
Abstract

Introduction
Those of us who have practiced surgery for the last 40 years or so have witnessed a remarkable transformation of our profession. In the early years, we were highly respected, we had almost unequivocal authority, could choose at random our sub-speciality interest and had a substantial control over the amounts and means of our remuneration. Most surgeons loved their work and gave of their time willingly and generously. We had great professional satisfaction and much respect from the public.
Over the last three decades, much has changed; decision-making power has shifted from clinicians to management and administrators. Costs, not quality, are the dominant theme in medical practice. Surgeons now feel disenfranchised, frustrated and powerless. They feel they have lost control of their working conditions and more importantly have lost the public’s confidence. They now practice under a cloud of fear; fear from litigation, fear from managers and fear from the regulator. Not surprisingly, there is now much talk of the loss of professionalism. But what does this mean?
Professionalism constitutes a bridge between society and the profession and is based upon mutual benefit and mutual trust. If we are committed to re-establishing surgery as a profession in the 21st century, we need to understand what the origins of professionalism are, what the threats are, and why, in my view, there are grounds for optimism for the future.
Ethics and professionalism
Ethics and the concepts of professionalism are inextricably intertwined. 1 The core elements of a profession are the possession of a specialised body of knowledge and a commitment to service. The Oxford English Dictionary defines a profession as the occupation which one professes to be skilled in and to follow. The word professes represents a public commitment to a set of values for example, the Hippocratic Oath or its modern equivalent. The importance of the acquisition of knowledge and skills as are used to serve others is emphasised. Because knowledge is used in serving others, professions are identified as being altruistic and value laden. In medicine, it was the services of the healer whose roots can be traced to Hellenic Greece and the Hippocratic Oath, which were organised around the ideal of the professional. The traditional principles espoused by the Hippocratic tradition included reverence for teachers, consideration towards colleagues and the appeal to do no harm. So ethics and professionalism are inseparable and interdependent and, most importantly, emphasise the role of the doctor (or surgeon) as healer.
Threats to the professional
Threats to the Professional.
Trade unionism: professionalism vs. profession
Professionalism and profession are words with elastic meanings that should be separated from each other in debate. 2 A profession is any group with a special body of knowledge, standards of education and practice and an ethical framework based on a social contract that permits a high degree of self regulation. Ethical principles are important descriptors of a profession. The word profession means a declaration or promise or commitment which is publically stated. That promise is made in every clinical encounter when the doctor offers to help those in need with their specialised knowledge. That promise infers that competence, knowledge and skills will be used for patient advantage even if this means some degree of sacrifice on behalf of the doctor.
Professionalism, in contrast, denotes a self-protective, self-interest promoting guild spirit in an organisation protective of its privileges. This epitomises the trade union approach. Deprofessionalision of this corrupted form of profession is not necessarily always to be regretted. These differences are illustrated in Figure 1.
