MiR-27 a/b contributes to proinflammatory phenotype of monocytes in treatment-resistant rheumatoid arthritis patients
M Frleta1,2, DS Gilchrist1, A Rainey1, L Crawford1, D Baxter2, M Kurowska-Stolarska1 and IB McInnes1,2
1Institute of Infection, Immunity and Inflammation, University of Glasgow, UK
2Rheumatology Clinic, Glasgow Royal Infirmary, UK
Abstract
Aim/Background: Although newly available therapeutics revolutionised treatment of rheumatoid arthritis, we are still unable to predict poor response to conventional disease modifying drugs (cDMARDs) or biologics in our patients. Treatment stratification is essential to improve outcomes in rheumatoid arthritis patients. The aim of this study was to identify microRNA signatures in CD14+ monocytes predictive of resistance to conventional and anti-TNFα therapies. Identified miR-27 a/b is dramatically down-regulated in monocytes of patients, failing multiple modes of treatment.
Methods: Peripheral blood CD14+ monocytes were isolated from three groups of rheumatoid arthritis patients meeting ACR2010 criteria: good responders to cDMARD (n = 20), resistant to cDMARDs (n = 17) or anti-TNFα agents (n = 30). Age-matched healthy volunteers (n = 23) were collected as controls. miRNA expression was quantified by Taqman-Low-Density-Array. TargetScan was used to identify potential miR-27 a/b targets.
Results: Our data identified miR-27 a/b as being significantly reduced in difficult-to-treat patients. Furthermore, these patients had elevated levels of both serum IL-6 (p < 0.001), and STAT3 when compared to patients with low disease activity following treatment with cDMARDs (p < 0.05) or healthy controls (p = 0.05). In silico analysis identified the IL-6 pathway as containing several potential miR-27 targets, including both soluble and membrane-bound isoforms of IL-6 receptor. Both IL-6 receptor variants were confirmed as targets of miR-27 a/b by luciferase assay. Inhibition of endogenous miR-27 a/b in THP-1 cells significantly increased levels of Il-6 R (p = 0.05, n = 4), showing that miR-27 a/b actively regulate IL-6 receptor expression in these cells.
Conclusion: Our study provides a novel molecular insight into the state of peripheral blood monocytes in difficult-to-treat patients, identifying potential new biomarkers in disease chronicity.
The association between capillary blood glucose and mortality: time to rethink inpatient glycaemic targets?
GC Jones, CAR Sainsbury and JG Timmons*
Centre for Diabetes, Gartnavel General Hospital, Glasgow, UK
*Academic FY1 Western Infirmary
Abstract
Background: Diabetes affects 7% of the population and 20% of hospital inpatients. Mortality and length of hospital stay are increased in this group – associated with hypo and hyperglycaemia.
Methods: Capillary blood glucose data from eight acute hospitals and associated units within NHS Greater Glasgow and Clyde between 1 January 2011 and 22 April 2013 were included. Patients were stratified into two groups. Follow-up analysis over 2.4 years was performed.
Results: 1,774,580 capillary blood glucose results were collected from 39,487 individuals. There were 15,989 in the diabetic subset and 16,108 without dysglycaemia. 5866 deaths were recorded over 2.4 years. In the total dataset, hyperglycaemia (capillary blood glucose >11.1 mmol/l) and severe hyperglycaemia (capillary blood glucose >20 mmol/l) had mortality hazard ratios of 1.13 and 1.47, respectively. In the diabetes subset, hyperglycaemia and severe hyperglycaemia had mortality hazard ratios 0.93 and 1.31, respectively. In the non-dysglycaemic dataset hyperglycaemia hazard ratio was 1.18. In the total dataset, severe hypoglycaemia (capillary blood glucose <2.5 mmol/l) and hypoglycaemia (<4 mmol/l) were associated with mortality hazard ratios of 1.56 and 1.28. In diabetic subjects, hazard ratios were 1.63 and 1.47 for severe hypoglycaemia and hypoglycaemia. Mortality was particularly high <90 days after measurement – hazard ratio 2.24 for both severe hypoglycaemia and hypoglycaemia. In no dysglycaemia subset, mortality hazard ratio was 0.87 with preponderance for early mortality <90 days (hazard ratio 1.27). Severe hypoglycaemia showed no significant difference over the total follow-up.
Conclusion: The findings support previous studies which have demonstrated excess mortality associated with hypoglycaemia. Mortality associated with hypoglycaemia – particularly early mortality – should be considered when setting inpatient glycaemic targets.
Obstetric and long-term kidney outcomes in renal transplant recipients: a 40-year single-centre study
S Stoumpos1, SH McNeill1, M Gorrie1, PB Mark1, JE Brennand2, CC Geddes1 and CJ Deighan1
1Glasgow Renal and Transplant Unit, Western Infirmary, Glasgow, UK
2Maternity Unit, Southern General Hospital, Glasgow UK
Abstract
Background: Fertility rapidly returns to women after successful kidney transplantation. The aim of this study was to analyse obstetric and kidney outcomes among all renal transplant recipients in our centre who have had a pregnancy.
Methods: Pregnant women with a kidney transplant were identified through our prospectively maintained electronic patient record and case notes between 1 January 1973 and 28 February 2013. A nested case–control study was also performed by identifying 83 pairs of pregnant and non-pregnant controls matched for sex, age, transplant vintage and creatinine.
Results: There were 138 pregnancies reported from 89 renal transplant recipients. Mean ages at the time of transplantation and pregnancy were 25.2 ± 6.4 and 30.3 ± 5.1 years, respectively. Median duration of follow-up from the first pregnancy was 8.2 years (IQR: 3.8, 16.9). There were live births in 74% of pregnancies with high prevalence of prematurity (61%), preeclampsia (14%) and low birth weight (52%). Lower eGFR (OR 0.98; p = 0.05) and higher uPCR (OR 1.86; p = 0.02) at conception were independent predictors for poor pregnancy outcome. Lower eGFR (OR 0.98; p = 0.04), higher uPCR (OR 1.50; p = 0.04) and living donor transplant (OR 0.35; p = 0.02) were the only significant predictors of ≥20% loss of eGFR one year after delivery. A first pregnancy was not associated with a poorer 10 years transplant or 20 years patient survival in kidney transplant recipients.
Conclusions: This analysis provides reassuring information about the long-term effects of pregnancy on kidney transplant function. In addition, it confirms previous information about the relatively high rates of obstetric complications in renal transplant recipients.
