
Abstract
Aggressive posterior retinopathy of prematurity is identified as a rare, rapidly progressing and severe form of retinopathy of prematurity (ROP). Here, we report the diagnosis and treatment of aggressive posterior retinopathy of prematurity (APROP) in two of the triplets born at low birth weight and small gestational age. A case concerning two triplets who were born at 31 weeks’ gestational age with low birth weight and reached bilateral threshold APROP was reported. The ROP of triplets A and B had the characteristic features of aggressive diseases, which were posterior location, prominence of plus disease and rapid progression. Low birth weight and small gestational age, multiple pregnancies, pregnancy-induced hypertension and older age of the mother might account for the presentations of APROP. These cases demonstrate the importance of early screening and diagnosis in APROP infants. Prompt and adequate laser photocoagulation with a large number of high-intensity closely performed spots and early retreatment could be effective and safe for preventing the progression of APROP with plus disease in zone 1 or 2 in premature triplets.
Keywords
Introduction
Aggressive posterior retinopathy of prematurity (APROP) is identified as a rare, rapidly progressing and severe form of retinopathy of prematurity (ROP). Here, we report the diagnosis and treatment of APROP in two of the triplets born at low birth weight and small gestational age.
Case report
The mother of the infant triplets was a 38-year-old female who suffered pregnancy-induced hypertension (PIH). Triplet A was a female infant who was born at 31 weeks gestation with a weight of 1300 g. ROP was present when she was screened at 33.5 weeks gestation. Bilateral threshold ROP was reached at 34 weeks gestation (zone 2 with plus disease), and the physician made the APROP diagnosis. Both eyes were immediately treated with an argon ion laser via a 30-diopter lens anterior to the ridge (340-mW intensity/200-ms duration; 1092 burns oculus dexter (OD) and 906 burns oculus sinister (OS)) (Figure 1(a, b)). Regular follow-up was conducted once a week. Triplet A’s platelet count before laser treatment was 74 × 109/L. No adverse cardiovascular or other complications were noted during or after treatments. The follow-up of fundus in both eyes at month 10 showed well-regressed ROP in the lasered retinal periphery.
Postoperative view demonstrated aggressive retinal photocoagulation with a large number of dense spots improves the hypoxic conditions of the retina (a: right eye of triplet A; b: left eye of triplet A; c: right eye of triplet B; d: left eye of triplet B).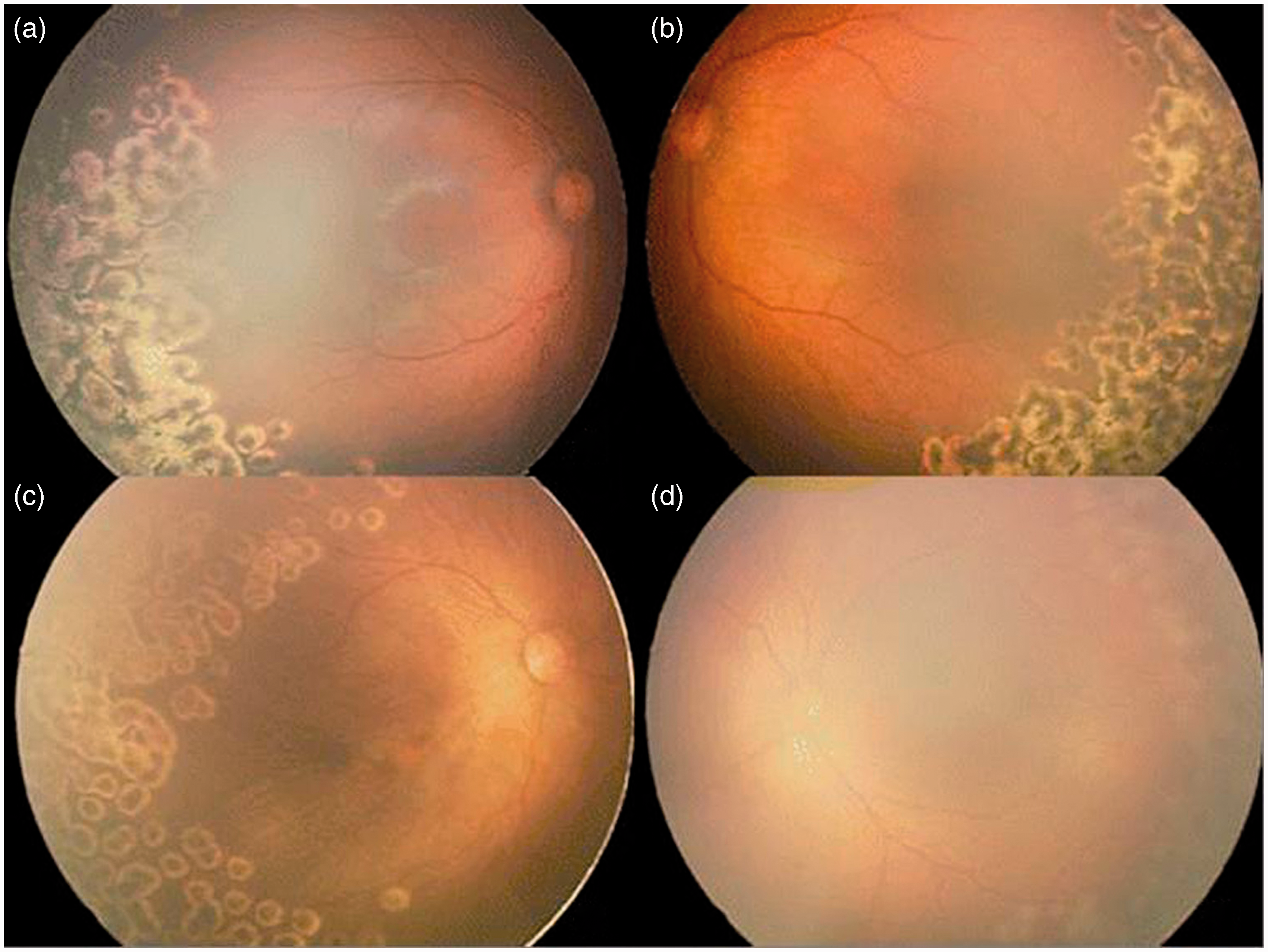
Triplet B was a male infant with a birth weight of 1160 g who reached bilateral threshold APROP on his screening examination at 35 weeks of gestation (zone 1 with plus disease bilaterally). Laser treatment (380-mW intensity/200-ms duration; 960 burns OD and 1404 burns OS) was performed the next day (Figure 1(c, d)). The preoperative platelet count was 211 × 109/L. No systemic complications were noted. APROP of both eyes regressed gradually throughout the 10-month follow-up period.
Triplet C had more critical systemic diseases than his siblings at birth. Diagnoses of septic shock and acute congestive heart failure were made on the sixth day. The infant died of respiratory and circulatory failure without a ROP screening examination.
Discussion
