
Abstract
A management algorithm for large renal cyst in autosomal dominant polycystic kidney disease (ADPKD) is lacking despite the potential to cause widespread medical and surgical complications. We report the case of a 37-year-old gentleman with ADPKD and large (>5 cm diameter) cysts who suffered sudden death due to autopsy-proven inferior vena cava and pulmonary arterial thrombosis. In this article, we discuss the possible pathophysiological factors at play in this catostrophic complication of ADPKD. We also review available literature to establish the prevalence of such a complication and also establish current thoughts and opinions as to the optimal management strategy for giant cysts in the context of ADPKD.
Introduction
Autosomal dominant polycystic kidney disease (ADPKD) is a condition with a high genetic penetrance affecting 1/1000 people. It is a multisystem disorder encompassing multiple renal cysts leading to renal impairment approximately 50% of individuals by the age of 60 years. 1
Patients with ADPKD also often have multiple liver cysts (80% of cases); pancreatic (8%) and splenic cysts (1–2%), intracranial berry aneurysms (6–16%), arachnoid membrane abnormalities, aortic aneurysms, cardiac valvular abnormalities and hypertension. Complications of the renal and hepatic cystic portion of the disease include pain, bleeding, rupture, infection, hypertension and a mass effect with compression of adjacent organs. Although mortality from cerebrovascular and cardiovascular causes has reduced over the last 20 years, cyst-related complications remain stagnant with nearly 20% of patients developing a cyst-related episode.2,3
A 37-year-old otherwise well man with known ADPKD and associated chronic kidney disease was found unresponsive at home by relatives. Despite aggressive and prolonged attempts at cardiopulmonary resuscitation by the paramedic attendants, spontaneous circulation could not be restored and he was pronounced dead. Recent blood tests conducted at his local nephrology clinic revealed a stable glomerular filtration rate of 22 mL/min, normal liver function, bone profile and clotting screens. A full autopsy was performed and revealed extensive inferior cava thrombus with extrinsic compression caused by a right renal cyst – approximately 5 cm in diameter and concomitant thrombus in the main pulmonary arterial trunk (Figure 1). There were no signs of iliofemoral vessels disease or signs of lower limb oedema which may have suggestive of deep venous thrombosis. The postulated mechanism of death was IVC compression due to a large right renal cyst leading to venous stasis, acute IVC thrombosis, pulmonary embolization and cardiovascular collapse.