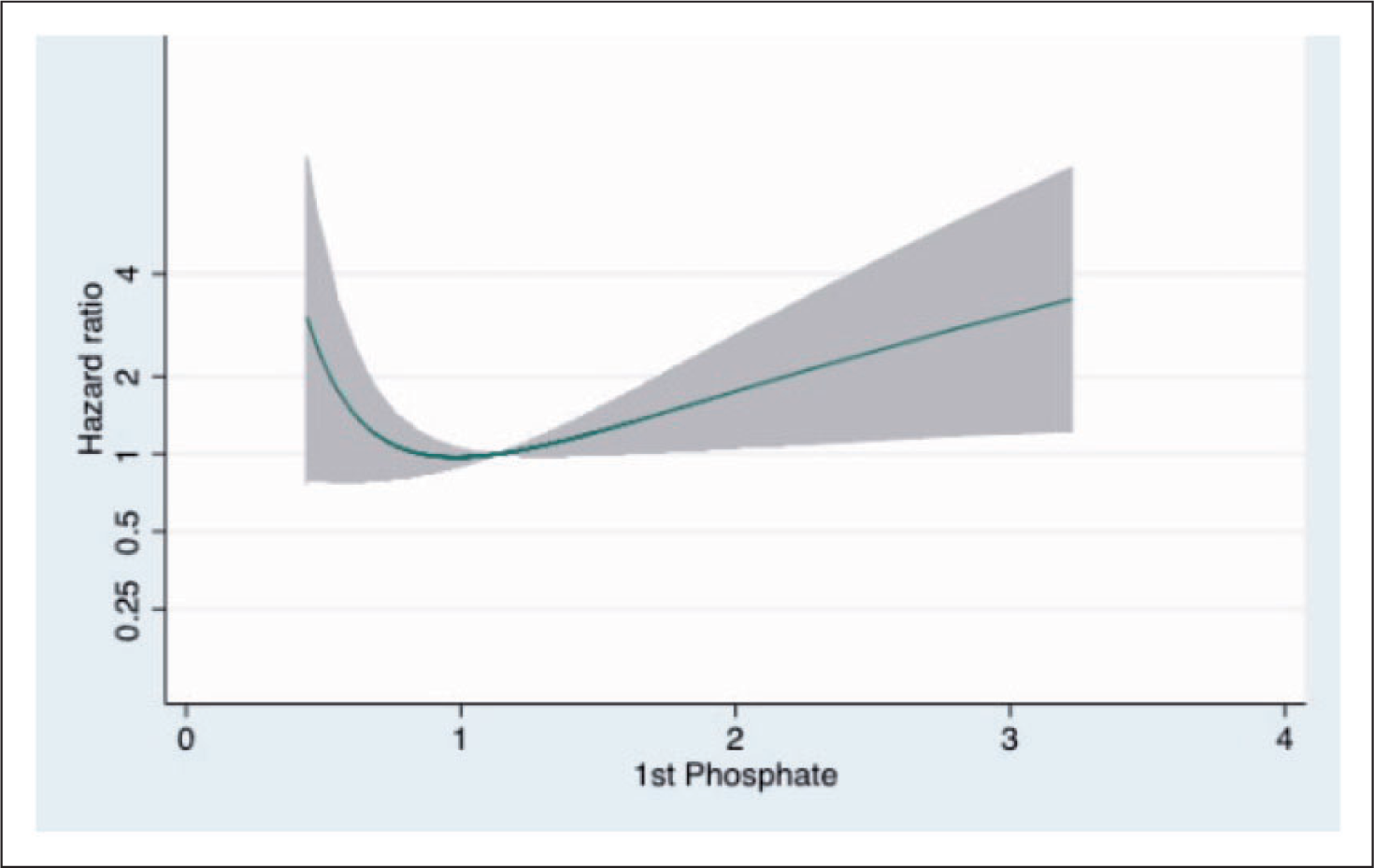
‘J shaped’ relationship between phosphate and risk of death in non-dialysis chronic kidney disease patients
S Macpherson1, PC Thomson2, MD Solbu1, KK Stevens1,2, AG Jardine1,2, RK Patel1,2 and PB Mark1,2
1University of Glasgow, Institute of Cardiovascular and Medical Sciences, UK
2Western Infirmary, Renal and Transplant Unit, UK
Abstract
Background: Hyperphosphataemia is associated with reduced survival in renal disease. We studied the relationship between serum phosphate, socioeconomic deprivation and long-term outcome in non-dialysis chronic kidney disease.
Methods: Adult patients with a first renal clinic attendance (excluding dialysis and transplant) during 2010–13 were studied. Baseline clinical and laboratory data at presentation were retrieved. Follow-up was recorded to October 2014. Time to death was calculated and stepwise Cox regression used to identify covariates significantly associated with survival.
Results: During the study period 2989 patients had a first clinic attendance. The mean estimated GFR (eGFR) at baseline was 46 ml/min. During follow-up 386 (12.9%) patients died. There were 67 cardiovascular deaths, 26.0% of known causes of death. Patients who died were older (74.8 versus 62.6 years, p < 0.001), had higher serum phosphate (1.20 versus 1.12 mmol/l, p < 0.001), lower haemoglobin (111 versus 125 g/l, p < 0.001) and eGFR (33 versus 48 ml/min, p < 0.001) than those alive at the end of follow-up. Patients who resided in lower socioeconomic areas had higher serum phosphate despite similar eGFR (47.0 versus 48 ml/min, p = 0.5). In a multivariate model significant independent predictors of mortality were age, male gender, increased serum phosphate, eGFR, haemoglobin and lower socioeconomic status. Increased phosphate was a significant independent predictor of cardiovascular death.
Conclusions: Increased serum phosphate and low socioeconomic status are independent risk factors for mortality in chronic kidney disease patients. Elevated phosphate despite similar renal function suggests high dietary phosphate might explain hyperphosphataemia in lower socioeconomic groups. Very low phosphate is also associated with increased risk.
Thromboembolism in primary nephrotic syndrome: is the risk overstated?
AJ Rankin, EP McQuarrie, JG Fox, CC Geddes and, B Mackinnon and On behalf of the Scottish Renal Biopsy Registry
Glasgow Renal and Transplant Unit, Western Infirmary, Glasgow, UK
Abstract
Background: Venous thromboembolism has been reported to occur in 25–30% of adult patients with nephrotic syndrome. As a result, empirical anticoagulation has been advocated in certain situations. We aimed to assess the incidence of venous thromboembolism in our patient population.
Hazard ratio of death in non-dialysis chronic kidney disease patients adjusted for eGFR, age and systolic blood pressure.
Methods: All adult patients undergoing native renal biopsy for nephrotic syndrome between 2009 and 2012 in the Glasgow Renal and Transplant Unit were identified. Using the prospectively completed electronic patient record the incidence of venous thromboembolism at any site was determined.
Results: Two-hundred and one patients underwent first renal biopsy for nephrotic syndrome during the four year period. Sixty-three were excluded for non-primary causes, leaving 138 for analysis. Median follow-up was 2.8 years. Fifteen (10.5%) patients suffered venous thromboembolism. Mean age was 58 years and 55% were male. The site of venous thromboembolism was pulmonary (n = 5), leg deep vein (n = 3), renal vein (n = 2) and other (n = 5). Median time to diagnosis of venous thromboembolism from renal biopsy was 24 days (IQR -22 to 195). Mean serum albumin at time of clot was 23 g/l (SD 11), median uPCR 714 mmol/mol and mean eGFR 69 ml/min/1.73 m2 (SD 51). There was no significant difference in the mean age (p = 0.2), serum albumin at diagnosis (p = 0.2) or median uPCR (p = 0.9) between those who suffered a venous thromboembolism and those who did not.
Conclusions: In this cohort, the incidence of venous thromboembolism at 10% is lower than quoted in the literature. The risk appears highest early in the course of nephrotic syndrome. These data suggest that routine anticoagulation of nephrotic patients may not be justified.
Collapses on both sides of the Clyde
A Shepherd1, K Colquhoun2 and L Mitchell2
1Department of Geriatric Medicine, Gartnavel General Hospital, Glasgow (GGH), UK
2Department of Geriatric Medicine, Southern General Hospital, Glasgow (SGH), UK
Abstract
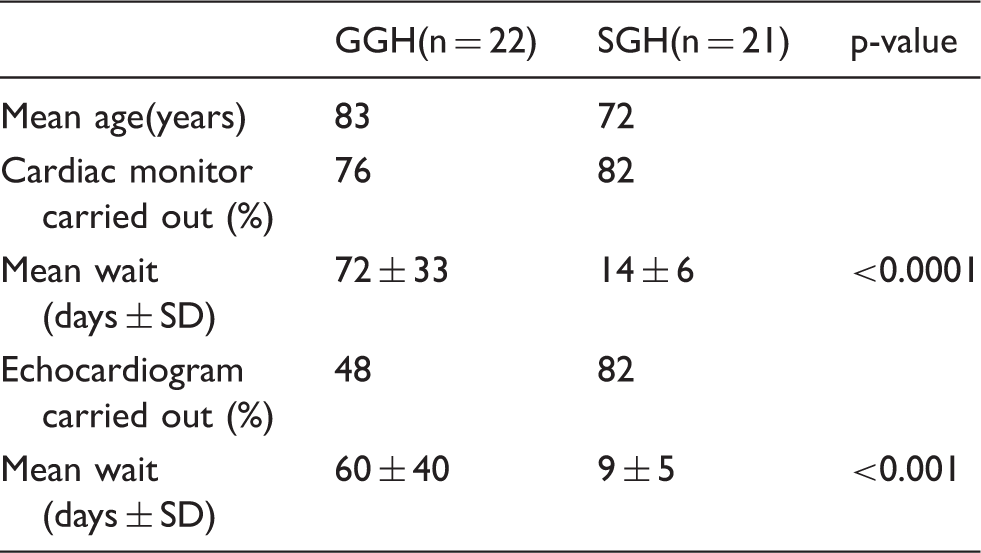
Aim: Rapid access syncope clinics improve both diagnostic efficiency and effectiveness (RA Kenny, D O’Shea, Age and Aging 2002;31:272–5). A dedicated syncope outpatient service was funded in SGH in 2005, no equivalent service exists in north Glasgow.
