
Abstract
Background
Immunosuppression helps prevent acute rejection post-cardiac transplant but has been linked to malignancy development. This may be due to a reduction in T-lymphocyte function, a direct oncogenic effect or the increased impact of environmental carcinogens. There has been shown to be significant increases in non-melanoma skin cancers and post-transplant lympho-proliferative disorders, particularly in those treated with OKT3.
Aim
To investigate the survival and incidence of malignancy in the Scottish cardiac transplant population and whether rates of non-melanoma skin cancers justify the provision of specialist dermatological follow-up.
Methods and results
Retrospective case note analysis of patients transplanted (363) or followed up (2) in Scotland from 1992 to 2016. Kaplan–Meier survival analysis generated a survival curve. Patients had a 1-year survival of 82% and a median survival of 10.9 years. There were 60 (95% CI 47.5, 75.2) NMSCs and 8 (3.7, 12.4) post-transplant lympho-proliferative disorders diagnosed in the cohort (3110 person years follow-up). Fisher’s exact test was employed to analyse the association between induction therapy (via OKT3 or rabbit antithymocyte globulin) and post-transplant lympho-proliferative disorder development. Patients treated with OKT3 had a 6.7 times greater risk (P = 0.014) and a shorter experience of patients treated with rabbit antithymocyte globulin has so far shown no significantly altered risk (P = 1.00) of developing a post-transplant lympho-proliferative disorder.
Conclusion
Incidences of non-melanoma skin cancers and post-transplant lympho-proliferative disorders were increased in the Scottish cardiac transplant population and there was a significant association between post-transplant lympho-proliferative disorder development and OKT3 therapy but not rabbit antithymocyte globulin therapy. These findings in Scottish patients reflect what is published in wider literature and support the provision of a dedicated post-transplant dermatology clinic.
Introduction and background
Cardiac transplantation has been carried out in Scotland since 1992. The service has been located at the Golden Jubilee National Hospital (GJNH) since 2008. There have been 363 patients transplanted since the start of the service, with the majority being followed up at the GJNH.1,2
Complications after cardiac transplant are both common and important. Specific complications such as acute rejection can be devastating to both the graft and patient. Rejection is an immune-led reaction to the graft and is one of the leading causes of death up to a year after transplant. 3 T-lymphocytes recognise the endothelial cells of the coronary circulation as foreign and mount a response. Endomyocardial biopsies are taken during the first year post-transplant to monitor for rejection.3,4 These samples are graded using the International Society for Heart and Lung Transplantation (ISHLT) system. 5
Episodes of acute rejection are treated with pulsed corticosteroids. However, patients are also prescribed high-dose immunosuppressants as prophylaxis. Scottish patients normally receive a calcineurin inhibitor (tacrolimus (TAC) or cyclosporine (CyA)) and an anti-proliferative agent (mycophenolate mofetil (MMF) or azathioprine (AZA)). The common regimens are outlined in Figure 1.
Current immunosuppressant regimes used by patients in the Scottish cardiac transplant population.
Between January 1995 and December 1998, patients were prescribed the murine monoclonal antibody therapy OKT3, an antibody against CD3+ lymphocytes, to help induce immunosuppression and protect against rejection immediately post-transplant. 6 OKT3 has since been taken off the market due to its well-recognised association with post-transplant lympho-proliferative disorder (PTLD) development. From 2010, patients have instead been treated with rabbit antithymocyte globulin (r-ATG), an anti-thymocyte antibody which also acts against CD3+ lymphocytes. 7 There was no specific induction therapy prescribed on top of routine corticosteroids outwith these periods.
There is a widely acknowledged link between the immunosuppressants used post-transplant and the development of malignancy. Firstly, patients with a malignancy treated with immunosuppressive agents were found to be at increased risk of developing a second de novo malignancy, particularly lympho-proliferative disorders. 8 Secondly, patients with the auto-immune disease psoriasis, treated with the immunosuppressant methotrexate, were shown to be at an increased risk of developing malignancies. 9 Despite the clear link, the mechanism by which immunosuppressants lead to malignancy is not well understood. It may be a direct oncogenic effect on cells, a reduction in the ability of intra-cellular monitoring to eradicate mutated cells or an increased susceptibility to environmental carcinogens (smoke/UV rays) 10 – or a combination of two or more of these.
