
Abstract
Introduction
Visceral artery aneurysms are very rare. Patients usually present as emergency secondary to the sudden rupture of the aneurysm or as an incidental finding on ultrasound, MRI or abdominal computed tomography. Among these, splenic artery aneurysms are the most common ones accounting for 60% of all splanchnic aneurysms and gastric and gastroepiploic aneurysms account for only about 4%.
Case presentation
We present a 61-year-old Caucasian male previously fit and well, presenting with sudden onset epigastric pain due to retroperitoneal haemorrhage secondary to ruptured left gastric artery aneurysm. Apart from a tender epigastrium, there were no other obvious signs elicited on abdominal examination. He had persistent tachycardia and haemoglobin drop from 10 g/dl to 6.7 g/dl. He underwent a contrast computed tomography which identified the ruptured left gastric artery. The aneurysm was controlled successfully with coil embolisation of the left gastric artery. At three-month follow–up, there was no evidence of the aneurysm.
Conclusion
Clinical presentations that do not correlate with examination finding should prompt immediate extensive investigation. The aid of contrast computed tomography and minimally invasive radiological interventional is the key to a fruitful outcome for this very rare entity.
Introduction
Visceral artery aneurysms are very rare. Patients usually present as emergency secondary to the sudden rupture of the aneurysm or as an incidental finding on ultrasound, MRI or abdominal computerised tomography (CT). 1 Among these, splenic artery aneurysms are the most common ones accounting for 60% of all splanchnic aneurysms 2 and gastric and gastroepiploic aneurysms account for only about 4%.2–6
