Presenting symptoms and long-term survival in head and neck cancer
CM Douglas1, K Ingarfield2, AD McMahon2, SA Savage3, DI Conway2 and K MacKenzie4
1Department of Otolaryngology – Head and Neck Surgery, Queen Elizabeth University Hospital, UK
2Community Oral Health Department, Dental School, University of Glasgow, UK
3Victoria Hospital, UK
4Department of Otolaryngology – Head and Neck Surgery, Glasgow Royal Infirmary, UK
Abstract
Objectives: To assess how type and number of symptoms are related to survival in head and neck cancer patients.
Design: Patients were followed up for over 10 years from the Scottish Audit of Head and Neck Cancer; (national cohort of head and neck cancer patients in Scotland 1999–2001). September 2013, cohort was linked to national mortality data. First, second and third presenting symptoms were recorded at diagnosis.
Setting: National prospective audit – Scotland.
Participants: A subset of 1589 patients, from the original cohort of 1895, who had cancer arising from one of the four main subsites; larynx, oropharynx, oral cavity and hypopharynx.
Main outcome measures: Median survival in relation to patients’ presenting symptoms.
Results: A total of 1146 (72%) males and 443 (28%) females, mean age at diagnosis 64 years (13–95). There was a significant difference in survival in relation to the number of the patient’s presenting symptoms; one symptom had a median survival of 5.3 years compared with 1.1 years for three symptoms. Patients who presented with weight loss had a median survival of 0.8 years, compared to 4.2 years if they did not (P < 0.001). Patients who presented with hoarseness had a median survival of 5.9 years compared to 2.6 years without (P < 0.001). There was no significant difference in long-term survival for patients who presented with an ulcer, compared to those who did not (P = 0.105).
Conclusions: This study highlights the importance of patients’ presenting symptoms, giving valuable information in highlighting appropriate ‘red flag’ symptoms and subsequent treatment planning and prognosis.
Oral Presentation 2
What is the association of evidence of problem drug use (via opiate replacement therapy prescribing) on health service engagement and clinical outcomes in patients with diabetes?
H Druce1, R Lowrie2, C Ritchie3, D Morrison1, CAR Sainsbury1 and GC Jones1
1Department of Diabetes and Endocrinology, Gartnavel General Hospital, UK
2Pharmacy and Prescribing Support Unit, West Glasgow ACH, UK
3NHS GGC Addictions Services, UK
Abstract
Background: People with problem drug use are thought to engage less with health services. Diabetes is a common co-morbidity conferring poorer outcomes. We hypothesised that people with diabetes and problem drug use engage less with services and have worse outcomes.
Methods: All adults using opiate replacement therapy (ORT) also in national diabetes database (SCI-diabetes) were included (2011–2016). An age, gender and diabetes duration matched case-control cohort was identified from SCI-diabetes without ORT use, and comparative analysis performed.
Results: A total of 393 people (age 41.0 (35.9–46.1)) on ORT and matched cohort were included. Haemoglobin A1c (HbA1c) levels showed no significant difference (P = 0.47) but number of HbA1c measures/year were lower in the ORT cohort (1.2 (0.4–2.0), 1.6 (0.8–2.5), P < 0.001). Proportion of appointments not attended/year was higher in the ORT cohort compared to matched cohort for diabetes clinics (median (interquartile range) 0.53 (0.33–0.83), 0.17 (0–0.5), P < 0.001) and retinopathy screening (0.33 (0–0.8), 0 (0–0.2), P < 0.001). Unscheduled hospital attendance rate/year was higher in the ORT cohort (0.6 (0–1.64), 0 (0–0.52), P = < 0.001). Five-year all-cause mortality was increased in ORT cohort (hazard ratio = 5.14, P < 0.001).
Conclusion: People with diabetes and problem drug use engage less with scheduled diabetes services and have more unscheduled care attendances. Mortality in this group is much higher than in patients with diabetes alone. In the context of an aging population and the contribution of chronic medical conditions to the recent increase in drug-related deaths, this cohort presents a potential target for enhanced case management facilitated through their regular attendance at ORT prescribing clinics.
Oral Presentation 3
Antithrombotic medications in upper gastrointestinal bleeding: frequency of use, timing of re-prescription & outcomes
K Bee1, K Sim1, J Adams1, J Tan1, M. Rahman1, AJ Morris and AJ Stanley2
1Medical students, University of Glasgow, UK
2GI Unit, Glasgow Royal Infirmary, UK
Abstract
Background: Upper gastrointestinal bleeding (UGIB) is a common medical emergency.1 The use of antithrombotic (AT) medications (anti-platelets or anti-coagulants/direct oral anticoagulants (DOACs)) is increasing. These drugs significantly increase the risk of UGIB.2 Our aim was to assess the use of AT medications and non-steroidal anti-inflammatory drugs (NSAIDs) on outcome after UGIB and the timing of re-prescription of these drugs.
Methods: A six-month audit (01 April 2016–30 September 2016) of patients undergoing endoscopy for UGIB was conducted. Demographics, drug use and Full Rockall risk score (FRS) were calculated. Outcomes included transfusion, endoscopic therapy, re-bleeding <7 days and 30-day mortality. We assessed prescription of ATs and NSAIDs following presentation.
Results: A total of 206 patients were identified, 48% were taking AT drugs or NSAIDs. Patients taking ATs were older (69 vs. 53 years; P < 0.001) and had higher FRS (+32.0%, P < 0.001) than those not. Peptic ulcers were more common (38% vs. 22%; P = 0.02) and varices less common (4% vs. 15%; P < 0.02) in patients on ATs vs. those not. Need for transfusion (29% vs. 27%) and need for endoscopic therapy (45% vs. 55%) were similar in both groups. Aspirin and adenosine diphosphate inhibitors were restarted <3 days in 57% and 40%, respectively; 71.4% and 60%, respectively, had these drug restarted <7 days and 17% and 13%, respectively, had them permanently discontinued. NSAIDs were permanently discontinued in 91%. All six patients on DOACs had the drug restarted <3 days. Comparing those on ATs vs. those not on ATs, there was no difference in re-bleeding (4.11% vs. 6.67%; P = 0.501) or mortality (10.9% vs. 7.07%; P = 0.447).
Conclusions: Use of AT drugs is common in patients presenting with UGIB. Most patients are restarted on these medications <3 days of their bleed. Despite patients on ATs being older and with higher FRS, outcomes after UGIB, including re-bleeding and survival, are similar for patients taking or not taking AT medications.
References
Scottish Intercollegiate Guidelines Network. SIGN 105: Management of acute upper and lower gastrointestinal bleeding. SIGN; 2008.LanasAet al.Low doses of acetylsalicylic acid increase risk of GI bleeding in a meta-analysis. Clin Gastro Hepatol2011; 9: 762–768.GralnekIet al.Diagnosis and management of nonvariceal upper gastrointestinal hemorrhage: European Society of Gastrointestinal Endoscopy (ESGE) Guideline. Endoscopy2015; 47: a1–a46.
Oral Presentation 4
The effect of T-regulatory lymphocytes on patient survival following neoadjuvent chemotherapy for oesophageal adenocarcinoma
A McLaren1, B Stewart2 and P Glen3
1University of Glasgow, UK
2Glasgow Royal Infirmary, UK
3Queen Elizabeth University Hospital, UK
Abstract
Background: Oesophageal cancer carries a poor survival of 12.3% at five years. Its predominant histological subtype in the Western world, oesophageal adenocarcinoma, is increasing in incidence. The influence that the host inflammatory response has on tumour progression and ultimately patient survival is being increasingly understood. Previously, it has been found that the Klintrup-Makinen criteria can be used to grade the overall local inflammatory response in oesophageal adenocarcinoma to stratify patients into prognostic groups. Detailed assessment of the cellular components of the local inflammatory infiltrate may provide insight into the driving force of its prognostic value. In this study, we aim to investigate the prognostic effect of FOXP3+ T-regulatory lymphocyte infiltration in a homogenous cohort of patients with oesophageal adenocarcinoma treated with neoadjuvent chemotherapy and surgical resection.