Method: From September to November 2013, new referrals to both falls and general clinics at GGH were screened, those describing syncope included. These were compared with all new referrals to the SGH syncope service over the same time period. All patients were analysed using the SGH syncope pro forma.
Results:
Abstract
SGH patients underwent more cardiac investigations, and all monitors were 3–7 days, compared with one day for GGH patients. Final diagnosis was documented for 90% of SGH patients compared with 57% of GGH patients. Resolution of symptoms was documented for 82% of SGH patients, 18% reporting partial improvement. Symptom resolution was documented in 19% of the GGH group, partial improvement in 51%.
GGH(n = 22)
SGH(n = 21)
p-value
Mean age(years)
83
72
Cardiac monitor carried out (%)
76
82
Mean wait (days ± SD)
72 ± 33
14 ± 6
<0.0001
Echocardiogram carried out (%)
48
82
Mean wait (days ± SD)
60 ± 40
9 ± 5
<0.001
Conclusion: These data indicate that the dedicated syncope clinic delivers faster investigations and, therefore, more timely diagnoses, to patients in south Glasgow versus those in the north. We would like to roll this service out in GGH.
Can measuring radio density predict urinary calculi composition?
J Hendry and GE Jones
Department of Urology, Glasgow Royal Infirmary, Glasgow, UK
Abstract
Background: Non-contrast computed tomography is the gold standard in investigating urinary calculi. Accurate radio density measurements with Hounsfield units may allow treatment planning of calculi prior to knowing biochemical analysis of stone composition.
Methods: A retrospective analysis of urinary calculi density on non-contrast computed tomography with three different graphics tools (square, circle and arrow) to calculate Hounsefield unit values in all patients undergoing percutaneous nephrolithomy between 2012 and 2014 was performed. Hounsefield unit density (Hounsefield unit/length in mm) was compared as higher radio density is linked with larger stone size. Statistical analysis of calculi density against stone composition was undertaken with one-way ANOVA and Student’s t-testing (significance p < 0.05).
Results: One hundred and one patients were included with mixed composition in 49 (48%). Calculi composition was: 33 calcium phosphate, 47 calcium oxalate, 11 struvite and 10 uric acid stones. Hounsefield unit density across three methods of measuring varied significantly for arrow versus square and circle measures (p < 0.01). Uric acid and struvite stones had significantly lower Hounsefield unit density versus all calcium stones (p < 0.01). No uric acid or struvite stone had a density higher than 50 HU/mm.
Conclusions: Radio density varies as per stone composition and a density of <50 HU/mm can predict composition of stones containing uric acid or struvite. The arrow graphics tool may not be the most accurate to predict. Hounsfield density of renal calculi and the alternative tools for estimating density should be used.
Patterns and impact of hypoglycaemia and hyperglycaemia on inpatients with cystic fibrosis-related diabetes treated with insulin
ZM Chong, J Gilmour, CAR Sainsbury and GC Jones
Diabetes Department, Gartnavel General Hospital, Scotland, UK
Abstract
Background: Patients with cystic fibrosis-related diabetes have a higher mortality than cystic fibrosis patients without diabetes. Hypoglycaemia, hyperglycaemia and glucose variability confer excess mortality and morbidity in the general population with diabetes. We investigated patterns of hypoglycaemia/hyperglycaemia and their association with mortality and readmission rate in inpatients with cystic fibrosis-related diabetes.
Methods: We identified all capillary blood glucose readings (measured using Abbott Precision Web system) of 105 patients with cystic fibrosis-related diabetes measured within our health board between January 2009 and September 2013. Frequency and timing of hypoglycaemia (<4 mmol/l) and hyperglycaemia (>15 mmol/l) were recorded and capillary blood glucose interquartile range calculated. Readmission rate at one year was compared with Chi square test. Survival analysis was performed using Cox proportional hazard model.
Results: 18,252 capillary blood glucose results were included. Hypoglycaemia was common with 1153 episodes (6.3%). Hypoglycaemia rate was constant throughout the day. Hypoglycaemia was associated with significant higher readmission rate at one year (64% versus 88%, p = 0.047). Hypoglycaemia, hyperglycaemia and high interquartile range were associated with non-significant increases in mortality.
Conclusions: Among inpatients with cystic fibrosis-related diabetes hypoglycaemia is common and predicts increased rate of readmission. Unlike previously reported trends in general inpatient population this group does not show a peak incidence of hypoglycaemic during night. Timings of capillary blood glucose monitoring should reflect this pattern. Impact on readmission rate of hypoglycaemia and trends to increased mortality with hypoglycaemia, hyperglycaemia and high interquartile range were found and avoidance of these patterns may be beneficial.
The use of dapagliflozin and its efficacy in Greater Glasgow and Clyde
Feicong Huang, CAR Sainsbury and GC Jones
Gartnavel General Hospital, Glasgow, UK
Abstract
Background: Trial data for dapagliflozin has shown reduction of HbA1c, weight and BP in patients with type 2 diabetes. Previous studies were performed in highly selected patient groups and may not reflect ‘real-world’ eclinical practice.
Methods: We report clinical experience with patients with type 2 diabetes taking dapagliflozin since authorisation within our healthcare system in January 2013. Data were collected retrospectively from primary and secondary care diabetes database.
Results: Four hundred and twenty-seven patients with type 2 diabetes had dapagliflozin initiated as part of routine care. Forty-three patients with no follow-up data were excluded. Of 384 remaining patients (208 male, mean age 57.4 years) baseline median HbA1c was 81 mmol/mol and weight was 97.4 kg (BMI 33.4). Dapagliflozin was used as monotherapy in one patient, as add on to one or more non-insulin therapies in 283 patients and with insulin ± other agents in 100 patients. In particular, 59 patients were on GLP-1. Ten patients had eGFR<60 at the time of therapy initiation. Fourteen (3.6%) patients stopped taking dapagliflozin during follow-up. Data were analysed by intention to treat. Hba1c was significantly reduced at 3 (−6 mmol/l), 6 (−12 mmol/l), 12 (−15 mmol/l) and 24 (−16.5 mmol/l) months (p < 0.05). Median weight loss at 12 months was 4.65 kg. There was a significant median reduction in systolic BP of 4 mmHg.
Conclusions: In our clinical practice dapagliflozin is effective at reducing HbA1c at up to two years. Weight reduction was recorded in 80% of those with data recorded. Withdrawal from treatment was low. This is in keeping with published trial data.
Initial experience with volume assured pressure support mode nocturnal NIV in a tertiary breathing support service
C Williams, G McDowell, D Macfarlane, H Ambler, S Davidson and C Carlin
Department of Respiratory Medicine, Gartnavel General Hospital, NHS Greater Glasgow & Clyde, Glasgow, UK
Abstract
Background: Long-term nocturnal non-invasive ventilation improves clinical outcomes in a range of disorders. Novel sensing, auto-titrating and responsive capabilities of the latest non-invasive ventilation modes (e.g. ‘AVAPS-AE’) may have clinical utility for initial non-invasive ventilation titration, long-term therapy in patients with labile ventilatory status and rescue therapy in patients responding sub-optimally to standard fixed pressure non-invasive ventilation. Clinical trial and real-world experience is currently limited.
Methods: Twenty-nine patients (obesity hypoventilation n = 19, kyphoscoliosis n = 6, airways disease n = 1, respiratory muscle weakness n = 2, cystic fibrosis n = 1) had received AVAPS-AE mode non-invasive ventilation via Respironics A40 generator based on clinical judgement and device availability. Their clinical and sleep study data, capillary blood gases and ventilation parameters were reviewed.