Most experts agree that early diagnosis and correct treatment play a vital role in the recovery of APROP infants. However, to date, there has been no literature regarding the assessment of risk factors for APROP occurrence using logistic regression analysis. We therefore reported this case and summarised the following controversial risk factors of APROP.
Platelet count was thought as one of the issue of risk factors of APROP. Vinekar et al. 1 found that a platelet count of <100 × 109/L was associated with APROP due to suboptimal scavenging of excess vascular endothelial growth factor A present in APROP infants. In our cases, the platelet count prior to laser treatment of triplet A was <100 × 109/L, while that of triplet B was more than 100 × 109/L.
The role of multiple births in ROP is still unknown. Some study showed that the morbidity of ROP was not significantly different between multiple infants and singletons when matched for gestational age. 2 However, a study of 363 infants suggested that singletons had a significantly higher rate of advanced ROP (stages II–III) compared with multiple premature. 3
The rate of ROP was found to be higher in infants whose mothers suffered from PIH. 4 With respect to retinopathy, live-born preterm infants of nonpreeclamptic mothers had better results compared to preeclamptic mothers, when gestational ages at birth were matched. 5 However, a recent study showed that preeclampsia was related to a reduced risk of ROP in premature infants. 6 The mother in our cases was over 35-year-old and had PIH, which could lead to premature delivery and intrauterine hypoxia of the unborn fetuses.
Some hold the view that APROP requires aggressive retinal photocoagulation with larger number of dense spots to stop progression of fibrovascular proliferation. 7 A recently published study of prospective and interventional case series over 10 years showed that APROP in zone 1 could lead to favorable outcomes with early screening, timely and sufficient laser photocoagulation (indication of plus disease with disordered shunt vessels in zone 1) and frequent follow-up until absolute regression. 8 However, another widely held point of view is that early vitrectomy approach is effective at avoiding disease progression. 9 Indirect laser photocoagulation combined with intravitreal bevacizumab injection may slow progression of APROP and accelerate the regression of the disease, but may give rise to tractional retinal detachment in some patients. 10
In our cases, the ROP of triplets A and B had the characteristic features of aggressive diseases, which were posterior location, prominence of plus disease and rapid progression. Low birth weight and small gestational age, multiple pregnancies, PIH and older age of the mother might account for the presentations of APROP. These cases demonstrate the importance of early screening and diagnosis in APROP infants. Prompt and adequate laser photocoagulation with a large number of high-intensity closely performed spots and early retreatment could be effective and safe for preventing the progression of APROP with plus disease in zone 1 or 2 in premature triplets.
Footnotes
Declaration of conflicting interests
None declared.
Funding
This research was supported by grants from the International Science and Technology Cooperation Program of Jilin Province (No. 20110733), the National Natural Science Foundation of China (No. 81400403) and the Technology Program of Soochow City (No. SYS201375).