Methods: Included in the study were patients with oesophageal adenocarcinoma who were treated with neoadjuvent chemotherapy and surgical resection with curative intent. Immunohistochemistry was used to assess FOXP3+ T-regulatory lymphocyte infiltration.
Results: Tissue was available for 72 patients for analysis. The median survival for FOXP3+low patients was 29.8 (95% confidence interval (CI) 11.4–48.2) months versus 22.3 (95% CI 16.1–28.5) months for FOXP3+high patients (P = 0.096). Lower FOXP3+ infiltrate was significantly associated with higher Klintrup-Makinen score (P = 0.003).
Conclusion: The present study demonstrates that FOXP3+ T-regulatory lymphocyte infiltrate does not predict survival in a homogenous cohort of patients with oesophageal adenocarcinoma treated with neoadjuvent chemotherapy and surgical resection with curative intent. However, it does demonstrate a significant negative association between FOXP3+ T-regulatory lymphocyte infiltrate and Klintrup-Makinen score.
Oral Presentation 5 (winner best oral platform)
Validating and comparing stroke prognosis scales
Sarjit Singh1, Terence J Quinn2, Philip M Bath3, Kennedy R Lees2 and Phyo K Myint4
1Undergraduate Medical School, University of Glasgow, UK
2Institute of Cardiovascular and Medical Sciences, University of Glasgow, UK
3Division of Clinical Neuroscience, Stroke Trials Unit, University of Nottingham, UK
4School of Medicine, Medical Sciences and Nutrition, University of Aberdeen, UK
Abstract
Objective: An array of scales purport to predict longer-term stroke prognosis using baseline data, although to date there have been few direct comparisons of prognostic scales and few external validations. We set out to compare the prognostic accuracy of various acute stroke prognostic scales using a large, independent dataset.
Methods: We directly compared eight stroke prognostic scales, chosen based on focussed literature review (ASTRAL, iSCORE, iSCORE-revised, PLAN, SOAR, SOAR-modified, SPI2 and THRIVE) using individual patient level data from a clinical trials archive (VISTA). We calculated area under receiver-operating characteristic curves (AUROCs) for each scale against 90-day outcomes of: modified Rankin Scale (dichotomized at mRS > 2); Barthel Index (BI > 85) and mortality. We performed two complementary analyses: the first limited to subjects with complete data for all components of all scales (simultaneous) and the second used as many subjects as possible for each individual scale (separate).We compared AUROCs and performed sensitivity analyses substituting extreme outcome values for missing data.
Results: In total, 10,777 subjects contributed to the analyses. Our simultaneous analyses suggested ASTRAL had greatest prognostic accuracy for mRS, AUROC: 0.78 (95% CI: 0.75–0.82) and SPI2 had poorest AUROC: 0.61 (95% CI: 0.57–0.66). Our separate analyses confirmed these results, ASTRAL AUROC: 0.79 (95% CI: 0.78–0.80 and SPI2 AUROC: 0.60 (95% CI: 0.59–0.61). There was a significant difference in mRS AUROC between ASTRAL and all other scales. Sensitivity analysis identified no evidence of systematic bias from missing data.
Conclusions: Comparative analyses confirm differences in the prognostic accuracy of stroke scales. However, even the best performing scale had prognostic accuracy that may not be sufficient as a basis for clinical decision making.
Acknowledgements
We thank Myzoon Ali (University of Glasgow) for assistance with obtaining dataset access.
Poster 1
Should we ScRAP SIGN 117?
CM Douglas and LJ Clark
1ENT Registrar, Department of Otolaryngology – Head and Neck Surgery, Queen Elizabeth University Hospital, UK
2ENT Consultant, Department of Otolaryngology – Head and Neck Surgery, Queen Elizabeth University Hospital, UK
Abstract
Introduction: Tonsillitis represents a significant burden on the health service. Recurrent tonsillitis fulfilling the Scottish Intercollegiate Guidelines Network guidelines is treated with tonsillectomy. The McKinsay report has suggested that £700 m could be saved if procedures with ‘limited clinical benefit’ – such as tonsillectomies, were stopped. We carried out a retrospective review of hospital admissions with ‘sore throat’ in the context of number of tonsillectomies being performed.
Methods: Information Services Division Scotland data were requested for rates of tonsillectomy, tonsillitis admission, peritonsillar abscess admissions and deep neck space infection (DNSI) admissions in Scotland, between 1993 and 2015. Data for prescriptions for penicillin were also requested for general practice and hospital admissions 2011–2016.
Results: Between 1993 and 2015, there has been a 48% decrease in tonsillectomy rates. There has been a corresponding 143% increase in tonsillitis admission rates over this same time period (P = 0.006, r2 = 0.85983) and a 116% increase in peritonsillar abscess admissions (r = –0.668, r2 = 0.45631, P < 0.001). Between 1996 and 2015, there has been a 306% increase in deep neck space abscesses (r = –0.483, r2 = 0.79926, P = 0.036). The defined daily doses for penicillin antibiotics in primary and secondary care between 2010 and 2016 show a significant correlation (r2 = 0.98).
Discussion: The significant decrease in tonsillectomy rates has correlated with a significant rise in ‘sore throat’ admissions to the hospital. The most alarming trend is the increase in DNSI rates, a condition associated with significant morbidity and mortality. A decrease in primary care prescribing has correlated with an increase in secondary care prescribing.
Poster 2
Patterns of hospital admission in 54,140 patients with epistaxis over a 21-year period in Scotland
T Tikka, B Broadbent, CM Douglas and J Montgomery
Queen Elizabeth University Hospital, UK
Abstract
Background: Epistaxis affects most people over their lifetime. It is the commonest ear, nose and throat emergency. Socioeconomic deprivation has been associated with mental health disorders, respiratory illness and with emergency hospital admissions. Low socioeconomic status has never previously been associated with epistaxis, a common reason for admission to ear, nose and throat departments throughout the UK.
Methods: Demographics from Information Services Division Scotland were analysed from 1995 to 2015. This focused on gender, number of admissions, number of bed days and socioeconomic deprivation (Scottish Index of Multiple Deprivation).
Results: Data from 54,140 patients were assessed. Males are more frequently affected. Admission numbers have remained stable but a significant reduction in bed days was found (P < 0.0001). This reflects an average reduction in the duration of inpatient stay by one day per patient. Social deprivation was linked with a higher number of hospital admissions (P < 0.001; Figure 1).
Conclusions: In comparison to other areas of the United Kingdom, Scotland has shown a reduction of days spent in hospital for epistaxis. Socioeconomic deprivation had a causal effect on number of admissions.
Poster 3
Deep neck space infection: assessing the hidden cost of a serious condition
RH Hurley, CM Douglas, J Montgomery and L Clark
Ear, Nose and Throat Department, Queen Elizabeth University Hospital, UK
Abstract
Background: The incidence of deep neck space infection (DNSI) is rising, this appears to be related to falling rates of tonsillectomy.1,2 These conditions have devastating complications including airway compromise, mediastinitis, internal jugular vein thrombosis and death. The purpose of this study was to assess demographics of patients presenting with DNSI and the financial burden to the National Health Service (NHS).
Mean number of epistaxis admissions per SIMD. SMID: Scottish Index of Multiple Deprivation.
Methods: Retrospective data collection of patients admitted to NHS Greater Glasgow and Clyde with DNSI between January 2012 and November 2016. Demographics, aetiology and use of hospital resources were reviewed. Cost of hospital admissions were calculated using data from the Scottish Government’s Information Services Division, the local diagnostics division and the British National Formulary.
Results: Seventy-four patients were admitted with DNSI. The median age was 43.98 (16–86). Forty patients were male (54%). The most frequent source of infection was the tonsil (n = 30, 40.5%). The most common infective organism was Streptococcus constellatum in nine patients (12.2%). Mean length of stay was 12 days. Fifty-five (74.3%) patients required operative intervention. The mean cost of admission was £5688.41 (£299.06–£46,577.00).
