
Abstract
A 65-year-old man presented with a six-month history of lethargy, weight loss and dry cough. He had a background of mild chronic obstructive pulmonary disease. Chest radiograph showed new right upper lobe cavitary opacification. Sputum cultures were acid-fast bacilli smear positive and yielded Mycobacterium marinum – a non-tuberculous mycobacterium (NTM) often found in aquatic environments and rarely associated with respiratory disease. The suspected source was silent aspiration of contaminated water, likely due to his initiating the siphon of his fish-tank by mouth. He completed a one-year course of rifampicin, ethambutol and clarithromycin, with negative repeat sputum mycobacteria cultures and radiological improvement. This case report demonstrates a successful approach to investigation and further management of Mycobacterium marinum pulmonary disease – a rare condition, particularly in immunocompetent individuals, with limited treatment guidelines.
Case presentation
A 65-year-old man was referred to the respiratory outpatient clinic with a six-month history of lethargy, weight loss of 4 kg and non-productive cough. He was a current smoker (25-pack year history) and medical history included mild chronic obstructive pulmonary disease and neurofibromatosis. Regular medications were beclomethasone diproprionate 400 µg per day, tiotropium bromide 18 µg once daily, salbutamol MDI as required and omeprazole 20 mg once daily. He had received a Bacillus Calmette-Guérin (BCG) vaccination in childhood, and there was no significant occupational exposure or family history. He had in the past kept fish, which he had given to his daughter eight months previously.
Investigations
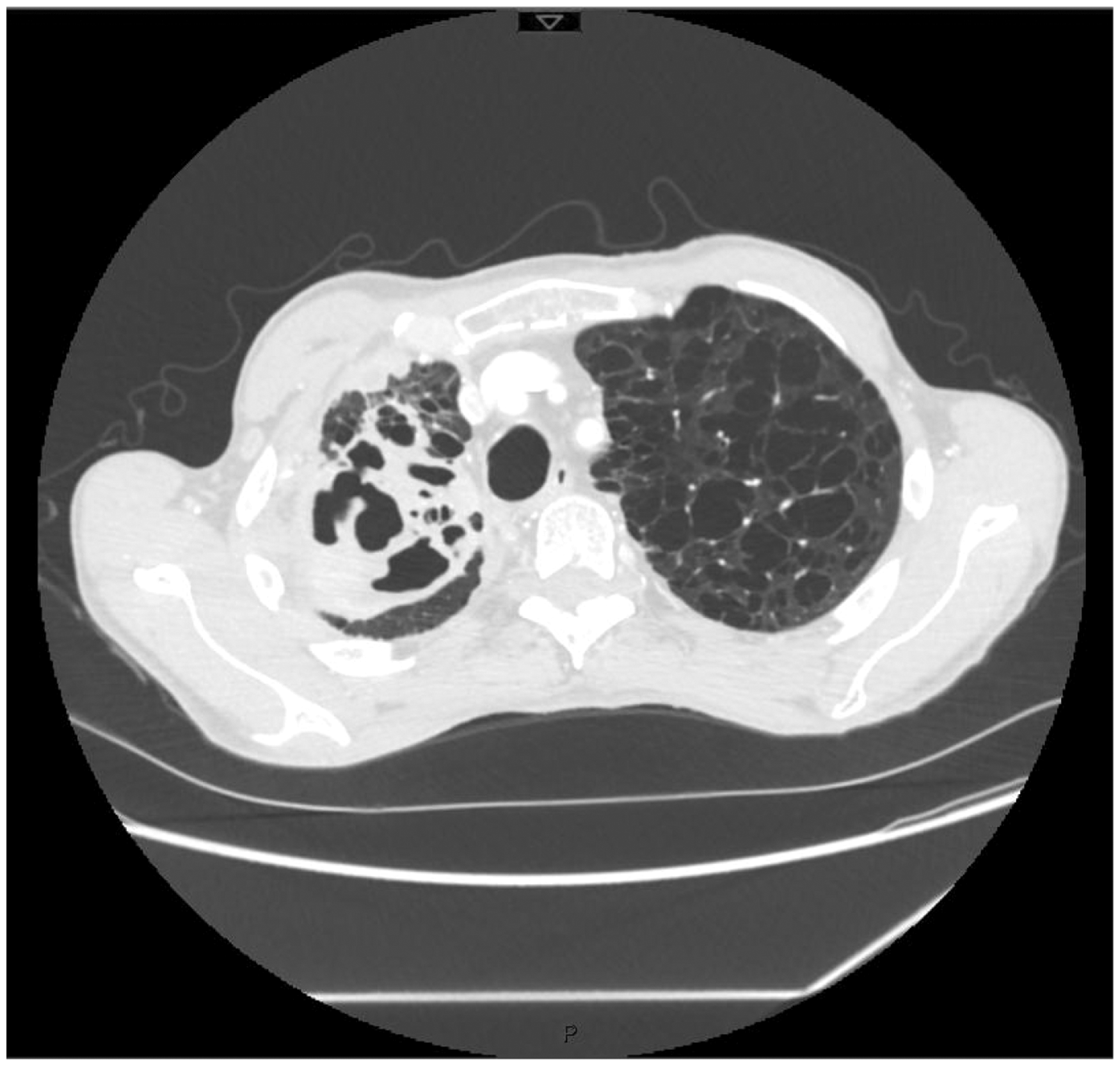
Body mass index was 17.4 kg/m2 and clinical examination was unremarkable. Routine bloods showed an elevated C-reactive protein (83 mg/L) and ESR (69 mm/h). Human immunodeficiency virus test was negative. Spirometry showed mild obstructive ventilatory defect with FEV1 2.1 (80% predicted), VC 3.9L (118% predicted) and an FEV/VC ratio of 53%. A chest radiograph showed extensive right upper lobe consolidation with loss of volume (Figure 1). Chest computed tomography showed a large cavitating right upper lobe lesion (9 × 6 cm), associated with volume loss and extensive lobar bronchiectasis. There was right hilar and paratracheal lymphadenopathy, and background centrilobular emphysema (Figure 2). These findings were suggestive of either atypical infection or malignancy.
