
Abstract

ABSTRACT BOOK
Doubletree by Hilton Dunblane Hydro, Perthshire
Scottish Society of Physicians is a charity registered in Scotland. No. SC029462
CONTENTS
• Session 1 3
• Session 2 4
• Session 3 5
• Session 4 6
ORAL PRESENTATIONS
Friday 30 October 2015
Session 1
Chair: Dr Stuart Paterson
Upper GI bleeding and recent advances
Honorary Associate Professor, Glasgow Royal Infirmary, Glasgow
Abstract
Upper GI bleeding remains a common cause of presentation to hospital, with a mortality of approximately 10%. Early risk assessment is important to both identify high-risk patients requiring emergency endoscopy after resuscitation and the very low-risk patients who can avoid admission. All other patients should have endoscopy within 24 h.1,2 Proton pump therapy is of proven benefit after application of endoscopic therapy to high-risk ulcers, but is not of clear benefit prior to endoscopy. 1 Recent studies suggest that a relatively restrictive blood transfusion strategy improves outcome, although the exact haemoglobin threshold remains unclear. If endoscopic methods fail to control non-variceal bleeding, interventional radiology (IR) should be employed, with surgery undertaken if there is delay in organising IR. 1
Patients suspected of variceal bleeding should be given vasopressors and prophylactic antibiotics as soon as possible. 2 If endoscopy fails to control variceal bleeding, placement of a temporary Sengstaken tube may be used as a bridge to repeat endoscopy or TIPSS procedure. 2 Clear protocols and pathways are essential for managing patients presenting with upper GI bleeding, with 24/7 access to endoscopic therapy, IR and surgery available on-site, or via clear and agreed regional networks. 3
References
Acute kidney injury – information for general physicians
Consultant Nephrologist, Lead Clinician and Honorary Clinical Associate Professor, South Glasgow University Hospital, Glasgow
Abstract
AKI is a feature of severe illness in many patients under the care of physicians. This talk will address some of the common questions arising in patients with AKI including assessing fluid requirements, diuretics, intravenous contrast administration, restarting of ACE inhibitors, when to refer to nephrology and long-term follow up.
Comprehensive geriatric assessment – what a general physician should know and do when seeing an elderly/frail patient
Consultant Geriatrician & Honorary Senior Clinical Lecturer, Monklands Hospital, Lanarkshire
Session 2
Chair: Dr Allan Bridges
Diabetic for other specialists
President Elect, Scottish Society of Physicians & Consultant Physician, Glasgow Royal Infirmary
Abstract
There are now a baffling number of different treatments for type 2 diabetes. New drugs have been introduced which work in ways that are complementary to older therapies such as metformin, sulphonylureas and insulin. Several diabetes therapies have side effects that can lead to the patient being sent for detailed investigations, where a careful drug history would have been better.
Fever in travellers from West Africa – Ebola
Consultant Infectious Diseases Physician, Gartnavel General Hospital, Glasgow
FITZGERALD PEEL LECTURE
Heart failure: current and new therapies
Consultant Cardiologist, Queen Elizabeth University Hospital, Glasgow
Abstract
Few conditions have seen such enormous progress in treatment (and improvements in outcomes) as chronic heart failure due to left ventricular systolic dysfunction (i.e. with reduced ejection fraction – HF-REF). By the early 2000s ACE inhibitors (or angiotensin receptor blocker if intolerance) and beta-blockers had become the cornerstone of disease-modifying therapy. 1 Thereafter, the two major thrusts of research effort were investigation of the value of devices and whether adding a third drug might improve outlook further. A decade of effort showed the effectiveness of the implantable cardioverter defibrillator in reducing the risk of sudden death and cardiac resynchronisation therapy (CRT) in reducing the risk of both death and hospital admission in selected patients with HF-REF. Similarly, initially angiotensin receptor blockers 2 and subsequently, and more convincingly, mineralocorticoid receptor antagonists, 3 were shown to improve mortality and morbidity across the symptom spectrum (as was CRT). 1
By 2012, guidelines were recommending that most patients with HF-REF are candidates for an ACE inhibitor, beta-blocker and MRA (and many for an ICD, CRT or both). 1
The latest breakthrough has come from a different therapeutic paradigm. This not only took a different pathophysiological approach but also adopted a ‘replacement’ rather than ‘add-on’ strategy. The angiotensin receptor neprilysin inhibitor (ARNI) sacubitril/valsartan was designed not only to block the renin-angiotensin system but also, by inhibiting the enzyme neprilysin, to augment potentially beneficial, endogenous, neurohumoral pathways such as natriuretic peptides, bradykinin and adrenomedullin. In a head-to-head comparison with enalapril, sacubitril/valsartan reduced both cardiovascular death and heart failure hospitalisations by a fifth and improved patient well-being. 4 We now have a better alternative than a gold-standard that has stood the test of time for more than a quarter of a century. I am sure we will continue to be successful in the war against heart failure.