Conclusion: This study highlights that DNSI is a significant financial burden to the NHS. As the incidence of DNSI continues to rise, there will be a subsequent increase in cost to the NHS, which must be planned for.
References
LauASUpileNSWilkieMDet al.The rising rate of admissions for tonsillitis and neck space abscesses in England, 1991-2011. Ann R Coll Surg Engl2014; 96: 307–310.YapDHarrisASClarkeJ. Serious tonsil infections versus tonsillectomy rates in Wales: a 15-year analysis. Ann R Coll Surg Engl2017; 99: 31–36.
Poster 4
Magnetic resonance imaging/ultrasound fusion biopsies improve rates of prostate cancer diagnosis: a direct comparison of fusion and standard transrectal ultrasound biopsies in the same population
E Day, MJ Rewhorn, M Gurun, R Meddings, G McLaughlin, D Chanock and R Clark
Ayr University Hospital, UK
Abstract
Background: Prostate cancer has a varied prognosis and requires careful diagnosis and risk stratification to avoid over-investigation or treatment. Magnetic resonance imaging (MRI) fusion biopsies can increase the detection of clinically relevant prostate cancer compared to standard transrectal ultrasound (TRUS)-guided biopsies. Here, we report on the optimisation of the technique in the routine diagnosis of prostate cancer for the first time in a Scottish Hospital. Importantly, we are able to include patients who had recent standard TRUS biopsies as a direct comparison of techniques.
Methods: Patients requiring prostate biopsy at Ayr University Hospital from 2014 to 2016 (n = 227). Fusion biopsies were performed using Artemis (Eigen, USA) by two consultant urologists in a day surgery setting. Standard systematic biopsies were also taken contemporaneously. A total of 90 patients also had recent standard TRUS biopsies.
Results: Fusion biopsy revealed malignancy in 156 (69%) cases. Of these, 60% were intermediate or high-risk cancers (D’Amico Classification). In all bar two cases, the targeted, compared to systematic, biopsy returned the highest grade. Of the 59 patients with previous benign standard TRUS results, 32 (52%) had malignant histology on targeted biopsies. Overall complication rates were low: systemic infection 4%, procedure not tolerated 0.4% and no cases of urinary retention.
Conclusions: MRI/ultrasound fusion biopsies more sensitively detect prostate cancer compared to standard TRUS biopsies, enabling appropriate risk stratification and avoiding repeat biopsy. Our data have shown that the implementation of fusion biopsy is feasible and improves the diagnostic algorithm for prostate cancer.
Poster 5
Initial assessment and management of acute renal colic: a retrospective audit of practice
F Rodger and O Aboumarzouk
Queen Elizabeth University Hospital, UK
Abstract
Background: Acute renal colic is a common presentation to the acute services. The European Urology Association has made recommendations for the investigation and initial management of these patients. Key investigations can help identify patients requiring intervention from those who can be managed conservatively. Additionally, initial management can reduce pain and avert the need for surgical intervention in some cases. We aimed to audit the initial assessment of patients presenting acutely with urolithiasis to the QEUH in line with the EUA guidelines (2015).
Methods: Patients with ureteric stones on CTKUB were identified via PACs. Fifty patients who presented to A + E or surgical receiving with symptomatic renal colic were identified from this group. Retrospective portal review was then carried out.
Results: All (100%) patients had baseline renal function and blood count checked and 98% had a CRP checked. Only 56% and 12% patients had calcium and urate level checked, respectively. Urinalysis was not recorded in 10% cases and 72% received non-steroidal anti-inflammatory drugs. Opioids were given in 62% and paracetamol was given in 88%. Medical expulsive therapy was given in 30%. X-ray KUB was carried out in 16% of cases.
Conclusions: We have identified short comings in key areas of initial renal colic assessment and management. In light of these findings, we present a local protocol for the assessment of acute renal colic in line with EUA guidelines. This will be disseminated to staff in A + E and surgical receiving. Following this, a re-audit will be carried out in June 2017.
Poster 6
Guess the weight: the accuracy of ‘guessimated’ weight (winner best poster – surgical)
JA Empry, RAB Thomas, S Seth and J Crozier
Doctor in Training, Forth Valley Royal Hospital, UK
Abstract
Background: Actual body weight (ABW) is used for many drug calculations and accuracy is paramount for safe dosing. ABW is often unavailable for emergency admissions and estimation is used instead. Research from A&E found healthcare professionals (HCPs) were poor at estimating weights but no data exist for surgical admissions.1 Our group assessed the reliability of weight estimation by surgical patients and HCPs. We also identified which group was most accurate and the factors affecting accuracy.
Methods: All emergency surgical patients admitted during a week in March 2015 were approached. If they consented, four HCPs (Consultant, Foundation Doctors, Nurse and Healthcare Assistant) independently estimated their weight. Then, the patients gave their own estimate. Actual height and weight were then recorded. Data were analysed using SPSS.
Results: A total of 73 consecutive surgical admissions were included. HCPs correctly (within ±10% margin) estimated a patient’s weight in only 57% of cases. Foundation Doctors performed worst (54%) and Consultants best (60%). Patients were considerably more accurate at 77%. Across all groups, accuracy declined when body mass index >35.
Conclusions: Staff are poor at estimating weight, but experience and similar body habitus improved performance. Patients are the most accurate estimators of their own weight but still not reliable enough. Importantly, even when estimated weight was within our predetermined ‘accuracy window’, there remains a significant risk of under or overdosing. Inaccurate weight also impacts on the safety of staff transferring patients and equipment use. Obese patients are particularly vulnerable to inaccurate guessimation. As a result of this research, our hospital plans to fund extra, accessible weighing machines.
Reference
1. Anglemeyer BL, et al. The accuracy of visual estimation of body weight in ED. Am J Emerg Med 2004; 22: 526–529.
Poster 7
Compliance to National Institute for Clinical Excellence guidelines of intravenous fluid therapy prescription in general surgery emergency admissions
S Robinson1, CL Gelder2 and A McMahon2
1Medical Student, University of Glasgow, UK
2Doctor in Training, Glasgow Royal Infirmary, UK
Abstract
Background: Audit to determine whether intravenous fluid (IV) therapy in general surgical emergency admissions adheres to National Institute for Clinical Excellence (NICE) guidelines.1 IV fluid therapy requires regular monitoring and is indicated for patients’ whose needs cannot be met by oral or enteral routes. We audited the reasons for IV fluid prescription and related complications.
Methods: A total of 77 patients’ data (30 male and 47 female) were obtained from a single general surgeons’ emergency admission list. Of the 77 patients, 62% received IV fluids. Data were collected over the patients’ first three days in hospital: fluid intake and output; reason for IV fluids; complications relating to IV fluids; relevant biochemistry and patient presentation. We assessed their fluid requirement by the correlation of clinical data with NICE IV fluid therapy guidelines.1
Results: Over the three days, 15% of fluid prescriptions adhered to NICE guidelines1 with 63% non-compliant. We were unable to assess compliance in a further 22% as no oral intake was documented. Incomplete fluid or fluid balance charts were noted for 27% of patients, with 31% having no fluid balance charts and 12% noted as receiving fluids but did not have a fluid prescription chart. The main reasons patients’ received IV fluids were due to fasting while awaiting scans (37.5%) or admission with nausea and vomiting (35%). Complications relating to IV fluids included hyperchloraemia (29%), hypouraemia (27%) and hypokalaemia (10%).
Conclusion: These findings indicate that further education on IV fluid prescription and its complications is needed alongside improvement in chart adherence. This audit will be reordered within three to six months.
Reference
1. National Institute for Clinical Excellence. Intravenous fluid therapy in adults in hospital. Clinical Guideline 32, London: NICE, 2013.