In this article, we present a case of a patient with acute abdominal pain due to retroperitoneal haemorrhage secondary to ruptured left gastric artery aneurysm. The aneurysm was controlled successfully with coil embolisation of the left gastric artery.
Case report
A 61-year-old gentleman presented as an emergency admission to the accident and emergency department with sudden onset of epigastric pain radiating to the back. He was previously fit and well with no history of high blood pressure or any other medical illnesses. On examination, he was tender over the epigastrium but there was no evidence of generalised peritonitis. He had a normal biochemical and haematological investigation. His Hb level was 10 g/dL and amylase was normal. An erect chest X-ray did not show any evidence of pneumoperitoneum. He had persistent tachycardia and a repeat blood test after 12 h of his admission showed a drop of Hb to 6.7 g/dl.
An urgent CT was performed. This showed a massive retroperitoneal haematoma in the lesser sac with ongoing bleed from the left gastric artery (Figure 1).
CT transverse and sagittal of bleeding into lesser sac: red indicating site of haematoma in lesser sac.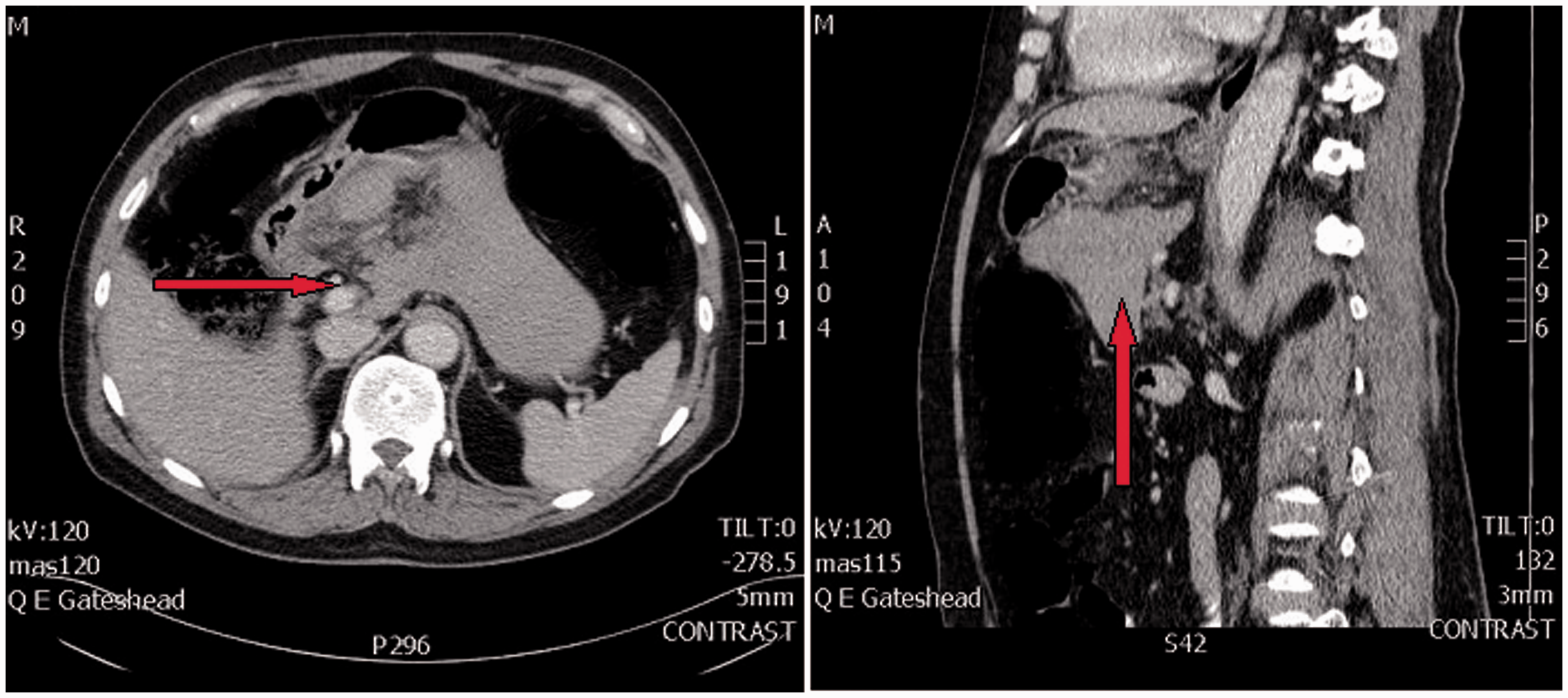
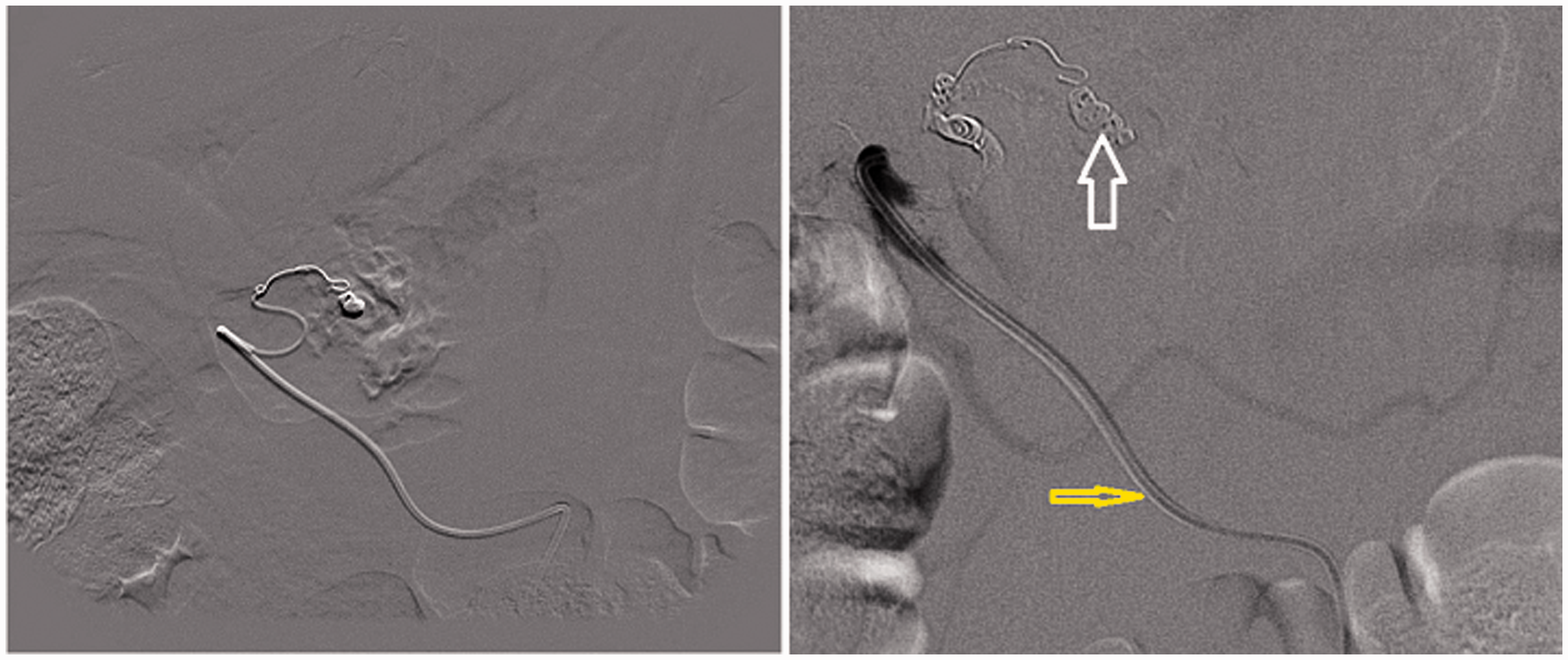
A mesenteric angiogram was then performed to identify the site of bleeding and to embolise the vessel if possible (Figure 2). This showed an actively bleeding left gastric artery aneurysm. The left gastric artery was then selectively catheterised and embolised with coils that were inserted to the afferent feeding vessel (Figure 3). The angiogram did confirm a good control of the aneurysm. He made a good recovery and was discharged home a few days later.
