A transperineal template mapping biopsies (TTMB) approach reduces infection risks associated with a transrectal route while allowing prostatic biopsies to be obtained comprehensively, including the anterior part of the gland. Using such a method, a 55% cancer detection rate has been reported despite previous negative transrectal biopsies. 5
The application of functional imaging (particularly multiparametric magnetic resonance imaging (MRI) to incorporate T1/T2-weighted, diffusion-weighted imaging (DWI) and dynamic contrast-enhanced imaging) in conjunction with prostatic biopsies is receiving much interest.6,7 Targeted biopsy through magnetic resonance guidance or MRI-ultrasound fusion offers unraveled accuracy in the detection of PC.8,9
Functional imaging-guided (targeted) prostate biopsy is beginning to alter clinical practice. However, it remains to be fully determined which patient subgroups would benefit from such an approach most. In our cohort analysis, we tested whether MRI-identified lesions may avoid the need for formal transperineal template mapping prostate biopsies.
The purpose of this study was to test whether MRI scans of the prostate performed to routine clinical standard are adequate to guide limited TTMB to regions or quadrants within the prostate.
Patients and MRI method
Consecutive cases of patients undergoing TTMB in a tertiary referral centre within the West of Scotland were reviewed. All procedures were performed by a single surgeon (HYL). MRI scans of the prostate and pelvis were performed using the GE HD× 1.5 T with an eight-channel cardiac array coil, according to established clinical protocols: (1) T2; axial, coronal and sagittal; (2) 3-mm slices field of view 18 × 18 (axial seven coronal) 25 × 25 (sag); and (3) diffusion sequences slice thickness 4 mm b values 0 and 1400. A pelvic phased-array coil was used.
Analysis of concordance between MRI findings and histology from TTMB
Report from each MRI was reviewed, and identified lesions were categorised as previously described.14 Score of MRI revealed lesions are as follows: 1 – no lesion, 2 – possible lesion, 3 – probable lesion of clinical significance, 4 – suspicious lesion and 5 – lesion highly likely to be malignant. The concordance between MRI- and TTMB-derived histology was then analysed based on data extracted from the reports of these two investigations. Histology from TTMB were considered in the context of their grid location: (i) urethra = column ‘G’; (ii) columns ‘A’ to ‘F’ represent the right halves of the prostates; and (iii) columns ‘H’ onwards represent the left halves of the prostates. If both MRI and TTMB findings suggested the presence of cancer in the same prostatic ‘regions’ (or ‘zone’) within a hemi- or quarter-gland context, MRI and TTMB were considered concordant in these cases.
Results
Stratification of patients by number of previous TRUS biopsies.
Prostate cancers identified by TTMB and their associated Gleason score.

MRI scans of the prostate and pelvis (either prior to or after TTMB) were carried out in 42 patients: 29 patients had MRI prior to TTMB and 22 patients had MRI following TTMB. Nine patients had MRI of the prostate and pelvis both before and after TTMB. Eight of these nine-paired MRI scans were highly concordant in localising detectable lesions to the same quadrants within the prostate. In the ninth case, again showing good concordance, both pre- and post-TTMB scans revealed no identifiable lesions.
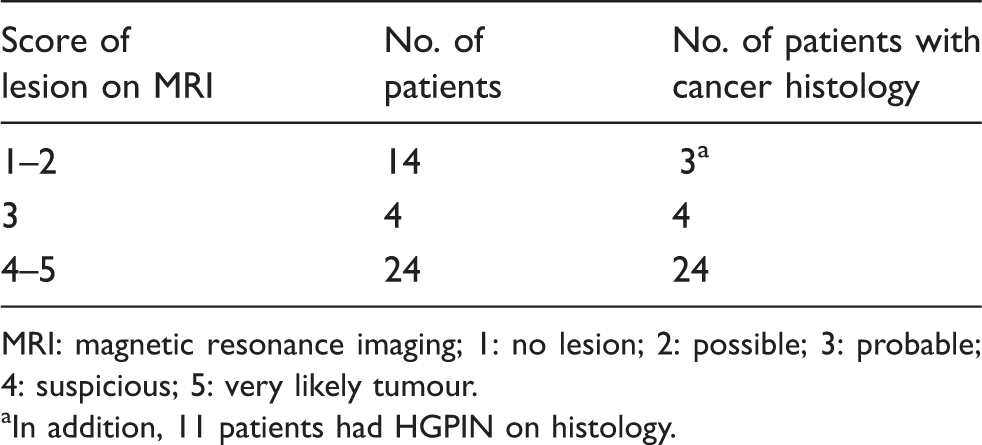
Suspicious lesions on MRI scans (MRI score ≥3) were identified in 28 patients (Table 3). Figure 1 illustrates matched images of a right peripheral lesion (MRI score 5) seen on T2, DWI and apparent diffusion coefficient (ADC) maps from one patient. Of note, all of these 28 patients were found to be positive of PC by TTMB. In contrast, low MRI scores (1 and 2) were associated with low risk of PC, with only three out of 14 patients positive for PC by TTMB. We then investigated the concordance between MRI revealed lesions (MRI score ≥3) and TTMB-identified PC in terms of their (quadrant- or hemi-gland) location within the prostate. First, analysing the data from MRI and histology using laterality (right vs. left hemi-prostate, R/L), 25 of 28 (60%) cases showed correct association between MRI-detected lesion (MRI score ≥3) and histology of PC, and thus, lesions seen in MRI were confirmed by histology in the respective left or right halves of the prostate. For those patients with no convincing lesions seen on MRI (score ≤2, 8 of 42 (19%)), TTMB only revealed benign prostatic tissue. Together, MRI correctly predicted the outcome of TTMB in 33 (= 25 + 8) of 42 cases (or positive predictive value at 79%) in a right–left laterality analysis. In the remaining nine patients, MRI and TTMB histology did not show concordance, with seven PC identified by TTMB while MRI was either negative (n = 2) or revealed lesions in the wrong side of the prostate (n = 5), thus suggesting a negative predictive value in nine of 42 (21%) patients.