Chest X-ray at presentation showing extensive right upper lobe consolidation and volume loss. Initial CT Chest demonstrating a large cavitating right upper lobe lesion (9 × 6 cm) with associated volume loss and extensive lobar bronchiectasis. Background centrilobular emphysema and right hilar and paratracheal lymphadenopathy.
Three sets of sputum cultures were acid-fast bacillus smear positive. Direct IS6110 real-time PCR for Mycobacterium tuberculosis complex was negative, although mycobacterial internal transcribed spacer was detected, consistent with likely NTM infection in this context. Three separate sputum cultures subsequently yielded Mycobacterium marinum. Ciprofloxacin showed poor in vitro activity whereas amikacin, clarithromycin, cotrimoxazole, doxycycline, ethambutol, rifabutin and rifampicin showed good activity against this isolate. Routine bacterial and fungal sputum culture did not identify other pathogens.
On further questioning, the patient described using his mouth to initiate the siphoning of his fish tank and it seemed likely he silently aspirated a small volume of contaminated water, thereby causing pulmonary M. marinum infection. He had given the fish to his daughter eight months previously, but it was suspected that he had developed the infection prior to this, and his presentation had been likely delayed by the insidious nature of his symptoms.
Treatment and outcome
Following initial sputum identification of AFB the patient was commenced on standard anti-tuberculous chemotherapy (rifampicin, isoniazid, pyranzinamide and ethambutol) with prophylactic pyridoxine as an outpatient. Treatment was subsequently altered to rifampicin, ethambutol and clarithromycin following the identification of M. marinum by culture and the availability of the antibiotic sensitivity profile. In addition, he was referred to smoking cessation services.
The patient was seen in the respiratory outpatient clinic 8 to 12 weekly for review, including repeat chest radiography and sputum mycobacteria culture. Initially, his liver function tests showed a mildly elevated γ-glytamyl-transpeptidase, but other liver enzymes were normal; therefore, rifampicin was continued with close monitoring.
Following six months of treatment, his lethargy had improved, but his weight remained unchanged and chest radiograph showed persistent right upper lobe opacification. Sputum was culture negative for M. marinum by this stage. C-reactive protein remained mildly elevated (23 mg/L); therefore, a further six-month course of treatment was advised.