Mesenteric angiogram with contrast: active bleeding from the ruptured aneurysm (right). Yellow arrow: angiogram catheter. White arrow: aneurysm of left gastric artery. Mesenteric angiogram: leak from the artery (right), coil embolisation of the left gastric artery aneurysm (left).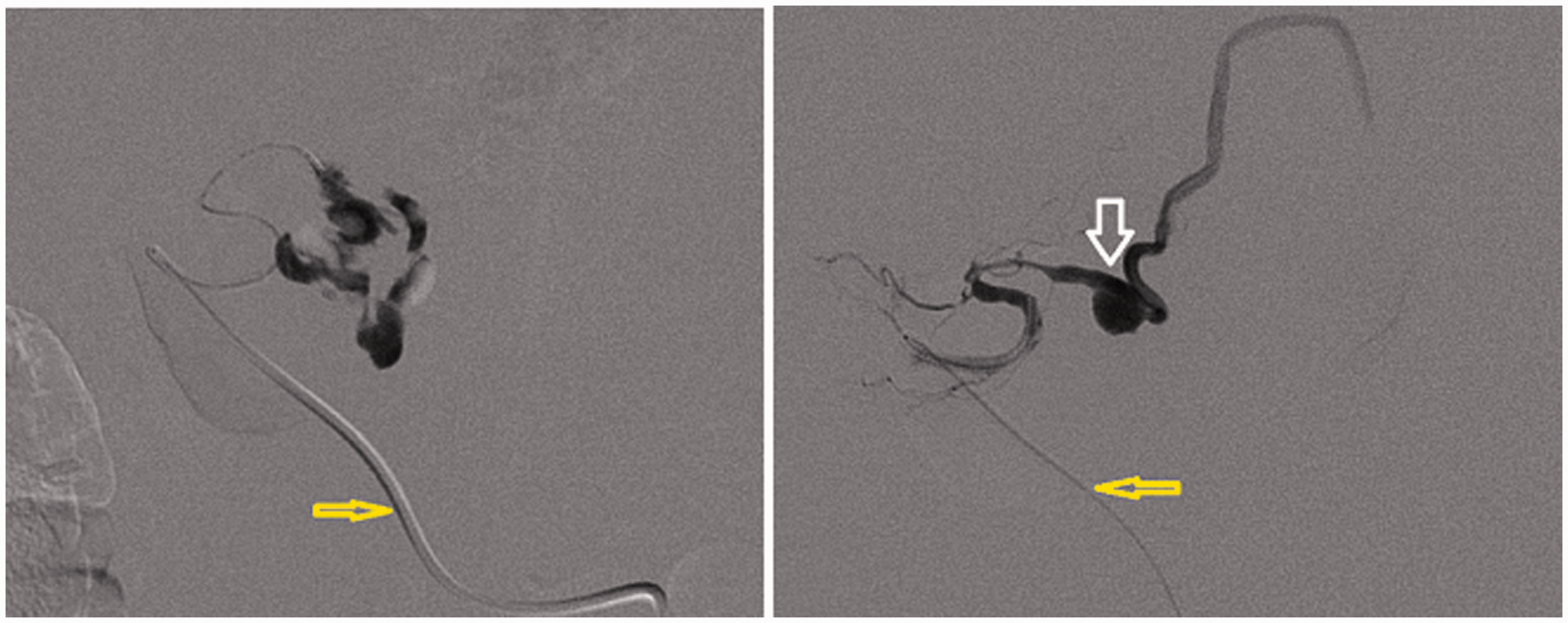
He was reviewed in the clinic three months later and a repeat CT scan was organised. This suggested dramatic resolution of the lesser sac haematoma with no evidence of aneurysm of the left gastric artery.
Discussion
Visceral artery aneurysms, including gastric artery lesions, are potentially lethal vascular pathologies that may be either congenital or acquired. 7 The acquired causes are inflammatory processes such as acute pancreatitis, peptic ulcer disease or vasculitis.1,7,8 Other acquired causes reported include, arteriosclerosis, trauma and connective tissue disorders.7,9,10 Although gastric artery aneurysms account for a very small percentage of visceral aneurysms encountered, a prompt diagnosis of this condition is important as nearly 80% of the patients reported with this condition can die 11 due to torrential haemorrhage. Gastric artery aneurysms are three times more common in men above the age of 50. 12 When the left gastric artery ruptures, it initially causes bleeding in the lesser sac 13 and may show a delayed overflow into the peritoneal cavity also called the ‘double rupture’ phenomena. 14
The true incidence of visceral artery aneurysm is unknown but it is being discovered more as an incidental finding due to the routine use of CT, MRI and angiography.1,14 However, many patients with visceral artery aneurysms still present as emergency due to rupture. 1