This paper aims to examine survival probability of patients’ post-cardiac transplant, the incidence of malignancy in this group, particularly non-melanoma skin cancers (NMSC) and PTLDs, and the associated risk of these malignancies with the induction therapies OKT3 and r-ATG. Scottish patients are routinely followed up every six months post-transplant and a specific dermatology clinic has recently been introduced to monitor patients for NMSC post-transplant. This paper also aims to examine if the acknowledged increased risk of NMSC justifies the provision of this service.
Methods
Structure and data collection
A retrospective case note analysis of patients transplanted (363) or followed up (2) in Scotland was carried out. This includes 285 male and 80 female patients. All basic patient data had previously been collated in a register for clinical use. Permission to use the data was granted by the transplant team at the GJNH. Patients were divided into those alive and deceased. Data were extracted (regarding medication regimen and malignancy) from paper case notes for surviving patients and from the Scottish Care Information (SCI) store, under supervision by the transplant team, for deceased patients. Patients were assigned a number and any identifiers (name, D.O.B., CHI number) were removed. Data from the transplant register and case notes were then transferred to a spreadsheet within the GJNH intranet. No identifiable information was removed from the internal GJNH servers or transplant office. The register was returned to the transplant team after data collection.
This study consisted of auditing clinical information and did not constitute research in accordance with the NHS Health Research Authority guidelines. 11 Therefore, an application to the Regional Ethics Committee was not required.