Composite of Polycystic Kidney and Lung with Pulmonary Embolus.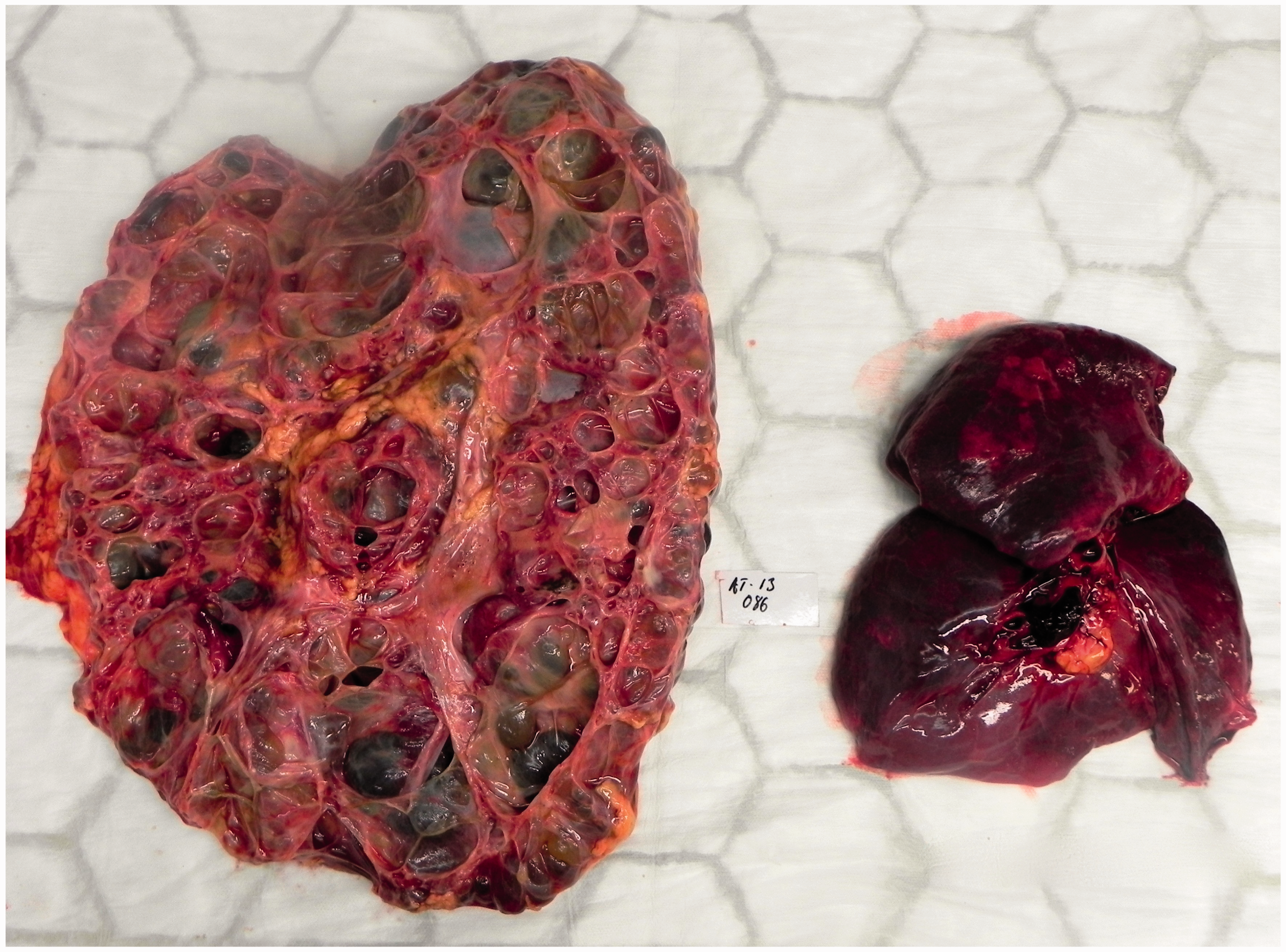
The patient was a young ambulant man of normal weight and blood pressure with no risk factors for thromboembolic disease such as smoking, recent long haul travel, previous history of deep venous disease, cardiac problems, malignancy or known thrombophilias. He had a family history only of polycystic kidney disease with no history of cardiac problems or thromboembolic events.
It is therefore likely that this patient succumbed to an extremely rare, indirect but noteworthy complication of his polycystic kidney disease.
Discussion
Similar manifestations of ADPKD are rare with only 11 cases reported worldwide. In nine out of these 11 cases, the aetiology of IVC thrombosis was a liver cyst impeding hepatic venous outflow due to either direct mass effect or acute rupture. Episodes of renal cystic lesion compressing the IVC and leading to pulmonary embolism have only been reported twice previously in published literature. 4 In both of these cases, the patients presented with symptoms of venous obstruction (lower extremity swelling) affording the opportunity of investigation with CT and the prompt initiation of treatment. In our case, there were no prodromal signs/symptoms which would have led to a suspicion of IVC obstruction or thrombus formation.
This case highlights an as yet unaddressed clinical conundrum: how often to image and when/if surgical intervention may be beneficial in large apparently asymptomatic renal cysts. Current literature is entirely focused on the management of symptomatic cysts (for pain, infection, bleeding and rupture).5,6 However, the wide variety of surgical management options available – ranging from aspiration, renal denervation, decortication and nephrectomy – can now be successfully undertaken laparoscopically. These new minimally invasive approaches with their resultant reduction in operative morbidity may allow for silent and asymptomatic cysts to be considered worthy operative candidates. Our case highlights that clinically silent medium and large-sized asymptomatic cysts also represent a clear and present danger. Any future studies directed to investigate the role of operative management of renal cysts must include this cohort in its protocol and analyses.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.