Selective angiography has become a standard method for treating these lesions and a multimodal approach 15 like deployment of coils, glue, thrombin, N-butyl cyanoacrylate or ethylene vinyl alcohol copolymer (Onyx) has been described in various studies.12,15,16 With advancements in interventional radiology, there is easier and safer access to small and remote vessels to treat difficult lesions. 17 Patients with a ruptured splanchnic artery aneurysm, including gastric artery aneurysm either needs surgical intervention or intervention radiology (IVR).11,18–20
Classic surgical options include ligation of the aneurysm or resection of the aneurysm with revascularisation.1,19,21,22 When patients present with a rupture, IVR is currently recommended as a first-line therapy.20,21 The risk of infarction to the organ is minimal when left gastric aneurysm is being treated due to the rich collateral supply by the surrounding vessels. 13
In summary, there should be a high level of clinical suspicion of a leaking visceral aneurysm in the differential diagnosis of epigastric pain with low haemoglobin. As reported in literature, the commonest clinical presentation of gastric artery aneurysm is epigastric pain and hypovolaemic shock. 12 A robust management of the problem by using minimally invasive method not only saves the patient a major open procedure but also his life.
Conclusion
Clinical presentations that do not correlate with examination finding should prompt immediate extensive investigation. The aid of contrast CT and minimally invasive radiological interventional is the key to a fruitful outcome for this very rare entity.
Footnotes
Acknowledgements
We would like to thank Dr Colin Nice for his expertise in interventional radiology and for providing the figures used in this article.
Authors' contributions
HK, RF and TF were involved in the progress of the patient’s care. HK and TF performed the literature search. CN, HK and TF were major contributors to writing the manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.