Results: Nineteen patients had AVAPS-AE for titration and were transitioned onto conventional non-invasive ventilation using the derived ventilator settings, which were unexpected in a significant minority. Mask leak compromised AVAPS-AE titration in a minority, but reduced length of hospital stay versus standard management was evident. Seven patients with complex obesity-related cardiorespiratory failure continued with AVAPS-AE as destination therapy, based on suboptimal response and/or poorer tolerance of conventional non-invasive ventilation. Three patients with acute respiratory acidosis refractory to conventional non-invasive ventilation responded to AVAPS-AE mode rescue therapy.
Conclusions: Adaptive, volume assured pressure support mode non-invasive ventilation appears as a valuable adjunct. Higher cost versus standard generators may be offset by service efficiency gains. Use of adaptive non-invasive ventilation for titration, troubleshooting and destination therapy in patients with nocturnal hypoventilation merits further scrutiny.
Predictors of therapy discontinuation in stroke secondary prevention
Sukainah Al AlShaikh1, Jesse Dawson1, Rachael Fulton1, Matthew Walters1, Philip Bath2 and Ashfaq Shuaib3
1Institute of Cardiovascular & Medical Sciences, University of Glasgow, Glasgow UK
2The University of Nottingham, UK
3University of Alberta, USA
For the VISTA Collaborators
Abstract
Introduction: Secondary preventative strategies are prescribed to reduce recurrence following ischaemic stroke. We investigated factors that may predict discontinuation of preventative strategies after stroke.
Methods: We used data from the Virtual International Stroke Trials Archive. We included patients with ischaemic stroke who were prescribed secondary preventative medication. We measured rate of discontinuation of major drug classes and used regression analysis to identify independent predictors of discontinuation of at least one drug class.
Results: A total of 10,304 patients were included. The mean age of participants was 69.4 (SD 12.4) years. When prescribed, percentage discontinuation was 12% for anti-coagulants, 18.7% for anti-platelets, 13.3% for lipid-modifying agents and 22% for anti-hypertensive medications. Older age (OR 0.98; 95% CI 0.97–0.99 per year), non-white ethnicity (OR 0.75; 95% CI 0.59–0.96; p = 0.02), higher baseline NIHSS score (OR 0.93; 95% CI 0.91–0.94 per unit increase), smoking (OR 0.87; 95% CI 0.78–0.97), polypharmacy (OR, 1.02; 95% CI 1.00–1.03, per drug) previous treatment with anti-coagulants (OR 0.46; 95% CI 0.35–0.61) or anti-platelets (OR 0.71; 95% CI 0.59–0.86) and cortical involvement (OR 0.70; 95% CI 0.52–0.94) were significant predictors of discontinuation. A regression model including these variables accounted for only a fraction of variance in treatment continuation (R-squared 0.07).
Discussion: Discontinuation of preventative medications after stroke is common. Although we identified several factors associated with stopping treatment, these were poorly predictive and further work is needed to better identify patients at risk of not being on preventative measures.
Is small beautiful? Emergency laparotomy outcomes in Scottish rural versus non-rural hospitals: a 10-year retrospective national cohort study
SJ Fergusson1, S Paterson-Brown2 and EM Harrison2
1Wishaw General Hospital, Lanarkshire, UK
2Royal Infirmary of Edinburgh, Little France Crescent, Edinburgh, UK
Abstract
Background: Post-operative mortality following emergency laparotomy is approximately 15% in the UK but the hospital-level characteristics which affect outcome have not yet been clearly determined. This study explores the effect of hospital rurality by comparing mortality and readmission rate following emergency laparotomy between Scotland’s six remote and rural hospitals and all other Scottish non-rural hospitals providing a comprehensive surgical service.
Methods: Data on all emergency laparotomies performed in Scotland from April 2001 to March 2011 were identified from the SMR01 national inpatient database. Risk-adjusted odds ratios of 30-day mortality and readmission (for any indication) were calculated using a model which included age, deprivation, a co-morbidity index and a procedural risk variable.
Results: A cohort of 30,623 cases was identified, with median age 65 years old. Overall Scottish all-cause post-operative mortality was 11.3% at 30 days. Thirty-day mortality in the 835 rural hospital cases was 9.2% versus 11.4% in the 29,726 non-rural hospital cases, p = 0.052. The risk-adjusted odds ratio of 30-day mortality in rural centres was 0.62 compared to non-rural centres (95% confidence interval (CI) 0.48–0.79). Thirty-day readmission rate in rural cases was 8.3%, compared with 12.4% in non-rural cases (p = 0.001). The risk-adjusted odds ratio of rural hospital readmission was 0.66 (95% CI 0.51–0.84).
Conclusions: Risk-adjusted Scottish administrative data demonstrate that emergency laparotomy outcomes are superior in rural hospitals, compared to non-rural. This suggests that rural hospitals are providing a high quality of emergency surgical care, even accepting that their case mix and transfer patterns are different to non-rural comparators.
A novel approach to improving coagulation sample ordering in an emergency department
E Murphy, C McGroarty and S MacGlone
Western Infirmary Accident and Emergency Department, Western Infirmary, Glasgow, UK
Abstract
Background: Driven by emergency department targets, there is a need for rapid initial assessment and investigation of attendees and as a consequence blood tests are often performed before full patient assessment. It has been shown that many investigations ordered in the emergency department are inappropriate. Coagulation samples are acknowledged as one of the commonest blood samples requested on admission. We aimed to determine if coagulation samples sent from our department were appropriate, develop guidance for appropriate testing and to increase the percentage of appropriate tests to 90%.
Methods: All coagulation samples sent from the emergency department over a one-week period were reviewed and the indications for testing compared to guidance developed by consensus with emergency department consultants. Feedback to clinical staff was given at education meetings and appropriate indications discussed. All coagulation sample request bottles were removed from the main clinical area and were only available in the resuscitation area.
Results: On the first data collection, 66 of 369 (17%) samples were deemed appropriate. Following our interventions, 69 of 96 (71%) samples were deemed appropriate and a further intervention is planned to attempt to reach our target.
Conclusions: Through a simple change in longstanding practice, we were able to reduce the number of inappropriate samples sent from the emergency department. This improvement could lead to a £100,000 saving annually and a cross-site collaborative study is planned to spread these improvements.
Gram Negative Bacteraemia rates in Haemodialysis’
EC Murray1, A Marek2, PC Thomson1 and JE Coia2
1Renal Unit, Western Infirmary, Glasgow
2Medical Microbiology, Glasgow Royal Infirmary, Glasgow
Abstract
Background: Patients on renal replacement therapy experience excess morbidity and mortality, infection being the second commonest cause of death. In our renal replacement therapy population, we characterised the organisms, sensitivity patterns and outcomes of Gram negative bacteraemia.
Methods: Greater Glasgow and Clyde and Forth Valley haemodialysis population data were collected 2011–2014 through a structured query language interrogation of the electronic patient record, and confirmed by an independent search of the microbiology database. Event rates were expressed as per 1000 haemodialysis-exposed days.
Results: Over 544,377 haemodialysis days, 84 patients experienced 95 Gram negative bacteraemia events, a rate of 0.175 per 1000 haemodialysis days, which varied with dialysis modality: non-tunnelled central venous catheters 4.77, arteriovenous grafts 0.24, tunnelled CVC 0.21 and arteriovenous fistulae 0.11/1000 haemodialysis days. The commonest sources of bacteraemia were CVCs (16.8%, n = 16), infected ulcers (14.7%, n = 14), urinary (10.5%, n = 10), biliary (9.5%, n = 9) and intra-abdominal (9.5%, n = 9). The principal organisms were Escherichia coli (49.47%, n = 47), Enterobacter spp. (13.68%, n = 13), Klebsiella spp. (11.58%, n = 11), Proteus mirabilis (6.32%, n = 6) and Pseudomonas aeruginosa (5.26%, n = 5). Eighty-nine per cent of Enterobacteriaceae were sensitive to gentamicin, 81% to ciprofloxacin, 92% to piperacillin-tazobactam and 100% to meropenem. Three-month patient mortality was 28.6% (n = 24). Ten patients (11.9%) had more than one Gram negative bacteraemia; of these, nine patients (90.0%) were the same causative organism.