Kaplan–Meier survival analysis
Kaplan–Meier survival analysis was employed to generate a survival probability curve 12 via PRISM (version 5.1). The time interval between transplant and death was calculated for each patient. Surviving patients were included as censored data, with survival calculated as the time between transplant and 12 September 2016 (the start of data collection). Median survival probability and 95% confidence intervals (95% CI) were calculated.
Immunosuppressant and malignancy analysis
Information regarding immunosuppressant regimen and malignancy was collated. To assess the incidence (95% CI) of NMSCs and PTLDs in the post-transplant population, a crude incidence rate was calculated using person-years spent in follow-up. The length of time each patient contributed was calculated and summed. 95% CI were generated using the Adjusted Wald technique for binary data. A two-tailed Fisher exact test was used to calculate an odds ratio to assess association between the use of induction therapy (OKT3 or r-ATG) and the development of PTLD. A result was deemed statistically significant when P < 0.05 (* on accompanying bar chart (Figure 6A)).
Results
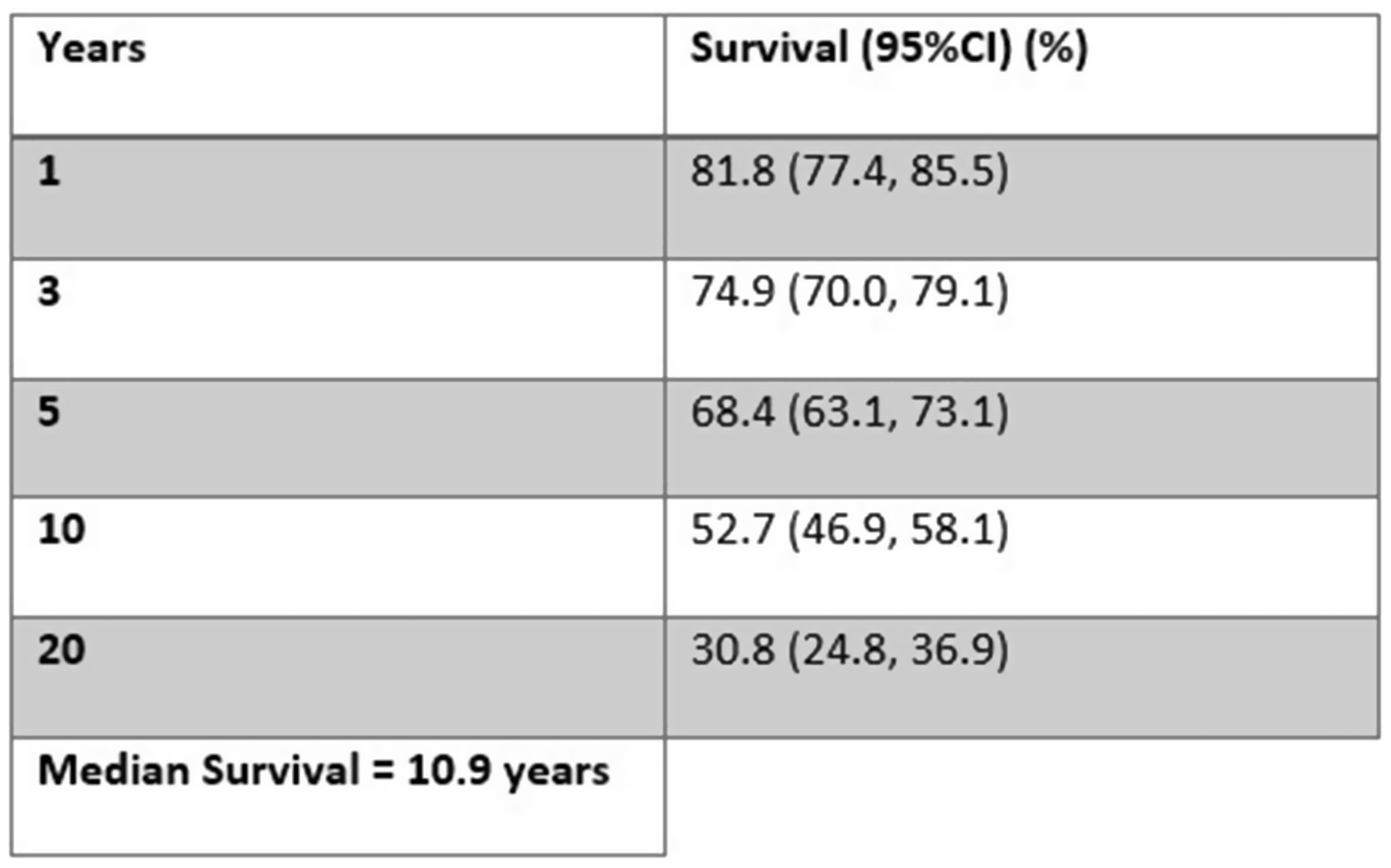
Patients transplanted or followed up in Scotland (365) had a median survival of 10.9 years (Figures 2 and 3). Survival was shown to be 81.8% (77.4, 85.5) at one year, with 52.7% (46.9, 58.1) of patients surviving to 10 years (Figure 3). The steep 18.2% drop in the first year post transplant is followed by a steady, stepwise decline. It takes a further 6.2 years for survival to decrease by another 18.2% (Figure 2).