Poster 8
The relationship between 18-fluorodeoxyglucose positron emission tomography–computed tomography derived markers of tumour metabolism and systemic inflammation in patients undergoing surgery for colorectal cancer
BY Khor1, ST McSorley1, D Colville2, S Han2, PG Horgan1 and DC McMillan1
1Academic Unit of Surgery, School of Medicine, University of Glasgow, Glasgow Royal Infirmary, UK
2West of Scotland 18FDG-PETCT Centre, Gartnavel General Hospital, UK
Abstract
Aims: The aim of the present study was to investigate the relationship between 18-fluorodeoxyglucose positron emission tomography–computed tomography (18F FDG-PETCT) derived markers of tumour metabolism and systemic inflammation in patients undergoing surgery for colorectal cancer.
Methods: Patients with colorectal cancer, who underwent potentially curative surgery between 2008 and 2015, and 18F FDG-PETCT during their treatment at a single centre were included in the study (n = 103). Modified Glasgow Prognostic Score (mGPS) and neutrophil–lymphocyte ratio (NLR) were derived from routine blood samples. Maximum standardised uptake (SUVmax), peak standardised uptake (SUVpeak), metabolic tumour volume (MTV) and total lesion glycolysis (TLG) were measured.
Results: Of the 103 patients, majority (55%) were male, over 65 (57%) and with node negative disease (51%). Thirty-three (32%) of the patients underwent 18F FDG-PETCT preoperatively, whereas 70 (68%) underwent follow-up 18F FDG-PETCT. Primary lesions, compared to secondary lesions, were associated with a significantly higher SUVmax (17 vs. 7, P < 0.001), SUVpeak (10 vs. 5, P < 0.001), MTV (8 vs. 2 mL, P = 0.001) and TLG (90 vs. 10 g, P < 0.001). Of those who underwent 18F FDG-PETCT as follow-up, patients with NLR ≥ 5 had a significantly higher SUVmax (20 vs. 7, P = 0.002), SUVpeak (14 vs. 5, P < 0.001), MTV (29 vs. 2 g, P = 0.001) and TLG (338 vs. 9 g, P < 0.001). Similarly, patients with mGPS of 1–2 had a significantly higher SUVmax (11 vs. 6, P = 0.048), SUVpeak (8 vs. 4, P = 0.046), MTV (13 vs. 2 mL, P = 0.005) and TLG (146 vs. 10 g, P = 0.004).
Conclusion: The present study shows a direct association between 18F FDG-PETCT derived measures of tumour metabolism and systemic inflammation in patients with recurrent colorectal cancer.
Poster 9
Alcohol bed days at a District General Hospital in Scotland: role of alcohol and alcohol liaison services
A Cutts
Inverclyde Royal Hospital, UK
Abstract
Background: Catchment area for Inverclyde Royal Hospital (IRH) has a large population affected by the use of alcohol. Objective of this study was to look at the total number of bed days as a sequela of alcohol.
Methods: Retrospective data collection using described presentations on acute admission lists and digitalised medical notes to quantify alcohol-related admissions to medicine. These were then collated and analysed using Excel. This included total bed days and total alcohol units consumed per week. Also categorised according to reviews by alcohol liaison services and if follow-up was arranged prior to discharge with alcohol services.
Results: Total of 164 admissions over four months related to alcohol. Average number of bed days was eight (range 1–10), average number of units consumed per week was 128.5. Of these, 93 were not seen by alcohol liaison services, despite 70 still drinking alcohol. The most common admission category was alcohol withdrawal with 70 admissions during the four-month period recording an average stay of 8.6 days and an average number of units consumed of 175 per week.
Conclusions: Alcohol-related admissions make up a large number of acute medical admissions to IRH. This comes at significant cost in number of bed days and clinician hours. Both National Institute for Clinical Excellence and Scottish Intercollegiate Guidelines Network guidelines recommend seven-day specialist alcohol service availability to reduce length of inpatient stays and prevent ongoing harm.
Poster 10
Weaning of non-invasive ventilation in patients with chronic obstructive pulmonary disease and acute hypercapnic respiratory failure
C Turner, E Nugent, P O’Mailley, H Bayes and E Livingston
Department of Respiratory Medicine, Glasgow Royal Infirmary, UK
Abstract
Background: Acute non-invasive ventilation (NIV) is a common evidence-based intervention for patients with chronic obstructive pulmonary disease (COPD) in acute hypercapnic respiratory failure. Following clinical stabilization, the British Thoracic Society (BTS) recommends gradual weaning of NIV over two to three days, although data are lacking as to whether this is beneficial. We undertook a complete audit cycle of our clinical practice, with a gradual weaning schedule added to our NIV proforma between audits.
Methods: Retrospective case note analysis of COPD patients started on NIV for acute hypercapnic acidosis in January to February 2015 (audit 1) and December 2016 to February 2017 (audit 2). Between audits, a gradual weaning schedule was added to the NIV proforma used on all respiratory wards at Glasgow Royal Infirmary.
Results: Audit 1 and 2 included 17 and 22 patients, respectively. All patients met the BTS criteria for acute NIV use. The patients demonstrated several features of severe COPD: 27% had long-term home oxygen, 64% home nebulisers and median FEV1 was 36.5% (interquartile range: 27.3%–45.0%). In audit 1, 25% (2/8 suitable patients) were gradually weaned from NIV compared with 67% in audit 2 (8/12) – a 42% increase in appropriate weaning. Overall, 20% (2/10) of those gradually weaned developed respiratory acidosis and subsequent unscheduled return to NIV during the same admission, compared with 80% (8/10) who had NIV abruptly discontinued (P = 0.023).
Conclusion: Introduction of a NIV weaning proforma significantly increased appropriate gradual weaning from acute NIV. Importantly, gradual weaning significantly reduces later deterioration with respiratory acidosis and unscheduled return to NIV.
Poster 11
Association between C-peptide, insulin therapy and all cause mortality: a retrospective cohort study of 872 patients with diabetes
EL Leighton1, K Smith2, SG Cunningham3, CAR Sainsbury1 and GC Jones1
1Department of Diabetes and Endocrinology, Gartnavel General Hospital, UK
2Department of Biochemistry, Glasgow Royal Infirmary, UK
3Clinical Technology Centre, Ninewells Hospital, UK
Abstract
Background: C-peptide is a frequently used measure of insulin secretion. We investigated the association between C-peptide and progression to insulin therapy and mortality in patients with diabetes.
Methods: A total of 1971 patients with C-peptide measurements (February 2007—December 2016) were identified within a single health board area. Total of 872 individuals with a diabetes diagnosis were taken forward to analysis. The date of the first encashed insulin prescription and date of death for each individual were extracted from the national diabetes dataset. All data were analysed with first C-peptide in dataset, age and body mass index (BMI) as covariables. Insulin-free survival (time to first insulin prescription or end of follow-up) was investigated using survival analysis (cox proportional hazard model). Mortality at three years was investigated using logistic regression.
Results: Three hundred and thirteen individuals had BMI data and were insulin-naive at the time of C-peptide measurement. C-peptide in the lower half of the range of observed values (<0.615 nmol/L) is associated with a significantly decreased time to insulin administration and a higher rate of insulin prescription at one year (hazard ratio for insulin requirement 2.0, P < 0.001). Increasing C-peptide concentration is associated with increased mortality at three years independent of age and BMI (n = 464, P = 0.02, estimate 0.42).
Conclusion: C-peptide below the median value for the cohort was associated with a reduced time to insulin prescription and an increased probability of requiring insulin at one year and independently associated with mortality at three years when age and BMI are taken as covariables.
Poster 12
Radioactive iodine therapy in thyrotoxicosis: appropriate dose and predictors of treatment failure
R Mauchlen, L Hogg, C Smith, N McGowan, C Harrow and M McIntyre
Royal Alexandra Hospital, UK
Abstract
Background: I-131 has been a safe and successful treatment for thyrotoxicosis for many decades. It is taken up by the iodide transporter and destroys the follicular cells, thus decreasing the size and function of the gland. However, there is ongoing discussion about the most appropriate dose to use. Higher doses require more prolonged ‘isolation’ and lower doses risk therapy failure, possibly repeat dosing and continued risk of complications. This issue is confounded by the fact that the patient would need to wait at least a year for repeat dosing.