Conclusions: CVCs and diabetic foot ulcers remain significant risk factors for Gram negative bacteraemia, highlighting the importance of vascular access planning. Despite good levels of antibiotic sensitivity, mortality remains high, supporting aggressive treatment of such pathogens.
Early initiation of antiplatelet therapy following ischaemic stroke is associated with lower recurrence rate
W Mazlan-Kepli1, RL Fulton1, M Walters1, PMW Bath2, J Dawson1 and On behalf of the VISTA Collaborators
1Institute of Cardiovascular and Medical Sciences, University of Glasgow, Western Infirmary, UK
2Stroke Trials Unit, University of Nottingham, UK
Abstract
Background: Guidelines suggest initiation of the anti-platelet aspirin within 24 h (UK), 24–48 h (ASA) or 48 h (ESO) of ischaemic stroke. The effect of earlier initiation of anti-platelets is less clear.
Methods: We used data from the Virtual International Stroke Trials Archive to explore the risk of recurrent ischaemic stroke and bleeding within 90 days in patients with ischaemic stroke according to when they commenced anti-platelet therapy (defined as early (day 0 or 1) or late (≥ day 2). We excluded patients treated with thrombolytic or anticoagulant therapy. We defined bleeding complications as intracranial haemorrhage or any major bleed. We used logistic regression analysis adjusted for important clinical factors.
Results: Among 3917 patients there were 113 recurrent strokes: 2.5% in the early group versus 3.8% with anti-platelets started day 2 or after (adjusted OR 0.63; 95% CI 0.43–0.94, p = 0.023). There was no difference in rates of ICH and major bleeds (adjusted OR 1.63; 95% CI 0.89–2.95, p = 0.112 and OR 0.85; 95% CI 0.57–1.28, p = 0.440, respectively).
Conclusions: Initiation of anti-platelet therapy early after stroke was associated with fewer recurrent stroke events without a clinically significant increase in bleeding events.
CT response to neoadjuvant chemotherapy as a predictor of survival following resection of oesophageal adenocarcinoma
M Pringle1, B Stewart1, S Sheridan2, S Ballantyne2 and P Glen1
1Department of Surgery, Southern General Hospital, UK
2Department of Radiology, Gartnavel General Hospital, UK
Abstract
Background: Consensus management for oesophageal adenocarcinoma is currently neoadjuvant chemotherapy followed by resection. The importance of staging following neoadjuvant chemotherapy has become more apparent, and currently staging which occurs post-neoadjuvant chemotherapy is by CT imaging. We aimed to determine if CT response to neoadjuvant chemotherapy predicted survival in patients with oesophageal adenocarcinoma.
Methods: A retrospective analysis of consecutive patients who underwent oesophageal resection. Clinico-radiological data were identified and pre- and post-neoadjuvant chemotherapy MDT reports were reviewed to assess response to neoadjuvant chemotherapy. Patients were grouped into improved, static or deterioration. Survival was calculated for each group and Kaplan–Meier analysis performed.
Results: One hundred and fifty patients underwent neoadjuvant chemotherapy and resection between June 2008 and January 2014. Sixty-five (43%) patients showed improved CT response, 75 (50%) had static disease and five (3%) deterioration. Five (3%) patients scans were inaccessible. Median survival for the group that showed response was 35 months compared to 30 months for static disease (deterioration group: incalculable). This difference was not statistically significant (p = 0.638). Kaplan–Meier analysis showed a non-significant trend towards increased survival in the response group.
Conclusion: In our cohort, CT response to NAC did not significantly predict survival in patients with oesophageal carcinoma although a trend is demonstrated. There are several reasons for this. An undetectable primary on pre-neoadjuvant chemotherapy CT cannot be seen to reduce in size, size of tumour does not correlate with tumour activity and pre-operative imaging cannot account for surgical factors influencing outcome. The predictive value of post-neoadjuvant chemotherapy functional imaging such as PET needs to be explored.
High incomplete excision rate is strongly associated with lobular subtype, node positivity and tumour size, but independent of hormonal and HER-2 status
Syed Adnan Kabir, James Mansell and Laszlo Romics
Department of Surgery, Victoria Infirmary, UK
Abstract
Introduction: Incomplete excision (IE) and final mastectomy (M) rates depend on numerous factors including pathology, patients’ breast size, choice of operation and comorbidities as well as surgical technique. Here, we investigated the association between histopathological characteristics and incomplete excision as well as mastectomy rates.
Methods: Data of 1389 consecutive patients underwent surgery for (non)invasive breast cancer between January 2008 and June 2012 were analysed. Statistical significance was calculated using Chi-square and Z-tests with a significance < 0.05.
Results: Overall incomplete excision rate was 13.74% (131/953), and mastectomy rate was 35.35% (491/1389). Higher incomplete excision and mastectomy rates were strongly associated with lobular subtype (IE: 26.03% (19/73); M: 51.22% (63/123); p < 0.01 versus other subtypes), node positivity (IE: 25% (36/144) versus 10.43% (68/652); p = 0 and M: 60.69% (193/318) versus 25.65% (216/842); p = 0) and tumour size (IE:T3 80%(4/5) versus T2 22.51% (43/191) versus T1 9.23% (55/596); all p < 0.01; and M:T3 95.35% (41/43) versus 59.46% (242/407) versus 16.16% (112/693); all p = 0). Incomplete excision rates were independent of hormonal and HER-2 expressions (ER + :12.55% (89/709) versus ER-:16.67% (15/90); p = 0.27 and HER2 neg:12.67% (91/718) versus HER2 pos:16.67% (13/78); p = 0.32) and it was just higher in grade 2 and 3 cancers (14.6% (60/411); p = 0.037 and 16.22% (36/222); p = 0.021 versus G1:6.86% (7/102). However, hormonal and HER-2 expressions as well as tumour grade were in strong association with mastectomy rate (ER+:33.28%(335/1007) versus ER-:48.75% (78/160); p < 0.01; HER2 neg:33.43% (341/1020) versus HER2 pos:49.65% (71/143); p < 0.01; G3:50.49% (205/406) versus G2:30.77% (172/559) versus G1:14.28% (17/119); all p = 0).
Conclusion: Higher incomplete excision rate is strongly associated with lobular subtype, node positivity and tumour size, but independent of hormonal end HER-2 expression, while tumour grade is not a strong predictor. However, all histopathological characteristics are strong predictors of final mastectomy rate.
Is cryoablation for renal cell cancers greater than 4 cm a viable treatment option?
A Mukherjee1, RS Khan1 and D Alcorn2
1Department of Urology, Gartnavel General Hospital, Glasgow, UK
2Department of Radiology, Gartnavel General Hospital, Glasgow, UK
Abstract
Background: Incidental small renal masses are commonly being discovered on routine abdominal imaging. The therapeutic approach for such lesions is an evolving paradigm. Probe ablative therapy such as cryoablation is emerging as an alternative option for select patients requiring nephron-sparing surgery. Typically, the use of cryotherapy is limited to tumours less than 4 cm in size. However, with advancing interventional cryoablative techniques, this treatment is being trialled in larger renal masses (tumours greater than 4 cm in size) with good effect. We present the outcomes of such patients from our series.
Methods: We reviewed our database of 135 patients treated with cryoablation for renal masses. A group of 11 consecutive patients were identified who demonstrated renal tumours greater than 4 cm in size on radiological imaging. The diagnosis, staging, outcomes, efficacy and morbidity associated with renal cryoablation were evaluated.
Results: The mean age at diagnosis for our study group was 66 years. All 11 patients demonstrated clear cell carcinoma on histology. The range of maximum tumour size in our series was 4.3–6.3 cm. After mean follow-up of 10 months (range 3–18 months), the cancer specific survival was 90% (n = 10/11) and overall patient survival was 100%. The treatment was well tolerated with a low complication rate.
Conclusion: In our series, cryoablative therapy appears to be an excellent curative option even for patients with renal masses greater than 4 cm in size. This modality of treatment offers encouraging oncological outcomes obviating the need for major surgery. Larger studies with longer term follow-up are needed to validate the use of this intervention as a viable primary treatment option.
Breast cancer presentation in the over 70s
L Smith, J Murray and A Lannigan
Wishaw General Hospital, Lanarkshire, UK
Abstract
Background: Older patients with breast cancer generally present later with more advanced disease. We aimed to explore the presentation of the over 70s with breast cancer, along with attitudes towards screening.