Profession versus professionalism. The implicit contract.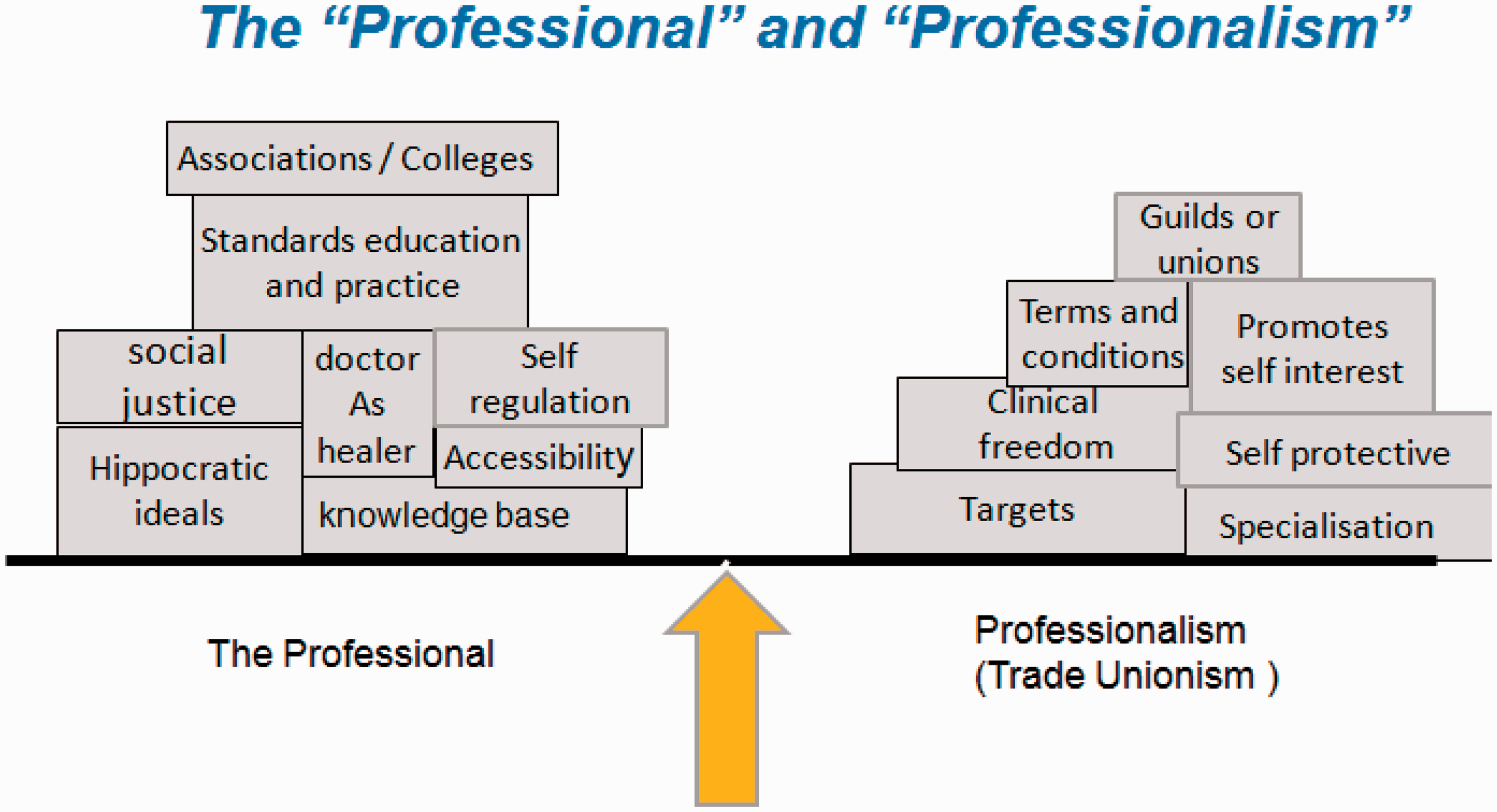

But doctors, surgeons, have to make a living and it would be unreasonable not to expect them to have some vested interest in their material reward for services provided. For doctors, who are usually employees, this serves to emphasise the inevitable conflict in their loyalties between the organisation which employs them, which seeks to make profit and the patient, to whom they owe a duty of care.
We cannot ignore the intrusion of costs into modern healthcare. This leads us directly to the next threat to our profession, the market place.
The market place
There is no doubt that recent years have seen a so-called ‘commodification’ of healthcare as a product like any other. As such, it is subject to the rules of the market place and the need to make profit. Concomitant with this has been a shift in professional values with greater emphasis on lifestyle and leisure activity. These changes were predicted over 30 years ago; many influential authors have predicted the pressures that would fall upon the profession of medicine as well as other professions. These have all increased greatly in the past three decades. Friedson, for example, was the first and most influential critic of contemporary medicines. 3 He stressed that medicine had used control over its knowledge base to gain a dominant position in society and within healthcare and had put its own welfare above that of society while failing spectacularly to self regulate. Others noted the closed nature of the profession and predicted that medicine would lose status through a process of de-professionalisation. 4 Many anticipated the market-driven changes that have occurred in recent years. In 1982, McKinley described the proletarianisation of American medicine, predicting that physicians would be reduced to selling their services in a competitive environment dominated by corporate interests playing physicians off against each other to diminish the unit price. 5 How apposite this is to the unseemly sight of surgeons competing for waiting list initiative work in private hospitals or soon, no doubt, in diagnostic and treatment centres. Other commentators have observed that medicine has sought to improve its position in society with little thought for the public good, gaining a monopoly over healthcare and then manipulating the market to create demand. The manipulation of waiting lists by a minority is a good example of this.
These factors all illustrate the self-serving power of a professional elite. Medicine, surgery in particular, is no longer trusted and as such loses significant influence. Alford described a concept of rationalisers who were found in state bureaucracies who seek to control the medical market place in the name of cost effectiveness. 6 These were to be distinguished from the monopolisers who are the medical associations and medical schools who seek to defend the status quo. There is no doubt who has been more successful in recent years. By the early 1990s, medicine as a profession was completely controlled by the state in countries such as ours or Canada, or by state and corporate interests in countries such as the USA. A consequence of this is that the public now perceive the problems of provision of healthcare as being the responsibility of the state and not necessarily of doctors. A further consequence is that society no longer holds the medical association in the high regard it used to do in the past. Krause in ‘Death of the Guild’ describes the medical profession’s loss of power to the state and draws analogy with many of the guilds of the 19th century which formally considered themselves powerful and immortal and which have now disappeared. 7 The Colleges and some Associations should take heed.