Methods: We carried out a retrospective analysis of patients treated with 400 MBq of I-131 for thyrotoxicosis over a three-year period at the Royal Alexandra Hospital. We used TrakCare to obtain data on their diagnosis (Graves’ disease or toxic nodular goire) and thyroid function tests before and after treatment. Data were obtained on 57 consecutive I-131 treated patients (F 43: M 14).
Results: By the third follow-up appointment, 12 patients were still thyrotoxic. Predictors of I-131 treatment failure were: being male (36.3%) vs. female (25.0%) P < 0.01; having a toxic nodular goitre (33.3%) vs. Graves’ disease (16.0%) P < 0.01 and pre-treatment thyroid-stimulating hormone low (28.6%) vs. normal/high (22.2%) P < 0.01.
Conclusions: The high rate of treatment failure suggests that it would be beneficial to increase the dosage. Patients with risk factors for treatment failure would particularly benefit from an increased dose.
Poster 13 (Winner best poster – medical)
Socioeconomic status is associated with place of death in patients known to hospice services
Sarah Bowers1, Maire O’Riordan2, Mike MacFarlane2 and Emma Carduff2
1Queen Elizabeth Hospital, UK
2Marie Curie Hospice, UK
Abstract
Background: Although 58% of Scottish deaths in 2015 occurred in hospital, most patients would prefer to die at home. This study described the relationship between place of death and socioeconomic status for patients known to a hospice over five years.
Method: Scottish Index of Multiple Deprivation (SIMD) was used to group patients according to socioeconomic status. Place of death was examined for each deprivation quintile. Deaths where location was unknown or in a nursing home were excluded.
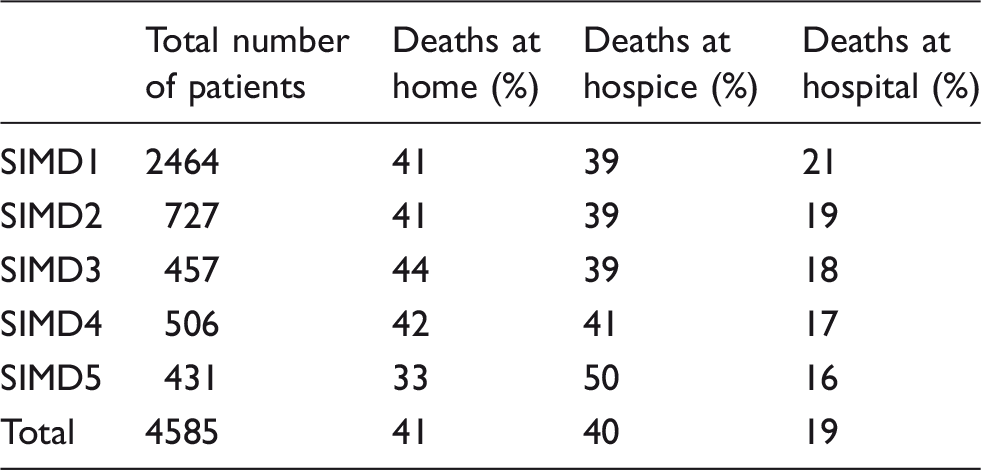
Results: Of 4585 patient deaths, 41% died at home, 40% in the hospice and 19% in hospital (Table 1). Over half of the patients (54%) were from SIMD1 (most deprived). Deaths at home were lower in the most affluent group. There was a highly significant direct relationship between DQ and proportion of patients dying in the hospice. There was an inverse correlation between DQ and the proportion dying in hospital (P = 0.0002, Chi-squared test for trend).
Total number of patients
Deaths at home (%)
Deaths at hospice (%)
Deaths at hospital (%)
SIMD1
2464
41
39
21
SIMD2
727
41
39
19
SIMD3
457
44
39
18
SIMD4
506
42
41
17
SIMD5
431
33
50
16
Total
4585
41
40
19
SIMD: Scottish Index of Multiple Deprivation.
Conclusion: Overall, this study demonstrates that patients from more deprived areas, known to hospice, are more likely to die in hospital than their more affluent counterparts, who are more likely to die in the hospice. This is potentially inequitable, does not necessarily reflect need and has resource implications.
Poster 14
Stroke imaging – you can’t always get what you want….
N Mooney1, N Parkes2 and T Baird3
1University of Glasgow, UK
2University of Sydney, Australia
3Institute of Neurological Sciences, Queen Elizabeth University Hospital, UK
Abstract
Abstract
Background: Appropriate utilisation of healthcare resources such as imaging and bed days confers economic benefit. Imaging preferences/pathways in the acute stroke unit of a large teaching hospital were interrogated to identify potential new models of working.
Methods: Data were collected on imaging modalities and length of stay in patients admitted to the ASU over a combined period of three weeks. In parallel, junior and senior doctors admitting patients completed a questionnaire on which imaging modality they thought was appropriate for each patient. The focus of this study was on patients with minor strokes; length of stay (LOS) ≤7 days was chosen as a surrogate marker for this.
Results: The majority (94%) of patients had computed tomography (CT) as primary imaging, 6% of patients had magnetic resonance imaging (MRI) and 56% of patients had both CT and MRI. Questionnaire data revealed that in 67% of cases, the junior doctor felt that CT was the best imaging modality. On senior doctor review, CT was thought to be best in only 42% of cases. Overall, 92% of patients in whom the senior doctor felt MRI was best first line had a CT first.
Conclusions: In the majority of cases, the senior doctor reviewing the patient felt that an MRI would be the best primary investigation; however, most patients still had CT as a first line test. This discrepancy is likely due to a variety of factors but primarily due to 24/7 availability of CT and relative difficulty in accessing urgent MRI. Duplicate brain imaging was frequent, potentially increasing LOS. Cost savings could be made if imaging pathways were streamlined.
Poster 15
Identification of cognitive impairment and delirium in decompensated heart failure
S Mitchell1, K Jones2, J Taylor2 and T Quinn2
1University of Glasgow, UK
2Glasgow Royal Infirmary, UK
Abstract
Background: Delirium is common in older hospitalized patients and associated with morbidity and mortality. There has been limited study of delirium in patients admitted with acute decompensated heart failure (ADHF). The local target is to perform cognitive screening in all older unscheduled admissions and implement delirium prevention/management in those at risk.
Methods: Patients admitted to a cardiology ward, admitting unselected adults with cardiovascular pathologies not requiring level 2 care, with ADHF were screened over five weeks. Cases were identified by case-note review. We recorded any completed cognitive assessment before assessing ADHF patients using the 4-A test (4AT), 10-point abbreviated mental test (AMT) and a questionnaire for cognitive impairment (AD8). The Think, Investigate, Manage, Explore (TIME) bundle is used to initiate delirium prevention/management.
Results: We identified 43 patients, mean age 78.7 years (range 52–95). Two patients refused, one was terminally ill. Of 40 patients assessed, AMT4 and 4AT were completed by ward staff in 85% and 45%, respectively. The TIME bundle was initiated in 42.5% of patients, none fully completed. Four patients had an established diagnosis of cognitive impairment. Following our assessment, a further 11 patients were identified as having cognitive impairment, 8 of these had not been identified by the treating team. Eight (20%) patients screened delirium positive; five also had likely underlying cognitive impairment.
Conclusions: Cognitive impairment, in particular delirium, is common in patients hospitalized with ADHF, but recommended screening and management bundles are infrequently completed. This has important implications for the training of healthcare professionals around recognition and management of these conditions.
Poster 16
Transfer of patients from off-site care of the elderly wards to acute hospital – what are the main reasons for this and are they preventable?
F Catterall, J Reid and C McCarthy
Queen Elizabeth University Hospital, UK
Abstract
Background: Many care of the elderly (COTE) departments have a variety of inpatient locations. Rehabilitation wards may be remote from the acute hospital, which can present a challenge if a patient becomes unwell. We reviewed the patient demographics and reason for emergency transfer to identify whether these moves were preventable.