References
Saturday 31 October 2015
Session 3
Chair: Professor Miles Fisher
Delivering future hospitals
Consultant Physician & Clinical Director, Urgent Care Division, Countess of Chester Hospital NHS Foundation Trust
Abstract
The Future Hospital Commission (FHC) was launched in September 2013 with much fanfare, including being recognised by The Lancet as ‘the most important statement about the future of British medicine for a generation’. Recommendations from that report were based on the very best of UK hospital services, taking examples of existing innovative and patient-centred services to develop a comprehensive model of care.
The RCP(L) established the Future Hospital Programme to implement the recommendations of the Future Hospital Commission taking the report from page to practice. In its first year of operation it has established four development sites operationalising and implementing change around the care delivered to the acutely unwell frail elderly and a series of metrics are in place to evaluate the changes which are being implemented across the sites. The programme is currently recruiting an additional four sites to model innovative ways of improving services across health systems. The programme also hosts a wide range of projects and workstreams across the RCP doing great work under the Future Hospital umbrella. These include work to promote shared decision making and support for developing the chief registrar role.
Through the Future Hospital Programme, we are now building an active and evolving partnership network of peers, experts, academics, organisations and patients who are key supporters of the Future Hospital, implementing ideas and recommendations relating to the Future Hospital and sharing their findings. To support this network in the active sharing of tools, knowledge and experience, we are in the process of developing an online hub where members of the Partners Network will be able to access key resources related to service improvement.
We are asking clinicians to tell us about new service models that align with the Future Hospital recommendations, with the aim of providing a platform through which clinicians are able to share and learn from examples of innovative practice from across the country. This information will be collated on the RCP website through the Tell us your story database.
Rheumatoid arthritis – new models of care and new drugs. What a general physician needs to know
Consultant Rheumatologist, Glasgow Royal Infirmary
Abstract
In the last twenty years major changes in the management of rheumatoid arthritis (RA) have resulted in significantly improved outcomes for patients living with this progressive chronic inflammatory disease.
The advent of tumour-necrosis factor antagonists and subsequently other novel biologic therapies greatly raised the bar in terms of patient and physician expectations of what could be achieved. Biologics, however, are only one of a number of interventions that have led to remission being an achievable goal in many RA patients.
The modern management of RA is underpinned by two main principles: (1) early diagnosis and initiation of disease modifying anti-rheumatic drugs and (2) the ‘treat to target’ strategy. This strategy involves setting an objective treatment target of remission (or at least low disease activity), undertaking regular formal measurements of disease activity and adjusting therapy to achieve that target. This approach is supported by an increasing evidence-base of clinical trials incorporating ‘treat to target’ principles demonstrating improved clinical, functional and radiological outcomes. These clinical trials also show that similar remission rates can be achieved with a number of different therapeutic agents, highlighting that it is the ‘treat to target’ principle that is key.
Despite significantly improved outcomes, the management of RA still presents many challenges to the rheumatologist and the general physician: potential long term toxicities with complex drug regimens, optimally caring for patients on lifelong immunomodulatory therapies and managing cardiovascular health in this at risk population. Until we can achieve drug free remission in all RA patients, these challenges will remain.
Session 4
Chair: Professor Miles Fisher
(Presenting author underlined)
Optical coherence tomography in chronic kidney disease: vasculopathy in the eye linked to kidney injury, inflammation and endothelial dysfunction
British Heart Foundation Intermediate Clinical Research Fellow & Honorary Consultant Nephrologist, University of Edinburgh
Email:
Abstract
References
Using PCR to help reduce admissions to an Ebola Treatment unit
General Duties Medical Officer, 39 Royal Engineers, Kinloss, Scotland
Email:
Abstract
In October 2014, a British Army field hospital deployed to the Freetown peninsula in Sierra Leone as part of the UK government’s response to the Ebola epidemic in West Africa. A 12-bed Ebola treatment unit was established for local and international healthcare workers. Approximately 50 staff were expected to have close contact with confirmed Ebola patients or samples on a daily basis, so called ‘Red Zone workers’. Hence, there was concern that red zone workers presenting with an undifferentiated fever or gastroenteritis would have to be treated as a case of suspected Ebola.