One unforeseen consequence of market forces in medical care has been erosion of the so-called ‘implicit contract’.
The implicit contract 8*
The ‘implicit contract’ describes a symbiotic relationship between the public (society), the medical profession and the State. 8 It has been described as a stable triangle of political forces based on mutual benefits. 9 Society was given healthcare rights by the state, and this healthcare was provided to a high standard by the medical profession. The state gained legitimacy and authority from society for providing healthcare, and relied on the medical profession to ration public resources. By providing high-quality care and applying resources appropriately, the medical profession gained the trust of citizens and the privileges of self regulation and professional autonomy within the NHS from the state.
In actuality, the implicit compact was the government granting the medical profession a large measure of autonomy and control over its work and its regulation. In return, doctors accepted the right of government to determine the budget and the broad national policy framework. As a consequence, doctors took decisions on the priority for treating patients within the available budget and politicians did not seek to influence these decisions. There was a degree of collusion between the government and the medical profession about not interfering in each other’s sphere of responsibility.
This is now all under threat as a consequence of high-profile cases in recent years, which have painted doctors and the profession in very poor light. These cases have led to a breakdown in trust between the profession, the society that it serves and the government.
This diminution in trust is exemplified by the exponential growth of agencies outside the NHS, all of which are government funded and all of which seek to make decisions on matters relating to healthcare and are often dominated by non-medical personnel. NICE, CQC, Monitor HQIP are all examples of such quangoes.
Evidence-based medicine
The old paradigm of medical training and learning was based primarily upon clinical experience. Implicit to this was the importance of apprenticeship and a deference to authority. Sadly, the system permits continuation of treatments based largely on faith and tradition. As Chantler said ‘medicine used to be simple, ineffective, and relatively safe. Now it is complex, effective, and potentially dangerous’. 10
One reason evidence-based medicine (EBM) evolved was as a consequence of perceived inadequacies in the old system. There was understandable distrust of the old meritocracy and discontent was fuelled by the ‘God of cost effectiveness’. Unfortunately, EBM has become a cult, almost a religion. It is led by managers, politicians and patient groups and not always by clinicians.
We have elevated the science published in journals and presented at meetings as being incontrovertible fact. Our search for certain proof has eroded valuable components of patient care such as comforting, explaining, listening, hand holding. These are all ‘passé’ in the EBM revolution. Note, importantly, that these are all attributes of the healer.
The proponents of EBM encourage the production of guidelines. Guidelines are loved by managers and politicians because they standardise healthcare, and this is considered cost effective. But guidelines have major drawbacks; these assume that the conclusions from clinical trials are always correct and we know that this simply is not the case. Further, guideline writers have a propensity to extrapolate unrepresentative trial data often carried out in specialist centres, to general populations or individual patients. Guidelines also encourage conformity. Sir Clifford Allbutt of Leeds said in 1906 that the prime condition of progress was to think the unthinkable. The greatest threat to progress is conformity. Guidelines might be cost effective but they guarantee conformity. As such, they necessarily stifle progress.
We presume we are better doctors or surgeons with the new science of EBM, but I am not so sure.
Increasing specialisation
I am not a ‘Luddite’ and as a specialist myself recognise the clear benefits of specialisation for a limited number of conditions. There is unequivocal proof that specialist care is associated with improved outcomes for a limited number of procedures. However, these axioms repeated ad nauseam at clinical meetings, supported by the medical press and regarded as untouchable by the guideline writers ignore the clinical reality of everyday practice. The great majority of clinical conditions, are by definition, because they are the majority, common. We need doctors, surgeons, to look after the majority not just the minority.
So, as recognised in the recent Greenaway report, we need generalists. 11 But from the perspective of professionalisation, we need to recognise the potential hazards of specialisation. The problem is that being a generalist is perceived as demeaning. Generalism has a low status, there is more money in specialising and modern society has come to venerate the specialist as a proxy for ‘better’.
Specialisation does have drawbacks; it breaks down continuity of care, promoting the ‘not in my clinical area’ response that fuels endless internal specialist referrals which waste time and resources. It means that health professionals are reticent to make decisions outside their specialty, which leads to a creeping paralysis of medical systems. Specialist opinion now dominates guideline development leading to the unblinkered extrapolation of unrepresentative trial data into general populations. Specialisation promotes medical tribalism in which clinicians aggressively defend their clinical turf and are unwilling to accept criticism. Specialisation encourages clinicians to work in selective silos rendering them less susceptible to outside influence. Specialisation encourages self-protectionism and elitism. Unchecked, it will lead to increased fragmentation of the medical profession.
Conversely, and paradoxically, were the sub-specialities in medicine and surgery to openly embrace the need for the generality of care, then their own long-term survival would be more probable.