Multiparametric MRI illustrates matched images of a right peripheral lesion (MRI score 5) seen on (a) T2, (b) DWI and (c) ADC maps from one patient. Score of pre-TTMB MRI revealed lesions. MRI: magnetic resonance imaging; 1: no lesion; 2: possible; 3: probable; 4: suspicious; 5: very likely tumour. aIn addition, 11 patients had HGPIN on histology.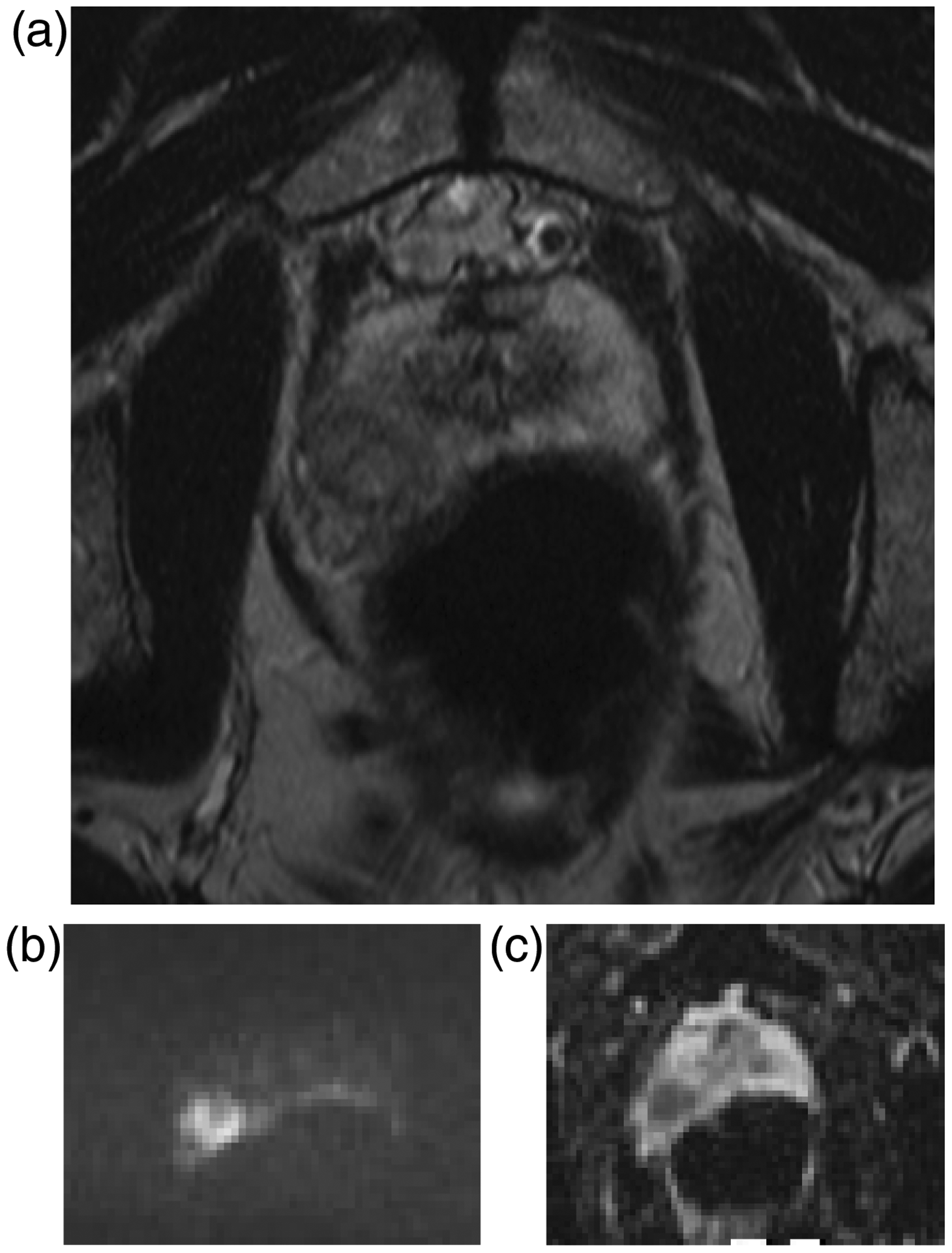
Similarly, analysing for concordance in an anterior-versus-posterior (A/P) context between MRI and histology, 17 of 42 cases (40%) correctly identified lesions (score ≥3) that were subsequently confirmed by histology in the respective A/P compartment. In eight of 42 (19%) patients with no convincing lesions seen on MRI (score ≤2), TTMB only revealed benign prostatic tissue. Together, MRI correctly predicted the outcome of TTMB in 25 (= 17 + 8) of 42 cases (or positive predictive value at 60%) in an anterior–posterior analysis. In 17 cases (40%), we did not observe concordance in A/P analysis between MRI-detected lesions and TTMB-derived histology. Further refining the analysis to quadrants of the prostate gland, combining MRI and TTMB data showed concordance in only 14 of 42 (33%) of the cases. Hence, our data suggest the usefulness of MRI-directed TTMB in a hemi-gland approach, particularly in a right to left manner, but not in a quadrant approach in identifying PC without whole gland mapping biopsies.
Discussion
Here, we present the analysis of 44 consecutive patients who underwent TTMB. MRI-ultrasound fusion-guided biopsies have the potential to aid accurate targeting of the index lesion(s) detected by MRI as well as the ability to return to a prior biopsy site with confidence. However, such an approach requires significant investment and changes in (urologic and radiologic) practice. Here, we report our findings on the feasibility of a simple pragmatic approach to apply information from MRI to limit TTMB to ‘regions’ of the prostate without a prior cognitive targeting of specific part(s) of the prostate.
Multiparametric MRI scan of the prostate (T2 weight imaging, DWI and ADC maps) was performed to routine clinical protocol, and data were extracted to corroborate with TTMB-derived histology. Our PC detection rate was 70%, including cancers of all Gleason scores, which is in keeping with the literature. 10 Apart from two patients with lower urinary tract symptoms who developed acute retention of urine, we observed no significant complications. As expected, the main indication for TTMB was abnormal PSA levels with previous negative TRUS-guided biopsies. TTMB is considered particularly useful to identify anterior PC that may not be covered by conventional 10–12 core TRUS-guided biopsies.5,11 Indeed, 20 out of 31 cases (65%) had an anteriorly located prostate tumour. In our series, consistent with reports on MRI-guided biopsy,12,13 TTMB have similar cancer detection rates regardless of the number of previous TRUS biopsies.