References
CT coronary angiography in the West of Scotland: is it reflective of NICE guidance and how does it compare with PROMISE?
Medical Student, Golden Jubilee National Hospital, Glasgow
Abstract
The results of the recent PROMISE 2 and SCOT-HEART 3 studies, which included moderate and high risk patients have added to the debate and there remains a divergence of opinion regarding the appropriateness of CTCA in this patient group. In particular, there is a concern that CTCA may increase the number of future invasive coronary angiograms. We studied patients referred to the CTCA service in our centre and compared their predicted risk, prior stress testing and subsequent investigations to the NICE guidance and with data from the PROMISE study.
Proportion of patients undergoing CTCA according to the likelihood of CAD.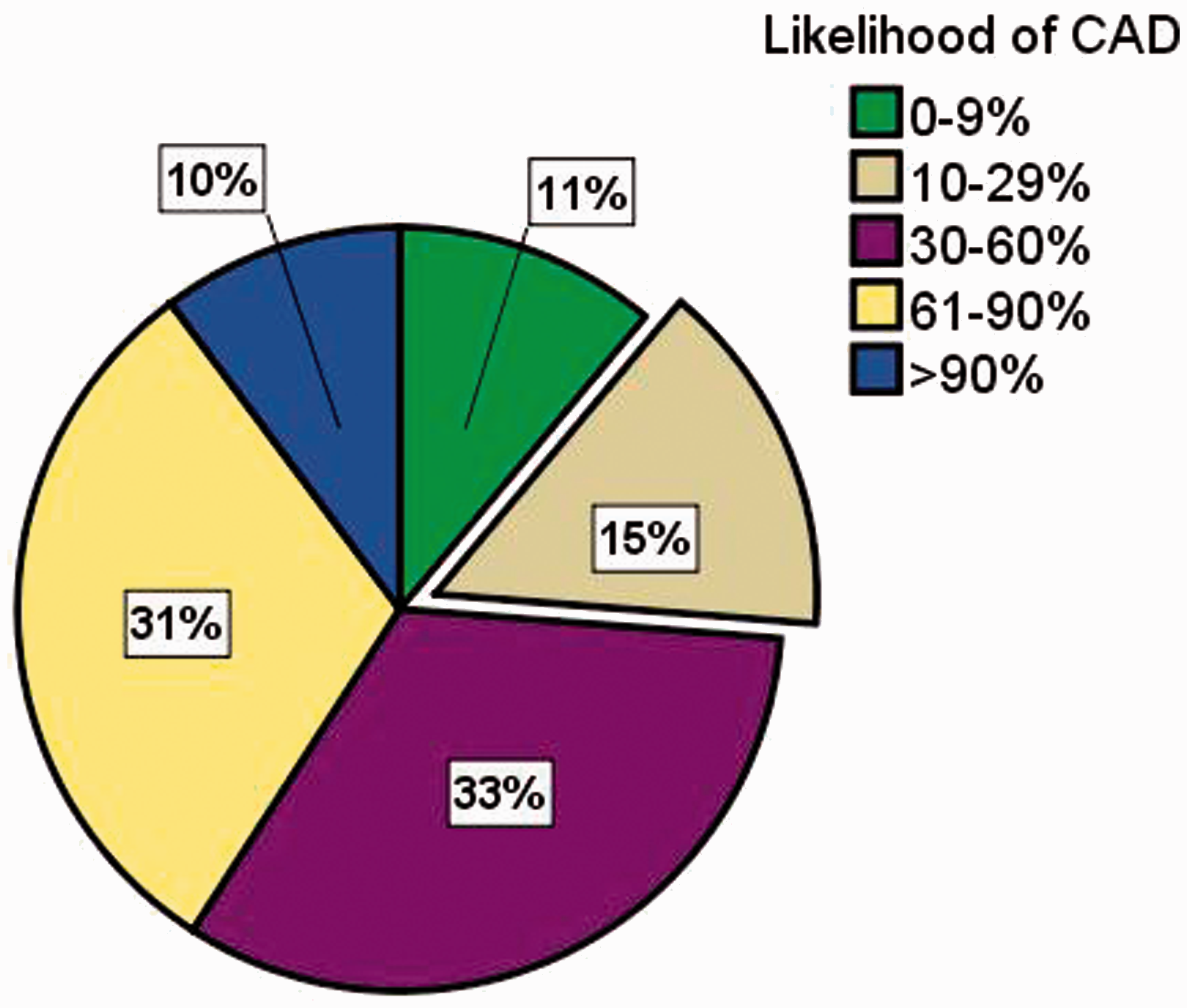
References
Fitzgerald Peel Prize Winner
The effect of the sodium-glucose co transporter Dapagliflozin on weight, blood pressure and lipid profiles in a Scottish Teaching Hospital
Medical Student, University of Glasgow, UK
Abstract
We sought to ascertain the relative benefits of one of these agents, the first in class Dapagliflozin, on cardiovascular risk profile, in a planned, observational analysis of routine care in a university hospital.