The patient’s weight subsequently improved and he remained clinically stable following a further six months of therapy, completing a one-year course of rifampicin, ethambutol and clarithromycin. Prior to discontinuing treatment, a chest radiograph showed significant improvement with residual right-sided apical fibrotic changes only (Figure 3). Repeat sputum cultures – the first at six months following the initiation of treatment, and subsequently at 9- and 12-months – remained negative, and the patient remained clinically stable 9 months following completion of treatment.
Chest X-ray following completion of treatment showing residual right-sided apical scarring.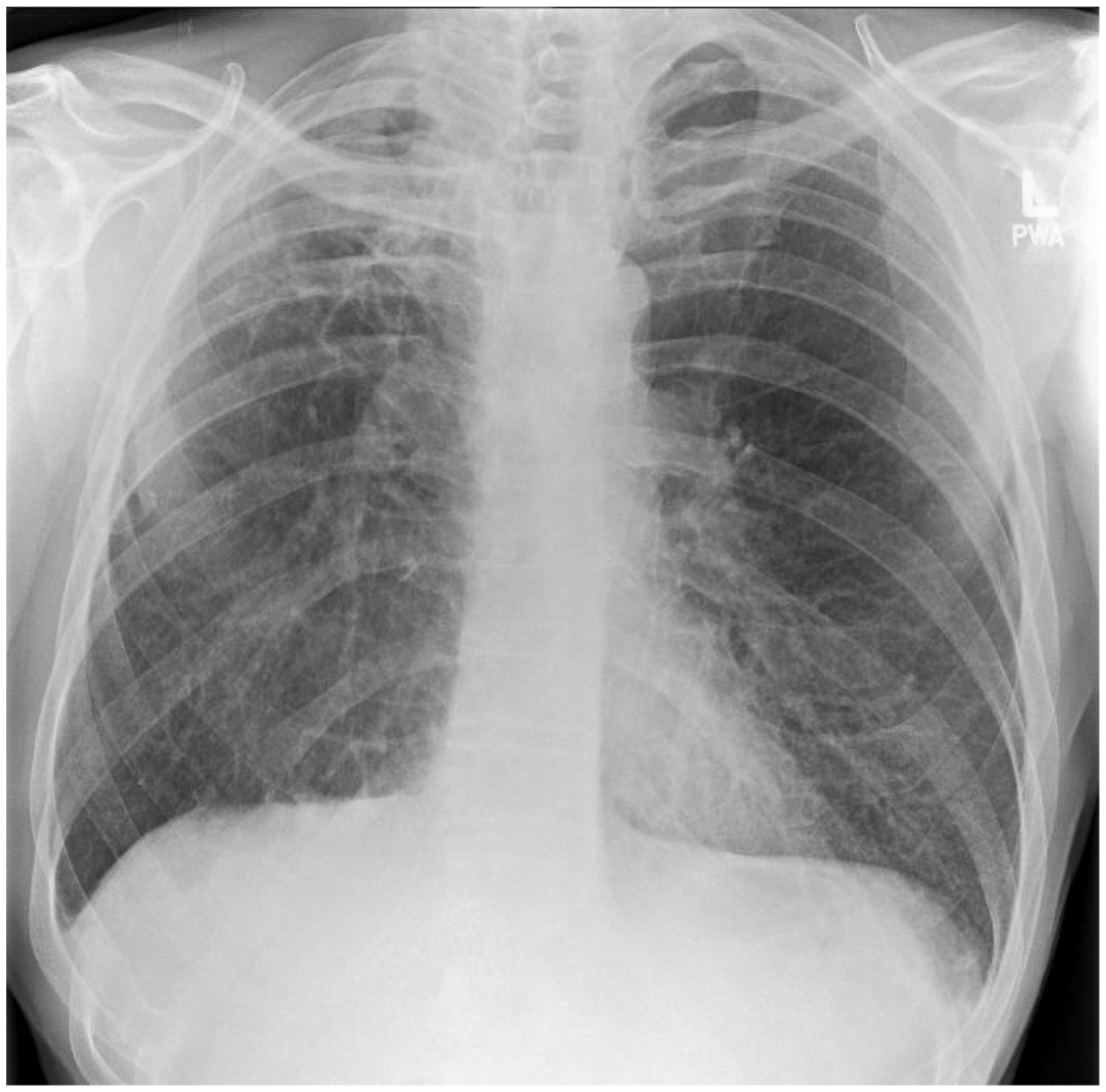
Discussion
M. marinum is a slow-growing non-tuberculous mycobacterium (NTM), commonly found in aquatic environments such as fish tanks or non-chlorinated swimming pools. M. marinum typically manifests as a chronic granulomatous soft tissue infection following minor hand trauma (“fish tank granuloma” or “swimming pool granuloma”), whereas respiratory involvement is very rare. We report only the third documented case of pulmonary infection with M. marinum in an immunocompetent individual.1,2 Interestingly, culture of water from the patient’s fish tank three months following presentation grew Mycobacterium interjectum, another NTM species that is a rare cause of pulmonary infection in immunocompetent individuals. M. marinum itself was not cultured from samples from the patient’s fish tank, but this may have been affected by tank cleaning and a change in the fish in the intervening period. NTM-associated pulmonary infection, which often occurs in patients with pre-existing structural lung disease, is most commonly caused by Mycobacterium avium complex (MAC). 3
The M. tuberculosis (MTB) complex real-time PCR enables rapid confirmation of MTB complex (M. tuberculosis, Mycobacterium bovis, Mycobacterium africanum, Mycobacterium canettii and Mycobacterium microti). This promotes early differentiation of transmissible M. tuberculosis from non-transmissable NTM prior to undertaking large contact-tracing exercises. When used, MTB complex PCR is always undertaken in conjunction with conventional liquid and solid mycobacterial culture, as culture remains more sensitive in untreated patients. Molecular resistance detection is available either directly on specimens or following MTB complex confirmation.
M. marinum infection can be classified into types I to IV based on site and extent of infection to guide subsequent therapy. The case presented can be classified as a type IV infection, indicating pulmonary or systemic manifestations. As M. marinum pulmonary disease has rarely been reported in immunocompetent individuals, there are no consensus management recommendations. We referred to the American Thoracic Society (ATS) guidelines for the treatment of MAC pulmonary disease and M. marinum soft tissue infections to guide antibiotic choice and treatment duration in this case. 4