Kaplan–Meier survival curve showing the percentage survival of patients from date of transplant to 26 years post-transplant. There were 151 surviving patients at the time of data collection. 18.2% of patients died during the first year post-transplant, with a stepwise decrease in survival from year one onwards. Patient survival at 1, 3, 5, 10 and 20 years’ post-cardiac transplant.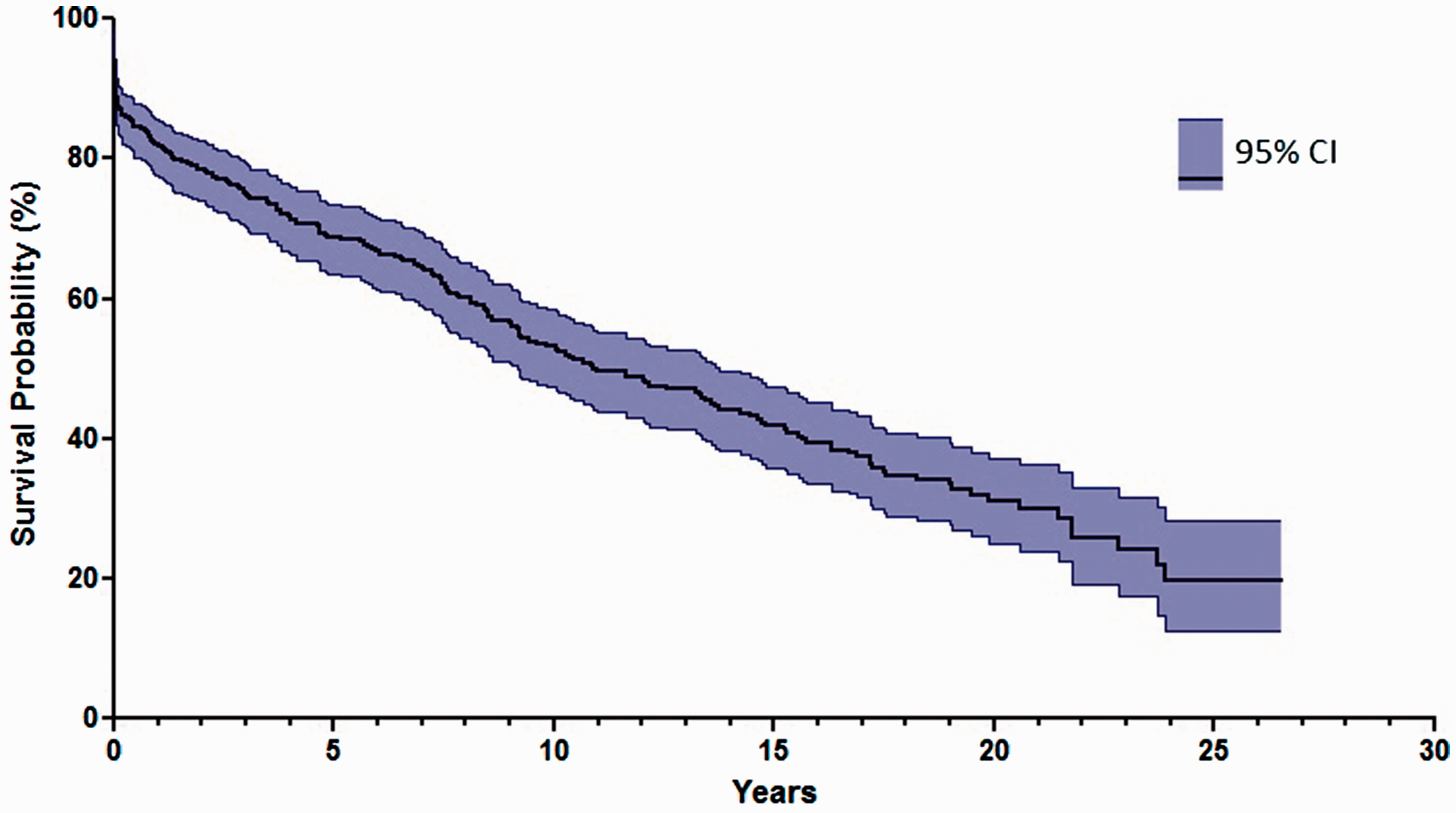
The most commonly used immunosuppressive regime post-transplant was CyA and MMF (Figure 4). One hundred sixteen patients were given additional OKT3 induction between 1995 and 1998 (Figure 4) and 72 patients were given r-ATG between 2010 and 2016 to induce immunosuppression on top of prednisolone.
The most commonly used immunosuppressive regime was cyclosporine and mycophenolate mofetil, with 216 patients prescribed this combination. There are still 111 patients taking cyclosporine and azathioprine, the first choice regime when the transplant service was established in 1992. Thirty three patients are using the now favoured tacrolimus and mycophenolate mofetil combination, with five having substituted mycophenolate mofetil for azathioprine. One hundred sixteen patients received induction via OKT3 therapy.
The most common malignancy diagnosed was NMSC with 60 (47.5, 75.2) cases. There were 8 (3.7, 12.4) PTLD diagnoses recorded as well as four lung, three breast and three laryngeal malignancies. There were additional sporadically diagnosed malignancies, bringing the total number to 89 (Figure 5). NMSCs, unlike other malignancies, were inconsistently recorded in individual patient’s case notes. This is likely due to their often insignificant effect on clinical management. Extensive reading of both hard and electronic case notes was thought to minimise this, but it is likely there is a degree of under-reporting of NMSCs.