Reference
Is home blood pressure monitoring viable within a large-scale web-based randomised trial of timing of blood pressure therapy and effect on cardiovascular outcomes?
British Heart Foundation Clinical Research Fellow, Medicines Monitoring Unit (MEMO) and Hypertension Research Centre (HRC), Ninewells Hospital, Dundee
Abstract
240 different models of BP monitor were reported. 62% of participants’ monitors were validated by international protocols. 124 devices were British Hypertension Society validated.
1755 sets of home blood pressure measurements were submitted by 680 participants. To June 2015, participants had entered between 1 and 13 sets of measurements (mean 3). 550 participants have submitted at least 3 sets of measurements. 48(2.7%) sets of measurements contained insufficient information to calculate mean morning and evening blood pressures.
References
IVC diameter predicts severity of renal dysfunction and survival in patients with heart failure
Clinical Research Fellow and Honorary Speciality Registrar in Cardiology University of Dundee, Division of Cardiovascular & Diabetes Medicine, Ninewells Hospital & Medical School, Dundee.
Abstract
References
INDEX OF POSTER PRESENTATIONS
PB01
Prognosis from malignant pleural mesothelioma: what is it and what influences it?
Core Trainee Year 2 ACCS – Acute Medicine (Acute Care Common Stem). Aberdeen Royal Infirmary. University of Aberdeen, Aberdeen
PB02
Recognition of medical specialty patients in the acute medicine unit
FY1, Forth Valley Royal Hospital, Larbert
PB03
Assessment of delirium – introducing the TIME bundle into the Geriatric Assessment Unit in Aberdeen Royal Infirmary
FY1 Doctor, Geriatrics Aberdeen Royal Infirmary, NHS Grampian
PB04
Optimising medical cardiovascular secondary prevention – a quality improvement project with the Vascular Department
FY1, Forth Valley Royal Hospital, Larbert
PB05
Inter-observer variability of two classification systems for stroke aetiology
Clinical Lecturer, University of Glasgow, Glasgow
PB06
Audit of medical management of patients with Graves’ disease
FY2, Queen Elizabeth University Hospital, Glasgow
PB07
State-of-the-art pharmacotherapeutics of chronic HCV infection in decompensated cirrhotic patients using recently licensed novel direct-acting antivirals
Consultant Physician, Dumfries & Galloway Royal Infirmary, Dumfries
PB08
Hepatitis E in South-East Scotland – a relationship between men, meat and medicines
Clinical Research Fellow, Royal Infirmary of Edinburgh, Edinburgh
PB09
Chronic cough prior to secondary care referral: is enough being done?