MRI of the prostate is increasingly carried out in specialised centres, in the hope to identify clinically significant disease and anterior tumours. Our findings will contribute to the debate in how best to manage patients with previous negative prostatic biopsies who are undergoing MRI.8,10 Specifically, data presented in this report would support the notion of targeted or limited mapping biopsies in those patients with detectable prostatic lesion(s) on MRI. Using a right–left split of the prostate, nearly 80% of patients were correctly predicted by MRI findings. It is worth noting that, of the 31 patients positive for PC on TTMB, 25 patients (80%) with PC were correctly identified when only (the right or left) half of the prostate as guided by MRI findings were biopsied.
Besides the need for financial and logistic considerations, for routine MRI prior to prostatic biopsies to be embedded into routine clinical practice, a number of technical and platform issues will need to be addressed: comparison and benchmarking of data across different manufacturing MRI systems, the use of appropriate software(s) to meaningfully support comparison of data, protocols and criteria used for the functional parameters as part of appropriate standards of procedures. Besides consensus on these issues, there is also the need for adequately objective means to categorise detectable lesions in terms of their size and level of likelihood of cancer. 14 In our series, T2, DWI and ADC maps were part of our MRI protocol. We did not carry out routine contrast-enhanced MRI which may further improve our data. Overall, we have demonstrated that without additional investment or training, an approach to limit TTMB as guided by MRI to the right or left half of the gland may reduce the number of biopsies required, while a more limited approach to individual prostatic quadrants may not be as efficient in diagnosing PC.
Footnotes
Declaration of conflicting interests
The authors declare no conflicts of interest.
Funding
This study was funded as part of the NHS service and the reported data were based on audit from our clinical record.
Authors’ contributions
AM and SM are joint first authors. AM, SM and HYL designed the study; SF and JS were responsible for pathology reporting and review; GB was responsible for radiology reporting and review; and HYL carried out the described biopsy procedure.