The number and types of malignancies diagnosed in the post-cardiac transplant population.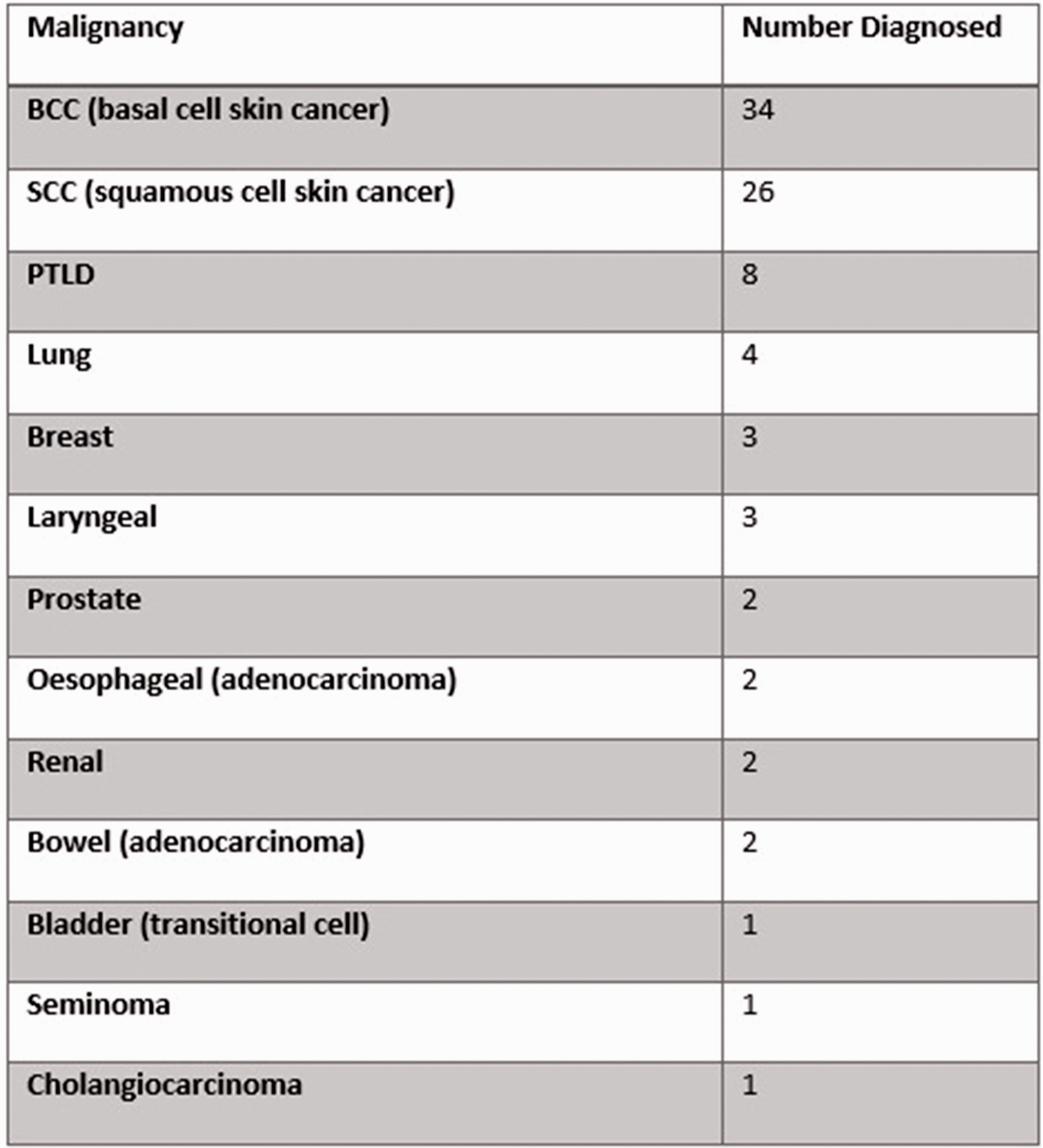
There was a statistically significant association between the development of PTLD and the group (n = 116) that received OKT3, odds ratio = 6.7 (P = 0.014) (Figure 6). There was no statistically significant association between PTLD development and the group (n = 72) that received r-ATG, odds ratio = 0.5 (P = 1.00) (Figure 6).
Significant association between the use of OKT3 and the development of post-transplant lympho-proliferative disorder (odds ratio = 6.7). No significant association between the use of the new induction agent rabbit antithymocyte globulin and the development of post-transplant lympho-proliferative disorder (odds ratio = 0.5, P = 1.00).