The ATS guidelines for MAC fibrocavitary pulmonary disease recommend treating with clarithromycin or azithromycin, rifampicin or rifabutin and ethambutol. Treatment should be continued until culture negative on therapy for one year. 4 There are no comparative trials for treatment regimens for M. marinum skin and soft tissue infections; however, treatment with a single agent is often recommended for 6 weeks to 12 months. Treatment with multiple agents for longer periods may be required for deeper-seated infections.5,6
We elected to treat the patient with rifampicin, ethambutol and clarithromycin, for one year in keeping with the aforementioned guidelines. This treatment regimen is consistent with the treatment regimen from an earlier case report of M. marinum-associated pneumonia and pneumothorax in an immunocompetent patient. 2 A second case report detailing a M. marinum-associated pulmonary nodule in an immunocompetent patient was treated successfully with surgical resection and combination therapy with isoniazid, ethambutol and rifampicin. 1 Isoniazid was used to treat superadded Mycobacterium kansasii, which was clinically suspected, but not proven with mycobacterial cultures.
This case report documents a third case of M. marinum pulmonary disease in an immunocompetent patient. It demonstrates evidence of an effective treatment regimen, guided by the existing ATS guidelines for NTM disease and supports previous documented case reports. It additionally highlights the importance of comprehensive history taking in identifying potential sources of infection.
Learning points
M. marinum usually manifests as chronic granulomatous soft tissue infection and very rarely causes pulmonary disease. This case report supports the use of rifampicin, ethambutol and clarithromycin in the treatment of M. marinum pulmonary disease. A detailed history can identify potential sources of non-tuberculous mycobacterial infection, in this case siphoning fish tank water.
Authors’ contribution
Prasad Palani Velu and Susan E. Fernandes were responsible for the acquisition of relevant information, authorship of the manuscript and preparation for submission. Ian F. Laurenson revised the manuscript for intellectually appropriate content and approved the version to be submitted for publication. Donald D. Noble obtained patient consent, revise the manuscript for intellectually appropriate content and approved the version to be submitted for publication.
Patient consent
Written informed consent was obtained from the patient for the publication of information relevant to the case and for the publication of anonymised imaging.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.