Methods: A prospective analysis of patient case notes who were transferred back from off-site rehabilitation wards to the acute hospital from 27 April 2016 to 26 June 2016.
Results: A total of 23 patients were transferred during this period: seven in the first week, eight during the first month and seven more than one month after moving off-site. Sixteen patients had no plan documented in the event of deterioration. The most commonly cited reason for transfer was acute medical illness (12 patients). Eleven patients required input from other specialties not available off-site. Two patients were quickly acknowledged to be approaching end of life and managed symptomatically.
Conclusions: While these patients are often deemed ‘stable’, acute deterioration in this population is not uncommon. Rapid assessment and management of a deteriorating patient on remote sites with reduced after-hours medical and diagnostic support can be challenging, often making transfer to an acute site the safest option. Robust escalation policies should be in place for these sites. With advance care planning, some of these transfers may have been preventable.
Poster 17
Short forms of the Montreal Cognitive Assessment – a systematic review
JA McDicken1, G Blayney1 and T Quinn2
1Doctor, Department of Medicine for the Elderly, Queen Elizabeth University Hospital, UK
2Doctor, Institute of Cardiovascular and Medical Sciences, Glasgow Royal Infirmary, UK
Abstract
Background: The Montreal Cognitive Assessment (MoCA) was developed to detect mild cognitive impairment (MCI) but there is a need for shorter screening tools. Various abbreviated versions have been developed which aim to discard less useful items while maintaining diagnostic accuracy. Our aim was to review the evidence for these shortened MoCAs and compare accuracy in detecting dementia or MCI.
Methods: We carried out a systematic literature review. We used the Quality Assessment for Diagnostic Test Accuracy Studies (QUADAS-2) tool to assess methodological quality and risk of bias. We assessed reporting quality using the dementia-specific extension to the Standards for Reporting of Diagnostic Accuracy (STARDdem) tool.
Results: We screened 593 titles and included 10 studies and 3 conference abstracts. There was significant study heterogeneity. Most were small and included diverse patient groups. Each short form varied in length, domains tested and cut-off point. No study scored low risk on all QUADAS-2 items. Areas of concern included patient selection and choice of reference standard. Reporting quality was variable and no study reported all items recommended in STARDdem. Diagnostic test accuracy varied but there was generally a pattern of high sensitivity and lower specificity.
Conclusion: There are many shortened MoCAs available but there is not one which is clearly superior in terms of diagnostic accuracy. There is significant heterogeneity between studies and many have limitations in terms of reporting and potential biases. It seems likely that there is a role for a shortened MoCA but clinical utility is not yet proven.
Poster 18
Is there an increase in expression of autophagy-related proteins in the dorsal root ganglion after sciatic nerve crush injury?
EA Logan and MR Andrews
University of St. Andrews School of Medicine, UK
Abstract
Background: Autophagy is a catabolic cellular process whereby expired cytoplasmic proteins and organelles are sequestered into a double membrane structure, the autophagosome, and degraded by lysosomes. Although autophagic activity is known to be upregulated after spinal cord injury (SCI), the regenerative value of this is yet undetermined. We proposed to determine whether expression of autophagy-related proteins in the dorsal root ganglion (DRG) is increased after peripheral nerve injury, and thereby in a model of successful nerve regeneration.
Methods: We investigated whether expression of the autophagic proteins light chain 3 (LC3), p62 and tumour necrosis factor receptor-associated factor 6 binding protein (T6BP) is increased in the DRGs of rats that have suffered unilateral sciatic nerve crush injury. Immunohistochemistry and western blot analyses were used to analyse both the uninjured and injured DRGs at four separate time points to determine protein levels.
Results: The DRGs housing the cell bodies of injured primary neurons exhibited greater activating transcription factor 3 (ATF-3) staining, confirming that these neurons were under stress. Immunohistochemical analysis of LC3 was inconclusive due to the highly suspected presence of lipofuscin. Immunohistochemical analysis of p62 was suggestive of no increased expression post-injury. Furthermore, analysis of the western blots suggested no increased expression of LC3-II or T6BP in response to injury.
Conclusion: The results are suggestive of no increased expression of autophagy-related proteins in the DRG after SCI. Further investigation for expression of these proteins at axonal points distal to the DRG will provide insights into autophagy’s role in post-SCI regeneration.
Poster 19
Outcomes post-lung resection surgery: does body mass index have an effect?
E Logan1, SA Singh2, T Fujiwara3, A Kirk2 and M Klimatsidas2
1Undergraduate Medical School, University of Glasgow, UK
2Thoracic Surgery, Golden Jubilee National Hospital, UK
3Clinical Nutrition, Golden Jubilee National Hospital, UK
Abstract
Background: Studies show a protective effect of increased body mass index (BMI) in lung cancer survival. However, surgical risk and post-operative complications in obese patients (BMI ≥ 30) are greater. Obese patients in other surgical specialities have benefited from Enhanced Recovery Programmes (ERP) but its impact for thoracic patients is undetermined. We researched outcomes of patients at Golden Jubilee National Hospital’s unit since ERP’s implementation.
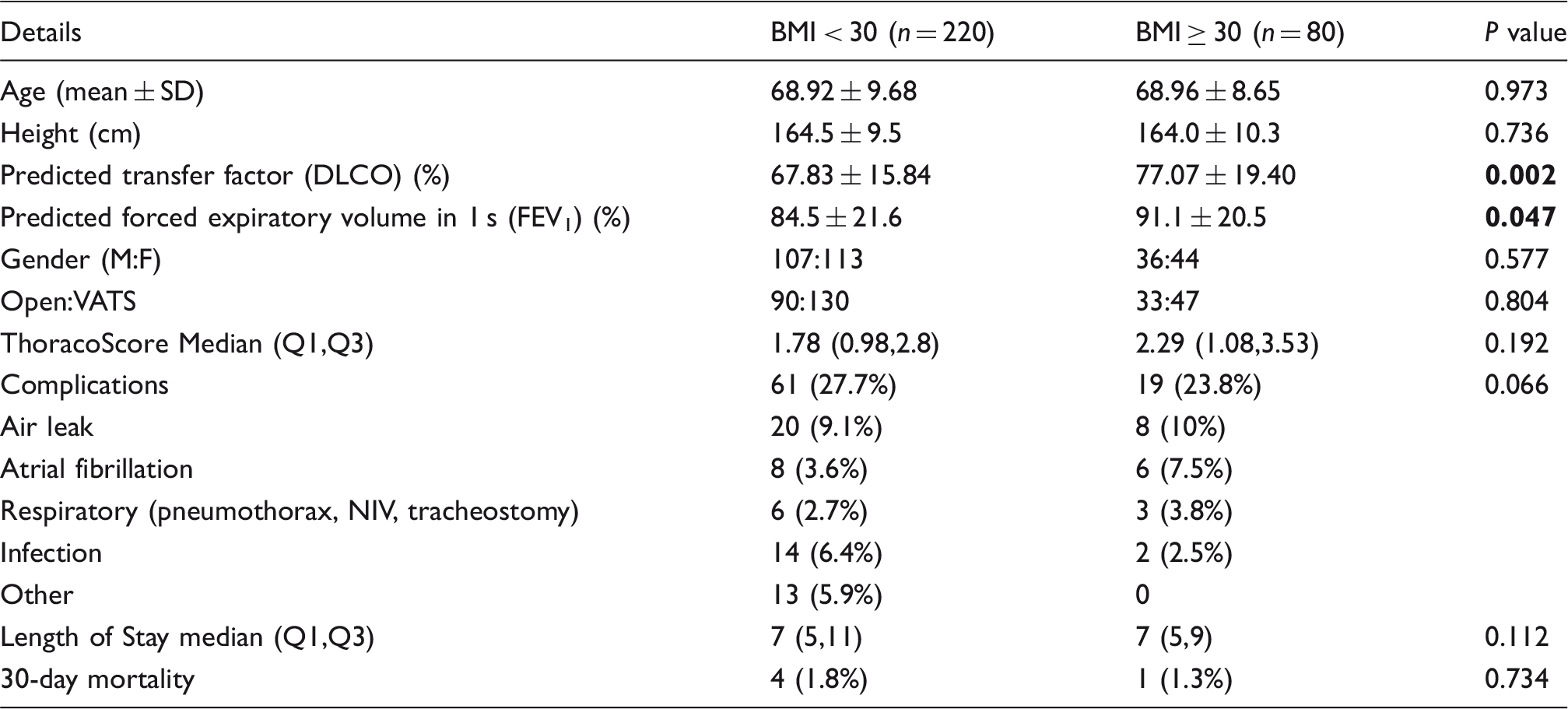
Methods: A retrospective cohort study was performed on all patients undergoing first-time lobectomies for primary lung cancer from January 2015 to June 2016. Patients with BMI < 18 were excluded. Student’s t test, Mann-Whitney U test and chi-squared analysis were used for demographic and outcome analyses. Forced expiratory volume in 1 s (FEV1) was significantly lower in BMI ≥ 30 group compared to BMI < 30. DLCO in the BMI ≥ 30 was significantly higher. There were no statistically significant pre-operative and post-operative parameter differences between the groups. Patients with BMI ≥ 30 had lower complication rates, higher ThoracoScores and shorter hospital stays: these were not statistically significant.