Discussion
Survival post-cardiac transplant
Scottish patient survival one-year post-transplant was 81.8% (77.4, 85.5) (Figures 2 and 3). This is marginally lower than the European survival range at one-year of 85–92%. 13 A rate of 85% is accepted as the current survival “target” from analysis of worldwide cardiac transplant data (2009–June 2013). 14 First year survival post-transplant in all UK centres was shown to be 81.3% (77.6, 84.5) for the period between 1 April 2008 and 31 March 2013. 15 Scottish patient survival at three-year was 74.9% (70.0, 79.1), again similar to the UK three-year survival of 76.2% (73.5, 78.7) from 2008 to2013. 15 Median survival was calculated to be 10.9 years in Scottish patients (Figures 2 and 3). ISHLT published worldwide survival data in 2010, stating the median survival post-cardiac transplant to be 12 years. 14 The 151 patients censored in analysis will have an as of yet unknown influence of Scottish patient survival. However, with survival rates post-transplant improving, overall survival rates would be expected to increase.
Non-melanoma skin cancer
NMSCs are the most commonly diagnosed malignancies post-transplant 8 and may have a particular association with cardiac transplants. Such patients have a Standardised Incidence Ratio (SIR) of 18.5 NMSCs compared to the general public, with renal, lung and liver transplants having SIRs of 16.6, 16.1 and 6.6, respectively. 16 There have been 60 (47.5, 75.2) NMSCs diagnosed in the Scottish cohort (3110 person years of follow-up), giving a crude incidence rate of 60 per 3110 person years (1930 per 100,000 person years). This is in comparison to the crude annual incidence of NMSCs in the general population of 207.8 per 100,000 people. 17 This suggests a large increase in the incidence of NMSCs in Scottish transplant patients compared to the general population, though differences in incidence measurement make a direct comparison inappropriate.
The development of NMSC involves the interplay of several variables. 18 AZA is thought to interact with the skin’s innate protection against UV rays, whereby individuals become susceptible to certain UV bands. This increases skin damage and may result in an increased incidence of skin cancer. 19 In another study, 300 patients receiving CyA and AZA, with or without prednisolone, were analysed for risk factors for NMSC. It was found that in those who developed NMSC, sun exposure was significantly higher, and exposure above 10,000 hours, led to an approximate three-fold increase in risk for developing an NMSC. 21 It has also been demonstrated that patients taking CyA are more likely to develop an NMSC than those taking AZA and prednisolone alone. This may explain why cardiac transplant patients display the highest rates of NMSC, as they are maintained on higher levels of CyA than other solid organ transplant patients. 19 One study of 312 post-cardiac transplant patients, transplanted between 1998 and2006 found a total of 1387 NMSCs diagnosed (including multiple NMSCs per patient) in the group, with 46.4% of patients having a skin cancer 19 years post-transplant. This trial did not show a link between NMSCs and immunosuppressants, but suggested that HSV infection, other non-skin cancers post-transplant (SCC only) and older age at transplant were significant risk factors for NMSC development. 20
Despite the likely under-reporting of NMSCs mentioned in the results section, Scottish data reflect results from many transplant centres. To help combat the increased incidence, patients are referred for annual review at a dermatology clinic. This clinic was commissioned to perform regular full body skin examinations to look for, monitor and treat any suspicious lesions as effectively as possible. Patients are also educated in adequate protection when sun-exposed and may be prescribed high factor sunscreen to combat the effects of the UV rays. This clinic may also help diminish any under-reporting of NMSCs.
PTLD
There have been 8 (3.7, 12.4) PTLDs reported in the Scottish cohort, providing a crude incidence rate of 8 per 3110 person years (257 per 100,000 person years). Lympho-proliferative disorders had a crude annual incidence in the general population of 144.9 per 100,000 people (2004–2012 UK). 22 Again, as with NMSC incidence, a risk ratio cannot be directly calculated, but the data does suggest an increase in the incidence of lympho-proliferative disorders in patients post-cardiac transplant.