FY1 in General Surgery, Aberdeen Royal Infirmary, Aberdeen
PB10
SMC assessment of medicines for end of life care and rare conditions: the initial year’s experience of a new approach
Chief Pharmacist, Scottish Medicines Consortium, Glasgow
PB11
A Study on the management of corticosteroid side effects in cancer patients
Foundation Medical Officer 2 Trainee, Mater Dei Hospital, Malta
PB12
The National COPD Audit: a local Scottish perspective
Specialty Registrar 4 at Department of Respiratory Medicine, Forth Valley Royal Hospital, Larbert
PB13
The impact of SIGN Guidelines on stroke services in NHS Tayside
Core Medical Trainee 1, Ninewells Hospital, Dundee
PB14
Skin protection amongst IBD patients on immunosuppressants: an audit of current practice
FY2, Department of Gastroenterology, Victoria Hospital, Kirkcaldy
PB15
Unexpected clinical characteristics of upper extremity DVTs
SHO, Acute Medicine, Royal Infirmary of Edinburgh, Edinburgh
PB16
Long-term outcomes of DVT involving upper extremities
SHO, Acute Medicine, Royal Infirmary of Edinburgh, Edinburgh
PB17
2 in 1 – type and go – a focused electronic assessment record as an immediate discharge summary
SHO, Acute Medicine, Royal Infirmary of Edinburgh, Edinburgh
PB18
‘Beat Diabetes’ – a Legacy of the 20th Commonwealth Games in Glasgow
ST4 Diabetes & Endocrinology, Glasgow Royal Infirmary, Glasgow
PB19
Confidence levels of junior doctors in managing hospital in-patients with diabetes; the Trainees Own Perception of Delivery Of Care (TOPDOC) Diabetes Study
Core Medical Trainee, Department of Diabetes & Endocrinology, Glasgow Royal Infirmary
PB20
Effect of haemodialysis on markers of platelet activation in diabetic and non-diabetic patients
Consultant Physician, Raigmore Hospital, Inverness Division of Health and research, University of Highlands & Islands, Inverness
PB21
Accuracy of weight-based antibiotic calculations in an acute care setting
CT1, Forth Valley Royal Hospital, Larbert
PB22
Statins in primary care; What’s holding us back?
Medical Student, University of Dundee, Dundee
BEST POSTER PRIZE: (PB23)
PB23
AKI recognition and management in the first 24 hours in FVRH
ST4, Forth Valley Royal Hospital, Larbert
PB24
AKI referrals to the renal on call service: presentation and short term outcomes
ST4, Forth Valley Royal Hospital, Larbert
PB25
The role of the chest radiograph in correctly diagnosing pneumonia and the contribution of further imaging
Foundation Year 2 doctor, Thoracic Medicine Department, Royal Free Hospital, London
Consultant, Royal Free Hospital, London
PB26
Metabolomic study of the impact of shift working in junior doctors
GPST3, University of Glasgow, Glasgow
PB27
‘Think Delirium Write Delirium’ – recognition and management of delirium in Raigmore Hospital, Inverness
ST2-ST3, Raigmore Hospital, Inverness
PB28
An examination of acute medical units in Scottish Hospitals
Clinical research fellow, Royal College of Physicians of Edinburgh and 2Post graduate MD student, Centre of Population Health Sciences, University of Edinburgh
PB29
The TIME (Treatment in Morning versus the Evening) study: a novel randomised trial of timing of antihypertensive therapy administration
Clinical Research Fellow, Medicines Monitoring Unit (MEMO) and Hypertension Research Centre (HRC), University of Dundee, Ninewells Hospital, Dundee
PB30
Potential application of guidelines for investigation of chest pain admissions to the clinical decisions unit (CDU) – a scoping exercise
ST1 Emergency Medicine, Ayr University Hospital, Ayr
PB31
Audit of the use of intermittent pneumatic compression stockings on the Acute Stroke Unit, Glasgow Royal Infirmary
FY1 Acute Stroke Unit, Glasgow Royal Infirmary, Glasgow
PB32
Audit on documentation of pleural procedures in the respiratory department
CT2, Borders General Hospital, Melrose
PB33
Liver function test predicts mortality and hospitalisation among ambulatory heart failure patients
Clinical Research Fellow, University of Dundee, Dundee
BEST STUDENT POSTER PRIZE: (PB34)
PB34
A long-term observational study on surveillance and incidence of cardiotoxicity in breast cancer chemotherapy
Masters Student, University of Dundee, Dundee
PB35
Is the Community Geriatric Team preventing hospital admission?
FY2, Community Geriatrics, DOME, NHS Grampian
PB36
A combination of PillCam®SB2 and SmartPill® in the investigation of patients with known or suspected Crohn’s disease, referred for small-bowel assessment and their association with faecal calprotectin levels; case series
FY1, Victoria Hospital Kirkcaldy