Methods: A questionnaire was sent to patients aged ≥70 at the time of breast cancer diagnosis in NHS Lanarkshire between 2006 and 2013. This detailed reasons and timing of presentation, in addition to thoughts about screening.
Results: Three hundred and fifty-two questionnaires were sent to women with a mean age of 76, 230 were returned (65%). Sixty-four per cent routinely examined themselves with 70% identifying a lump themselves. Distressingly only 36% of these patients were aware of the other signs/symptoms of breast cancer. The majority of women sought medical attention early, with 39% seeing someone within days. Personal concern was the greatest prompt for presentation (68%) followed by family or friend concern (10%). Eighty-three per cent routinely attended screening when invited, with a further 3% willing to attend if the service was routinely offered to the over 70s. Although the majority (60%) were not aware that they could opt into the screening service once over 70.
Conclusions: Despite the belief that older women are less breast aware most of our patients routinely examined themselves, identified pathology and promptly sought medical advice. This is the case despite most women having no knowledge of other signs and symptoms of breast cancer. Our cohort has also shown that they are keen to continue screening over the age of 70 if it was routinely offered.
Attitudes towards breast conservation in patients aged 70 and over with breast cancer
L Smith, S Dayal, J Murray and A Lannigan
Wishaw General Hospital, Lanarkshire, UK
Abstract
Background: The majority of breast conserving surgery is performed in younger women. There is little published information about the views of women aged ≥70 regarding breast conserving surgery and the factors which influence their decision about the type of surgery to choose.
Methods: A questionnaire was sent to patients who were aged ≥70 at the time of breast cancer surgery in NHS Lanarkshire between 1999 and 2013. This detailed surgical recommendations, treatment expectations and other factors which may have influenced any decision made, e.g. travel for radiotherapy and potential side effects.
Results: Responses were received from 339 patients, 192 of whom had a mastectomy with the remaining undergoing breast conserving surgery. Eighty-six per cent of both groups were recommended their surgical management by the surgeon. In the mastectomy group, 18% would have preferred BCS had it been an option, with 40% willing to have neoadjuvant endocrine therapy to facilitate this. Only 14% would have considered neoadjuvant chemotherapy with the same aim. Almost half of the mastectomy patients said that the risk of local recurrence following BCS was a factor which influenced their decision. Despite our BCS patients having to travel a considerable distance daily for radiotherapy, only 4% found it problematic. Eighty-eight per cent of patients who had BCS were happy with their treatment decision, 72% being happy with the cosmetic outcome.
Conclusions: Breast conserving surgery is something that patients aged ≥70 are interested in considering. More than a third of patients requiring mastectomy would be willing to take neoadjuvant endocrine therapy to attempt to facilitate breast conserving surgery.
Associations with delirium in an older adult cohort
JR Lumsden, K Hendry, V Scortichini, D Moran, DJ Stott and TJ Quinn
Department of Medicine for the Elderly, Glasgow Royal Infirmary, Glasgow, UK
Abstract
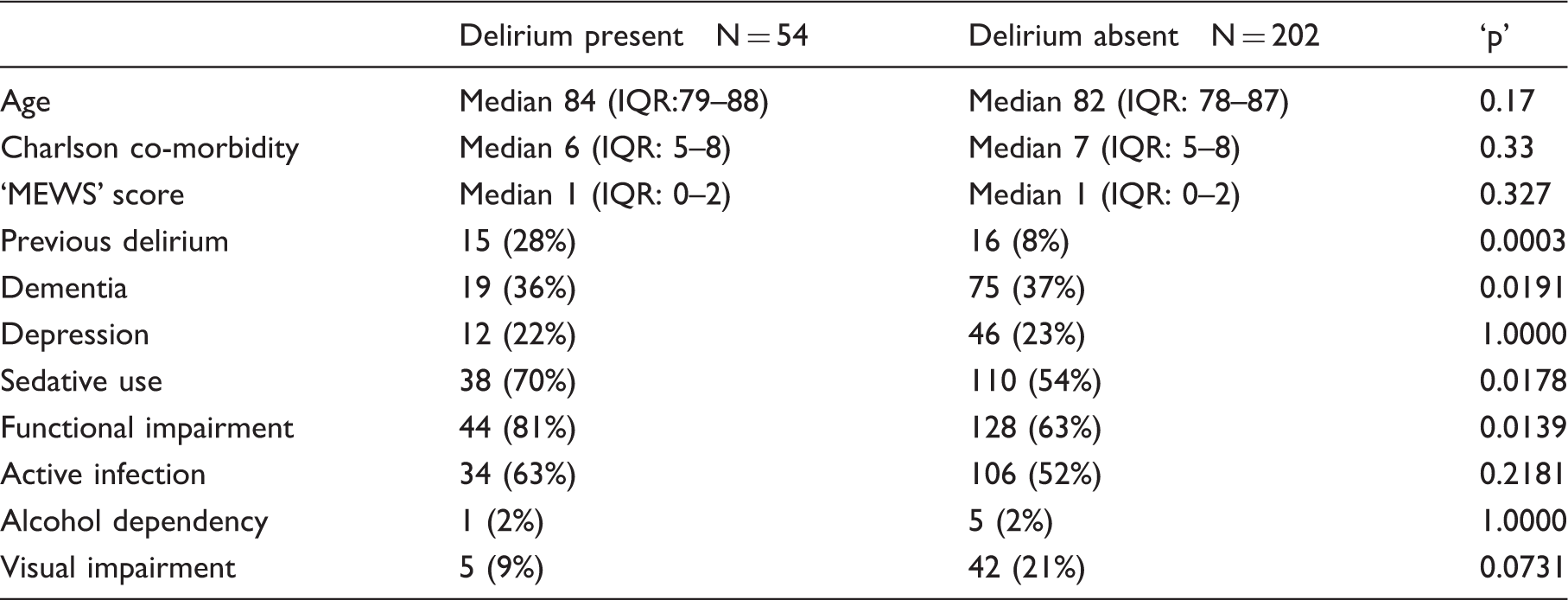
Introduction: Delirium is a common syndrome that often accompanies medical illness in hospitalised older adults. We sought to describe association of previously described delirium ‘risk factors’ in a real-world cohort of hospitalised older adults.
Methods: Participants were all older adults (age > 65 years) admitted to pre-selected geriatric assessment wards of a University Hospital. Diagnosis of delirium was made by Geriatric Medicine consultant and was based on clinical assessment (DSM-IV criteria). Diagnosis was coded as definitely present, possible or absent. Covariates of interest were based on a previous systematic literature review of associations with delirium. We examined univariate and multivariate associations with delirium. In the first instance, we excluded those with ‘possible’ delirium.
Results: Over six months data collection, we assessed and had useable data on 340 patients, of whom 54 (16%) had definite delirium and 202 (59%) did not have delirium. From analysis, univariate predictors of delirium were previous history delirium, prevalent dementia and sedative use and functional impairment (see table). On multivariate logistic regression only previous delirium diagnosis and functional impairment were independently associated with delirium.
Conclusions: In a frail older geriatric medical hospital cohort previous delirium episodes and functional impairment were independently associated with delirium. Previous delirium seems to be a particularly powerful predictor; this information could be readily added to routine data collected for older people on hospital admission.