Conclusion: Patients with BMI ≥ 30 perform just as well as patients with BMI < 30 when undergoing lobectomy for lung cancer in an ERP.
Details
BMI < 30 (n = 220)
BMI ≥ 30 (n = 80)
P value
Age (mean ± SD)
68.92 ± 9.68
68.96 ± 8.65
0.973
Height (cm)
164.5 ± 9.5
164.0 ± 10.3
0.736
Predicted transfer factor (DLCO) (%)
67.83 ± 15.84
77.07 ± 19.40
0.002
Predicted forced expiratory volume in 1 s (FEV1) (%)
84.5 ± 21.6
91.1 ± 20.5
0.047
Gender (M:F)
107:113
36:44
0.577
Open:VATS
90:130
33:47
0.804
ThoracoScore Median (Q1,Q3)
1.78 (0.98,2.8)
2.29 (1.08,3.53)
0.192
Complications
61 (27.7%)
19 (23.8%)
0.066
Air leak
20 (9.1%)
8 (10%)
Atrial fibrillation
8 (3.6%)
6 (7.5%)
Respiratory (pneumothorax, NIV, tracheostomy)
6 (2.7%)
3 (3.8%)
Infection
14 (6.4%)
2 (2.5%)
Other
13 (5.9%)
0
Length of Stay median (Q1,Q3)
7 (5,11)
7 (5,9)
0.112
30-day mortality
4 (1.8%)
1 (1.3%)
0.734
BMI: body mass index; NIV: non-invasive ventilation.
Poster 20 (winner best poster – student)
Audit of preoperative investigations prior to elective surgery
G Bowie1 and S Noble2
1Fourth Year Medical Student, University of Glasgow, UK
2Consultant Anaesthetist, Glasgow Royal Infirmary, UK
Abstract
Background: National Institute for Clinical Excellence (NICE) released new guidelines in April of 2016 outlining the correct investigations required prior to elective surgery. This audit was carried out to identify whether the appropriate investigations were being organised at preoperative assessment in the Glasgow Royal Infirmary and to calculate the cost of any investigations deemed unnecessary according to NICE.
Methods: The audit involved collecting data from various surgical specialties at random over a four-week period during an SSC placement. Permission was sought from the supervising consultant. The data collected listed the preoperative investigations the patients received and the patients ASA grade. This was then compared to the NICE guidelines to ascertain whether unnecessary tests were being ordered.
Results: Of the 46 patients reviewed in this audit, 62 unnecessary tests were carried out including, 13 FBC, 9 coagulation, 10 U and E, 29 LFTs and 1 additional ECG. Only 33% of the patients didn’t receive any unnecessary investigations. The cost of these additional tests was £411.93.
Conclusion: The unnecessary expenditure works out at £8.95 per patient. If this sample represents typical practice then in National Health Service hospitals throughout the UK, huge savings could be made by adhering to the NICE guidelines.
Poster 21
Chest X-ray is not indicated in referral for patients with suspected head and neck cancer
Patricia Fingland1, Theofano Tikka2, Catriona Douglas2 and Jennifer Montgomery2
1University of Glasgow Medical School, UK
2Department of Otolaryngology – Head and Neck Surgery, Queen Elizabeth University Hospital, UK
Abstract
Background: Scottish Referral Guidelines (SRG) for patients with suspected cancer in primary care recommend that persistent hoarseness lasting >3 weeks should be referred urgently to the head and neck team, with a chest X-ray (CXR) requested simultaneously. This audit aimed to identify adherence to these guidelines, and to audit CXR results for relevance related to the referral.
Methods: All urgent suspicion of cancer referrals to the ear, nose and throat department in National Health Service Greater Glasgow and Clyde between June 2015 and 2016 were audited. Referrals were assessed for adherence, presence of CXR and results. Data included patient demographics, presenting symptoms, final diagnosis and management. Information was recorded anonymously in an excel spreadsheet.
Results: A total of 2144 referrals were received. Of these, 1977 were included in the audit. Mean age of patients was 59 years. There were 855 (43.2%) male patients. Persistent hoarseness >3 weeks instigated the referral in 548 (26.3%) patients. CXR was performed in 120 (21.6%) patients. In these patients, it showed no abnormality (116, 96.7%), features of infection (2, 1.7%) and features suggestive of pulmonary malignancy (1, 0.8%). Total cancer detection rate was 12.0%. Head and neck cancer was identified in 170 (8.6%). Referrals were appropriate to SRG in 1205 (56.0%).
Conclusions: The CXR findings did not alter management in any patients, and this should be removed from the SRG for suspected cancer.
Poster 22
Patients’ attitudes towards rubber dam: a practice-based audit
F McKirdy and A MacDonald
The University of Glasgow, UK; MacEndo, UK
Abstract
Background: Rubber dam is a latex sheet used to isolate a patient’s tooth during non-surgical root canal treatments. The benefits of using it are well documented but there is great discordance in this standard of care and its use in dental practice. Patients’ perceived negative attitude towards its use is cited as a main reason for its lack of use by general dental practitioners, as is time taken to place it. This audit aims to discover patients’ attitudes towards rubber dam in order to promote its use in general dental practice.
Methods: Twenty-one patients at a private endodontic referral practice were given questionnaires after treatment to assess their attitudes towards the use of rubber dam, and placement time was measured in 13 patients.
Results: Twenty-one questionnaires were collated. 24% found rubber dam pleasant, 71% comfortable, 5% uncomfortable and none found it painful; 95% would prefer it to be used at their next appointment and 5% expressed no preference. All (100%) patients would recommend it to a friend undergoing similar treatment. The mean time taken to place the rubber dam was 121 s (range 98 s–158 s).
Conclusions: This audit further strengthens evidence that patients report their treatment experience to be better with the use of rubber dam and time measurements show it is quickly placed. Rubber dam is considered the standard of care for non-surgical root treatment and as patients prefer its use, there is little argument for the lack of acceptance among the dental profession.
Poster 23
Analysis of paediatric usage of caspofungin and cost-based comparison with a similar echinocandin micafungin
D Clayton1, R Hague2 and C Doherty2
1Student, University of Glasgow Medical School, University Ave, UK
2Royal Hospital for Children, UK
Abstract
Background: Invasive fungal infections account for a significant burden to the healthcare system and are the leading cause of death in children with cancer or following haematopoietic stem cell transplant. With the crude mortality associated with invasive fungal infections in paediatric patients being reported as high as 60%: it is essential that anti-fungal agents such as the echinocandins are studied and audited to maximise efficacy and cost-effectiveness of current treatment regimens. The aim of this project was to analyse the usage of caspofungin in a busy children’s hospital over a period of 12 months from January 2015 to January 2016 and create a cost comparison with micafungin – a very similar echinocandin antifungal.