Reasons for optimism
There are, in my view, three reasons to be optimistic: Firstly, despite the fact that medicine has lost control of the market place, and as such its ability to bargain has been greatly reduced, nonetheless few question the role of the medical profession in the setting and maintaining of standards. Colleges and Speciality Associations must take advantage of opportunities now presented to re-build trust by openly espousing a public service commitment. Secondly, because medicine as a profession no longer controls healthcare systems, it is perceived as being more objective when it offers commentary and advice. The role of the profession as a source of impartial expertise may then become re-established. Repeated surveys of public opinion demonstrate a continued Trust in doctors, despite the adverse publicity of recent years. This suggests that the public still look to the profession for advice. The third cause for optimism is society’s need for and dependence on the healer. As Cruess et al. described, the mystique of medicine has been retained through the role of the healer.
4
This is particularly true for surgery. The unique place of surgery within medicine as a profession was exemplified in an excellent article by JM Little entitled ‘Ethics in Surgical Practice’.
12
In this, he talks about the ethics of surgery and describes five factors that distinguish surgery from other aspects of medicine and which underpin the ethics of surgical practice. These are: rescue, proximity, ordeal, aftermath and presence. Rescue recognises that surgery is an assault on the person and thereby to consent to surgery intimates that the surgeon rescues the patient from their disease. Surgeons can abuse this by over-rating the benefits of surgery or not being honest about complications or mortality. Proximity recognises that the surgeon enters into a relationship with the patient which is unlike any other. By the end of the surgical encounter, the surgeon will know things about the patient’s body that are hidden from the patient. Proximity is an unbalanced privileged relationship which is easily abused if not acknowledged. Ordeal recognises that surgery is something to be endured. Surgeons should not forget that whilst they may enjoy their operations, the patients most certainly do not. Aftermath recognises that surgical procedures leave scars, stomas, stiffness, discomfort and recurrent symptoms that all serve as reminders of the past illness. As Little states, the burdens of survivorship may be lifelong. Finally, Presence, which in many ways is the most compelling of Little’s five principles. In this, it is recognised that what patients want most from their surgeons is their presence. Patients want their surgeon to demonstrate his or her commitment to a caring role by being there and being available to talk. Little’s principles provide a framework by which surgeons can establish and maintain trust, not only with individual patients, but also with wider society. In this context, I would add the principles of veracity and audit. Over the past few decades the relationship between surgeons and their patients has deteriorated for all the reasons outlined above. If surgeons as a profession take the opportunity to rebuild trust with their patients, then their future as a profession is guaranteed.
The future
Surgeons are, and will be, professionals. But this is not to ignore the overwhelming influence of the market economy on the day-to-day practice of each and every surgeon. While individual surgeons may feel that outside agencies have no right to influence their practice on the grounds of cost or the spurious argument of clinical independence, they would be entirely wrong. Surgeons have a moral and an ethical responsibility as professionals to advise on appropriate treatments taking into account cost effectiveness. The maverick surgeon promulgating the latest robotic or laparoscopic procedure is acting unethically, if these operations are unproven and performed to satisfy personal whims. Similarly, surgeons pursing the latest technological technique, be it laparoscopic or otherwise, for many hours for reasons of personal pride and edification is wholly immoral. We, as surgeons need to evaluate new techniques from all aspects including cost effectiveness to provide that impartial advice referred to above to the budget holders in our institutions. I think we have failed to do this satisfactorily in the recent past. If surgeons wish to continue to be held in high esteem, they need to avoid the accusation of self-interest.
Conclusion
So, as argued in preceding paragraphs, my view is that surgery as a profession does have a future primarily because surgeons occupy a unique role as healers, and this will endure. But their role as impartial advisers needs to be performed in the context of a modern society in which cost effectiveness is a primary driver. Surgeons must not shirk this responsibility; they must engage with this process.
And this leads to a most curious paradox: accepting that the modern surgeon is a healer, but nonetheless has an ethical responsibility to consider costs for the benefit of society, the question arises as to who should look to the interests of the surgeon. I have argued that the Colleges and Associations’ prime responsibility is to educate, maintain standards and offer impartial advice as their primary commitment is to the public. That being the case, it would be inappropriate for them to become involved with the terms and conditions of surgeons as they would rightly be accused of conflict of interest. Logically, therefore, there must be a place for an organisation to exist which represents the interests of surgeons outwith their professional responsibilities. Does this mean that surgeons need their own trade union?
Footnotes
Acknowledgements
1. This article is based upon the RCP and S Glasgow Macewen lecture delivered to Association Surgeons GB and Ireland, April 2015.
2. The image of the implicit contract is reproduced courtesy of ‘Hospital Medicine’.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.