Delirium present N = 54
Delirium absent N = 202
‘p’
Age
Median 84 (IQR:79–88)
Median 82 (IQR: 78–87)
0.17
Charlson co-morbidity
Median 6 (IQR: 5–8)
Median 7 (IQR: 5–8)
0.33
‘MEWS’ score
Median 1 (IQR: 0–2)
Median 1 (IQR: 0–2)
0.327
Previous delirium
15 (28%)
16 (8%)
0.0003
Dementia
19 (36%)
75 (37%)
0.0191
Depression
12 (22%)
46 (23%)
1.0000
Sedative use
38 (70%)
110 (54%)
0.0178
Functional impairment
44 (81%)
128 (63%)
0.0139
Active infection
34 (63%)
106 (52%)
0.2181
Alcohol dependency
1 (2%)
5 (2%)
1.0000
Visual impairment
5 (9%)
42 (21%)
0.0731
Neutrophil–lymphocyte ratio predicts survival following neoadjuvant chemotherapy in oesophageal adenocarcinoma
J Young1,2, B Stewart1,2 and P Glen1,2
1School of Medicine, University of Glasgow, Glasgow UK
2Department of Surgery, Southern General Hospital, Glasgow, UK
Abstract
Background: Neoadjuvant chemotherapy before resection is now standard of care in oesophageal adenocarcinoma. Neutrophil–lymphocyte ratio is recognised as a prognostic indicator in this disease. There is increasing evidence that staging post-neoadjuvant chemotherapy is more accurate than at time of diagnosis. We wished to assess neutrophil–lymphocyte ratio pre- and post-neoadjuvant chemotherapy in our cohort of patients.
Methods: Consecutive patients who underwent oesophageal resection after neoadjuvant chemotherapy for oesophageal adenocarcinoma between 2008 and 2013 were identified. Systemic inflammation was assessed by modified Glasgow Prognostic Score and neutrophil–lymphocyte ratio, measured at the time of diagnosis and immediately prior to resection. Patients were stratified as either low or high mGPS and neutrophil–lymphocyte ratio, and SPSS was used for statistical analysis.
Results: One hundred and sixty-nine patients fulfilled the criteria for inclusion. At time of diagnosis neither mGPS (p = 0.984) nor neutrophil–lymphocyte ratio (p = 0.808) showed any significant effect on survival. Post-neoadjuvant chemotherapy, mGPS did not show any significant effect on survival (p = 0.524). After neoadjuvant chemotherapy neutrophil–lymphocyte ratio significantly stratified survival: neutrophil–lymphocyte ratio ≤2.5, median survival of 38 months, neutrophil–lymphocyte ratio 2.5–5 median survival 21 months and neutrophil–lymphocyte ratio >5 median survival of 15 months (P = 0.003).
Conclusion: Neutrophil–lymphocyte ratio post-neoadjuvant chemotherapy is a predictor of survival following oesophageal resection for oesophageal adenocarcinoma. This supports recent findings that suggest staging investigations post-neoadjuvant chemotherapy should determine patients’ suitability for resectional surgery.
Metabolic risk factors in south Asian women of reproductive age with polycystic ovarian syndrome
MA Shah, MA Lumsden and S Iliodromiti
Reproductive and Maternal Medicine, University of Glasgow, UK
Abstract
Background: Women of South Asian origin with polycystic ovarian syndrome are thought to be more insulin resistant and thereby at greater risk of future type 2 diabetes and cardiovascular disease than their European counterparts. However, their excess risk is not fully attributed to conventional risk factors. Our aim was to assess lifestyle factors, cardiometabolic biomarkers and endothelial reactivity in South Asian women in the UK with polycystic ovarian syndrome compared with women of white descent.
Methods: South Asian and European women aged 18–39 years with diagnosed polycystic ovarian syndrome were recruited. Women with existing cardiometabolic disease or on hormonal therapy were excluded. Dietary data, objectively measured physical activity (with the use of accelerometers), cardiorespiratory fitness and central adiposity were measured. Vascular reactivity was assessed with the use of Laser Doppler Imaging with Iontophoresis. Fasting bloods were collected for routine biomarkers.
Results: Nine South Asians and six Europeans with polycystic ovarian syndrome were recruited. The South Asians had greater levels of HbA1c (p = 0.02), a lower mean HDL of 1.03 ± 0.2 mmol/l (p = 0.03), decreased sex hormone binding globulin (p = 0.002) and a greater mean free androgen index of 7.3 ± 3.3 (P = 0.04) compared with the women of white descent. In addition, the South Asians exhibited lower levels of vigorous physical activity (p = 0.006) and reduced reactivity to both endothelium dependent and independent chemicals than their comparators.
Conclusion: South Asian women with polycystic ovarian syndrome exhibit an adverse cardiometabolic profile along with early vascular impairment. Early intervention targeting modifiable risk factors can potentially ameliorate their metabolic profile.
Trends of improvement in survival with era of treatment in patients with multiple myeloma and renal impairment
W G Dunn1, R Soutar2, A Laing3, CC Geddes3 and PB Mark1,3
1School of Medicine, University of Glasgow, UK
2Beatson West of Scotland Cancer Centre, UK
3Glasgow Renal and Transplant Unit, Western Infirmary, UK
Abstract
Background: Renal impairment is a leading cause of mortality in patients with myeloma. We aimed to distinguish whether treatment advances over three decades had resulted in improved survival for patients with myeloma and renal impairment, and to identify prognostic factors.
Methods: All myeloma patients who attended the Glasgow Renal Unit between October 1985 and June 2014 were identified from the prospectively acquired renal database. Baseline clinical and laboratory data at presentation were retrieved. Time to death was calculated and Cox regression used to identify covariates significantly associated with survival.
Results: Three hundred and twenty-four patients were identified (mean age 67.9 years, 61.1% male), 217 (67%) had complete data for use in the proportional hazards model. Median survival from presentation to the renal unit was 433 days, 48.8% of patients received dialysis. Multivariate analysis of patients not receiving dialysis demonstrated age at presentation (HR 1.044, p = 0.002) and serum albumin (HR 0.909, p < 0.001) as being significantly associated with survival. This also demonstrated improved survival in the most recent decade (p = 0.011). In patients receiving dialysis, date of presentation was not significantly associated with survival. Predictors of death in this group were age and eGFR at presentation.
Conclusions: Outcomes for patients with renal impairment and myeloma remain poor. In patients not requiring dialysis, it appears that outcomes are improving compared to historical cases. This does not appear to be the case in those requiring dialysis. Further work is required to define the contribution of age and co-morbidity to outcome in patients needing dialysis, to optimise treatment decisions.
Determining the relationship between clot length and successful recanalisation rates with intravenous thrombolysis in acute ischaemic stroke
M Abdullah1 and K Muir2
1Medical Student, University of Glasgow, UK
2Department of Neurology, Southern General Hospital, UK
Abstract
Background: A retrospective study to validate the reported relationship between clot length and treatment response investigating the purported 8 mm threshold at which intravenous thrombolysis is no longer effective in acute ischaemic stroke.
Methods: Using a dataset of 105 stroke patients comparing alteplase to tenecteplase patients exhibiting a hyper-dense clot visible on thin slice non-contrast computer tomography in the middle cerebral artery were selected. Images were reconstructed to 2.5 mm thickness and clots were measured. Recanalisation was assessed with CT angiography using the TIMI scoring system with a score of 2–3 considered recanalised. ROC curve and logistic regression analysis were carried for all patients and just alteplase patients.
Results: Thirty-nine patients had visible clots on NCCT. When only including patients who received alteplase (20 patients) p values were reduced with ROC curve having an area under the curve of 0.738 (p = 0.099). A 9 mm threshold for recanalisation failure showed a sensitivity and specificity of 83.3 and 71.4%, respectively. Logistic regression with output as recanalisation failure had an odds ratio of 1.036 for every millimetre increase in clot length (p = 0.398). Five patients recanalised having a clot length of 8 mm or longer.
Conclusion: 8 mm is not an absolute threshold for recanalisation failure. As clot length increased, recanalisation was more likely to fail in alteplase only patients although investigation needs to be repeated with higher patient number for significant results.
Aneusomy detected by FISH has high positive predictive value for Barrett’s dysplasia
EAG Allan1, R Miller2 and JJ Going2
1University of Glasgow, UK
2Pathology, Southern General Hospital Glasgow, UK
Abstract
Aim: The goal of this study was to pilot a commercial four-colour fluorescence in situ hybridisation probe set as a marker of dysplasia in surveillance biopsies of patients with Barrett’s oesophagus. To determine whether dysplastic tissue could be correctly identified and differentiated from normal tissue based on gene copy number recognised using four-colour fluorescence in situ hybridisation.