Methods: A total of 16 patients treated with caspofungin in the time period were identified and key case information extracted by the use of a data collection form that preserved anonymity. The pharmacy caspofungin order forms displayed the number of vials used in each patient’s treatment and the resultant cost of treatment was calculated. Through looking at the British National Formulary for treatment using micafungin – a theoretical treatment regimen could be formulated and resultant number of vials of micafungin required calculated. The cost of this theoretical treatment could then be compared with the actual treatment that was used.
Results/Conclusion: The project found that a theoretical total of £74,352.74 could have been saved if micafungin had been used as the echinocandin of choice in the hospital, however, more research is required to assess whether their efficacy in treatment can said to be truly equal.
Poster 24
The effectiveness of the Airsonett device in treating severe asthma patients
S Mustafa and D Cowan
Third Year SSC, Medical School, University of Glasgow, UK
Abstract
Background: Airsonett is a laminar airflow device that provides filtered, allergen-free air to the breathing zone of patients with severe asthma as they sleep, resulting in fewer asthma attacks during the night. This audit was used to determine its effectiveness on nine patients at a severe asthma clinic in Glasgow, in terms of their health and quality of life.
Methods: The following measurements were recorded at baseline and at the patients’ one-year review of the device: immunoglobulin E (IgE) levels for different allergens and spirometry results; scores from three questionnaires assessing their control of their asthma, used to assess quality of life; extra information regarding quality of life was also gleaned from clinical letters.
Results: The results revealed that the patients found an improvement in their quality of life (P = 0.0156), due to better sleep and fewer asthma attacks. The IgE results, lung function tests and number of hospital/GP visits showed no significant improvements. The clinical letters described that 6/9 patients felt they benefitted from the device, and they all described:
• Fewer nocturnal symptoms
• Improved nasal symptoms
• Better quality of life
• Brought up less mucus
The other three patients had poor adherence and did not feel an improvement.
Conclusions: It was concluded that the quality of life of the patients improved, which was shown by the improved questionnaire results. This is backed up by the improved symptoms described in the clinical letters. These coupled with the fact that six out of nine patients saw an overall benefit, imply that Airsonett is an effective treatment for severe asthma. Two previous studies, from Boyle et al and Pedroletti et al., also concluded significant improvements in quality of life after Airsonett use.1,2
References
Boyle RJ, Pedroletti C, Wickman M, et al. Nocturnal temperature controlled laminar airflow for treating atopic asthma: a randomised controlled trial. Thorax 2011. doi:10.1136/thoraxjnl-2011-200665 http://thorax.bmj.com/content/early/2011/11/07/thoraxjnl-2011-200665.long.Pedroletti C, Millinger E, Dahlén B, et al. Clinical effects of purified air administered to the breathing zone in allergic asthma: a double-blind randomized cross-over trial. ResMed J 2009; http://www.resmedjournal.com/article/S0954-6111(09)00101-2/fulltext.
Poster 25
Modelling the effect site compartment in a target-controlled infusion of propofol
A Croall1, C Hawthorne2 and M Shaw2
1Wolfson Medical School, University Ave, UK
2Institute of Neurological Sciences
Abstract
Background: Target-controlled infusion (TCI) devices rely on pharmacokinetic (PK) models to predict drug concentrations. Extension of PK models through the addition of a rate constant for elimination (ke0) from a theoretical ‘effect site’ compartment allows estimation of the time course of clinical effect of a drug relative to the plasma concentration. The original Marsh Model for TCI protocol adjusted PK compartment volumes based on the patient covariate of weight. The Covariates Model has updated the original model via the inclusion of additional gender and age covariates. This study is a companion study to the Validation Study of the Covariates Model (VaSCoM). The primary aim of this study was to determine the ke0 for the Covariates Model using a non-parametric technique.
Methods: Data sets from 30 patients anaesthetised using the Covariates Model were used. In a non-parametric approach to ke0 calculation, measured drug concentrations, as opposed to concentrations predicted by the PK model, are compared to some clinical measure. In this study, we had a total of 126 arterial propofol concentrations taken during the first 20 min of anaesthesia to compare to the continuously recorded Bispectral Index (BIS, Medtronic, ROI). A population ke0 was estimated using non-linear mixed effects modelling (NLME) implemented in the R package nlmeODE.
Results: Both random and fixed effects ke0 estimates were determined. The overall population estimate for ke0 for the covariates model was 0.273 min–1.
Conclusions: The ke0 determined here is similar to that calculated in the same data set using a parametric technique (0.254 min–1), and to that used in the original implementation of the Marsh Model in the Diprifusor® (0.26 min–1). Therefore, a ke0 of between 0.25 and 0.27 min–1 should be reasonable to use in any clinical implementation of the Covariates Model.
Poster 26
The modulating effects of polyphenols found in green tea on the gut microflora: a systematic review
JY Chen
University of Glasgow, University Avenue, UK
Abstract
Background: In the Western world, our dietary intake of polyphenols is mainly from fruits, vegetables and beverages, and is around 0.15–1 g/day despite no recommended daily requirement. Polyphenols are micronutrients relating to any molecule with several hydroxyl groups on an aromatic carbon ring. Dating back to ancient China, polyphenols have been widely believed to benefit the body despite being only partially absorbed. The remainder is either metabolised by the gut or excreted. Green tea makes up 20%–22% of the tea consumed worldwide and is very rich in dietary polyphenols (>30% of dry weight). There is little known about the in vivo effects of green tea bio-compounds on specific gut microflora bacteria; therefore, this review aimed to investigate this.
Methods: Two systematic searches on Web of Science and PubMed were carried out using relevant inclusion and exclusion criteria regarding green tea and its modulating effect on the gut.
Results: Green tea polyphenols are much more bioavailable than previously thought (39%). Tea polyphenols did not significantly alter the quantity of putrefactive products in the colon which is consistent with previous studies. However, polyphenols increased acid-forming beneficial bacteria (lactobacilli and bifidobacterium) and decreased harmful bacteria (clostridia). Products of flavan-3-ol degradation were detected exclusively in the urine of green tea drinkers.
Conclusions: There is great interindividual variation in the urinary excretion of colonic metabolites. With regular consumption, green tea can inhibit putrefactive bacteria and promote beneficial bacteria, but these effects are short-term. Clostridium is a risk marker for colon cancer so a polyphenol-rich diet may be cancer protective.
Poster 27
A novel prospective study of missed lung cancers on chest radiographs – what is an acceptable miss?
NTH Khoo and S Kearney
▪▪
Abstract
Introduction: The chest X-ray (CXR) remains the single most important investigation in the detection of lung cancer. Unfortunately CXR identification can be challenging leading to missed cancers and delayed diagnosis. Benchmarking to establish standards for identification of lung cancer on CXR is difficult. This results in challenges for radiologists to evidence quality of reporting and determining whether a retrospectively ‘missed’ lung cancer should be bound by Duty of Candour.
Methods: We developed an online self-assessment, peer comparison module for CXR identification of lung cancer. (www.xrayetc.org, Access Code: LungCancer2016). Ten CXRs comprising missed, reported lung cancers and normals were included. Answers with explanation and comparison results were provided. Radiologists across the UK and local radiographers where invited to complete the module. User feedback was requested. Assessment results were analysed.
Aims: Feasibility of benchmarking performance standards for a range of ‘missed’ lung cancers. Potential to develop of a validated set of ‘missed’ lung cancer for QA purposes.
Results: OVERALL: Seventy-five completed the module (50 consultants – 28 chest radiologists (CCRs), 22 non-chest radiologists (CNCRs), 15 trainees, and 10 radiographers. User feedback was very positive. CONSULTANT: Average score 7.1/10 (range 3–10). CCRs 7.4 (3–10) and CNCRs 6.8 (5–9). Average time taken per question 54.9 s. Four of the six missed cancers identified by >50%. Conclusion: This online self-assessment allows participants to assess their performance in the identification of lung cancer on a challenging set of CXR, with educational feedback. Results from all those completing the module are available to the participant, therefore allowing peer comparison which is a requirement of revalidation.