Methods: Four-colour fluorescence in situ hybridisation probes to 9p12 (CDKN2A), 17q11.2-12 (HER2), 8q24.12-13 (CMYC) and 20q13.2 (ZNF217) in 20 cases of Barrett’s oesophagus. Dysplastic and non-dysplastic mucosa were compared for each case. Two observers independently counted 50 cells in each region of interest, and the mean score taken. Wilcoxon’s signed rank test was used to determine the significance of differences between dysplastic and non-dysplastic tissue. Predictive power was determined by logistic regression and receiver operator characteristic curves were plotted to examine sensitivity and specificity of each gene to detect dysplasia.
Results:HER2, CMYC, and ZNF217 showed significant (p < 0.0005) increases in copy number in dysplastic mucosa, CDKN2A had an insignificant (p = 0.852) decrease when compared to non-dysplastic mucosa. While aneusomy was strongly predictive of dysplasia, eusomy did not rule it out. Inter-observer agreement was excellent.
Conclusions: Increased HER2, CMYC and ZNF217 copy number distinguished dysplastic from non-dysplastic mucosa, but non-detection of aneusomy did not exclude dysplasia. Further studies are justified to determine whether four-colour fluorescence in situ hybridisation-positive dysplasia might justify earlier treatment by radio-frequency ablation.
Patterns of CMV infection post renal transplant
AF Sheldon1, M Clancy2 and P Thomson1,2
1Wolfson Medical School, University of Glasgow
2Department of Renal Transplantation, Western Infirmary
Abstract
Background: CMV infection post renal transplant is most common in seronegative recipients of seropositive donors (donor+/recipient-) leading to widespread use of antiviral prophylaxis. CMV infection manifests at a lower incidence in the non-prophylaxed combinations. We evaluate incidence and timing of CMV viraemia and disease in all donor/recipient serological combinations.
Methods: This study included consecutive renal transplant patients from 1 July 2010 to 30 June 2013 with a minimum of one year follow-up. Demographic data, donor/recipient pre-transplant CMV status and post-transplant CMV PCR were extracted from a prospectively compiled, electronic patient record. Time to CMV DNA PCR positivity was calculated in all groups.
Results: Pre-transplant CMV status was established for 294/335(87.7%) transplantations. 23.5% (69/294) were in the prophylaxis group (D+/R-). 43.5% (30/69) of the prophylaxis group encountered CMV viraemia post-transplant (27.5% (19/69) symptomatic) versus 8.9% (20/225) in the non-prophylaxis group (1.8% (4/225) symptomatic). Peak incidence of CMV viraemia was at 90 days in the non-prophylaxis group compared to 270 days post-transplant in the prophylaxis group.
Conclusion: CMV viraemia occurs in the high-risk group despite prophylaxis but mostly later than six months post-transplant. Clinicians should maintain a high level of clinical suspicion for CMV infection in non-prophylaxed patients early post-transplant. In patients who receive prophylaxis, infection is more likely 6–18 months post-transplant.
Concussion: an investigation of current guidance from UK sporting bodies
KG McGivern1, J Hay2 and W Stewart1,2
1University of Glasgow, UK
2Neuropathology Research Laboratory, Laboratory Medicine Building, Southern General Hospital, UK
Abstract
Background: High profile cases in a variety of sports have focused attention on the potential immediate and long-term consequences of concussion, together with an apparent lack of consistency in concussion management across sport. Further, a recent survey of Scottish educators demonstrated knowledge gaps around concussion management, suggesting ineffective messaging.
Aim: To explore the availability and quality of UK sports organisations concussion management guidelines.
Methods: The websites of a range of sports governing bodies were interrogated for publically available guidance on concussion management. Where no information was available online, this information is sought via direct follow-up emails and telephone calls. In each case, where available, the concussion advice was assessed against the International Rugby Board’s multi-author ‘Concussion Guidance for the General Public’, and a 25-point IRB CONcussion score generated reflecting performance against a minimum dataset.
Results: Of 48 UK sports organisations’ websites examined, only seven (15%) had information on concussion management in the public domain, with no further guidance received from follow-up mails or calls where no online information was available. Of the seven organisations with concussion information, ICON scores ranged from 1/25 (British Horseracing) to XX/25 (English Hockey), with considerable variation in detail on concussion management between guidelines.
Conclusion: This review demonstrates a clear lack of publically available information on concussion management from UK sports governing bodies. Further, in the few instances where information is present, there is inconsistency in messaging. There is a pressing need for generic, robust and consistent messaging on concussion management.
Functional analysis of related patient-derived HCV envelope sequences: identifying novel epitopes required for virus entry into host cells
R Swann1, J Hamilton2, R Wilson2, S Cole1, V Cowton1 and A Patel1
1The University of Glasgow, Centre for Virus Research, UK
2The University of Glasgow, School of Medicine, UK
Abstract
Background: Hepatitis C Virus currently affects 2% of global population. Current effective therapies are unlikely to achieve global eradication without a vaccine. Studying mechanisms of viral entry into host cells can help inform future vaccine design. Hepatitis C virus has a high rate of mutation, therefore studying related envelope protein (E1E2) sequences derived from individual patients allows us to compare the functional impact of single amino acid (aa) changes. Our aim was to identify ‘aa’ changes in Hepatitis C virus envelope proteins associated with a loss of infectivity.
Method: Plasmids expressing different related HCV E1E2 derived from individual patients were used to make a panel of viral ‘pseudoparticles’ of Genotype 1 and 3. These pseudoparticles were tested for their ability to infect hepatoma cells in vitro. Some were found to be infective, others not. We confirmed expression of E1E2 in by these constructs using ELISA with two anti-envelope antibodies. Using MEGA-6 software, ‘aa’ sequences of expressed envelope proteins producing infective pseudoparticles, and those derived from the same patient not producing infective pseudoparticles, were compared.
Results: Four sequences had single amino acid changes which appeared to render pseudoparticles non-infective. For genotype 3, S118P and M191T and in genotype 1, D653G and I709T amino acid changes produced non-infective sequences which still expressed E1E2.
Conclusion: Studying the functional properties of related HCV envelope sequences can yield valuable information. We have identified four ‘aa’ changes, which may affect HCV cell entry. These require further testing to determine precise mechanisms.
Delineating the role of mTOR kinase in chronic lymphocytic leukaemia
SP Bowers, A Holroyd, E Cosimo and AM Michie
Institute of Cancer Sciences, University of Glasgow, UK
Abstract
Background: Chronic lymphocytic leukaemia is currently incurable with chemotherapeutic agents. The microenvironment within lymphoid organs attracts chronic lymphocytic leukaemia cells and promotes their survival and proliferation. CXCL12 encourages migration to the microenvironment via the PI3K/Akt/mTOR pathway. The aim of our study is to assess the role of mTOR kinase in chronic lymphocytic leukaemia cell migration and define the molecular events that allow migration to occur.
Methods: Primary chronic lymphocytic leukaemia cells from 11 patients were stimulated with CXCL12 before treatment with mTOR inhibitors, AZD8055 (mTORC1/2) and rapamycin (mTORC1). Western blotting assessed short-term stimulations (0.5, 1 and 4 h). Long-term stimulations (48 and 96 h) assessed cell viability by flow cytometry (Annexin-V/7AAD). CLL cell migration towards CXCL12 was assessed using transwell migration and pseudoemperipolesis ± mTOR inhibitors.
Results: Short-term CXCL12 stimulation showed an increase in mTORC1, mTORC2 and ERK signalling (pS6, pNDRG1 and pERK, respectively). AZD8055 and rapamycin inhibited mTORC1 activity, while mTORC2 activity was only reduced by AZD8055. ERK signalling was non-significantly reduced by rapamycin. Long-term CXCL12 stimulation increased chronic lymphocytic leukaemia cell survival, which was reduced by AZD8055 and rapamycin. CXCL12-mediated chronic lymphocytic leukaemia cell migration via pseudoemperipolesis was reduced by AZD8055 and rapamycin, with the decrease elicited by AZD8055 showing significance. AZD8055 also reduced transwell migration.
Conclusions: These findings confirm the importance of mTOR in chronic lymphocytic leukaemia cell migration, with only dual mTOR inhibition significantly reducing CXCL-12-mediated chronic lymphocytic leukaemia cell migration in vitro. Due to the success of other inhibitors of migration, our data support dual mTOR inhibition as a successful inhibitor of CLL cell migration.