PTLDs are a well-recognised condition in those who have received a solid organ transplant and are often fatal. There are multiple factors that are thought to increase the risk of developing a PTLD. These include receiving a combined cardiac–lung transplant, a heart or lung transplant on its own, 23 or if the donor is Epstein–Barr Virus positive (via impaired T-lymphocyte surveillance).24,25 However, the immunosuppressive agents themselves are the most important risk factor owing to their chronic use. The calcineurin inhibitors, particularly TAC, have been shown to increase the risk of developing PTLD. 26
OKT3 therapy and PTLD development
There is a clear link between the development of PTLD and the use of OKT3. 24 One study of 154 patients post-cardiac transplant reported nine PTLDs diagnosed in the group that received OKT3 (n = 79) and one in the group that did not (n = 75) (odds ratio = 9.5), 24 with the study noting that OKT3 therapy was the only significant difference between the two groups despite the risk of PTLD with CyA. 27 This study agrees with another that found OKT3 to have an associated PTLD SIR of 21.5 (15.7, 28.8; P < 0.001) compared to non-transplant controls, with no induction having a PTLD SIR of 9.4 (8.3, 10.6; P < 0.001). 28 The Scottish data agree with these results, confirming a significant association between the use of OKT3 and PTLD development in our own experience (odds ratio = 6.7).
OKT3 therapy has not been used in Scottish patients since January 1999 and has since been withdrawn from the market. However, owing to the risk of PTLD and the aggressive nature of these disorders, it is important to monitor patients who have been treated with OKT3 in the past.
The incidence of NMSC and PTLD post-OKT3 or r-ATG therapy
The crude incidence of NMSC in those treated with OKT3 was 1828.2 per 100,000 person years compared to 1814.7 per 100,000 person years in those who received no induction therapy, suggesting that OKT3 therapy itself has had little impact on NMSC. The crude incidence rate of NMSC with r-ATG therapy was 2592.4 per 100,000 person years compared to 1693.7 per 100,000 person years in those who received no induction therapy. Despite the large difference in incidence, there were only a small number (4) of NMSC diagnoses in the r-ATG group. Further monitoring of the cohort and analysis would be required to confirm or exclude an association between NMSC and r-ATG, but it may have an impact on NMSC rates.
The crude incidence of PTLD decreased from 6 per 1258.1 (476.9 per 100,000) person years in those who received the OKT3 to 1 per 826.6 (121.0 per 100,000) person years in those who did not receive any induction agent. The incidence of PTLD in those who did not receive OKT3 (121.0 per 100,000) is indeed similar to that observed in the general population (144.9 per 100,000). Allowing for the low numbers, and the inability to calculate risk ratio, these figures suggest that the risk of developing a PTLD in those not treated with OKT3 may be similar to that in the general population.
The incidence of PTLD in those who have received r-ATG induction therapy is 0 per 154.3 (0 per 100,000) person years. The number of patients treated with r-ATG and time spent in follow-up is much less than for those who received OKT3 or no induction therapy. However, a PTLD is most likely to develop in the first year post-transplant, 29 suggesting if there was an increased risk of PTLD with r-ATG therapy, there may have been some evidence of this in the cohort. This suggests that the risk of PTLD with r-ATG is lower than with OKT3. No association was shown between PTLD development and r-ATG when compared with those who did not receive any induction (odds ratio = 0.5, P = 1.00). The study was clearly not powered to show any difference, but, along with the suggestion that patients who received no induction therapy had a similar incidence of PTLD to the general population, these early results are encouraging that r-ATG may be a safe therapy to use in terms of PTLD risk.
Conclusion
Analysis of Scottish post-cardiac transplant patient data revealed a one-year survival of 82%, which is slightly lower than the European average of 85–92%, although CIs overlap with this European average. Incidences of NMSCs and PTLDs were increased in Scottish patients versus the general population. The importance of the historical immunosuppression inducer OKT3 was confirmed, after the withdrawal of OKT3, the incidence of PTLD reduced almost 6 fold to 1 per 826.6 person years in those that received no induction therapy. So far, there appears to be no significant alteration in risk of PTLD development with r-ATG therapy when compared with no induction therapy. There may be a link between r-ATG therapy and NMSC development, however this will require more monitoring of the cohort to confirm.
The observed NMSC incidence post-transplant of 1929.3 per 100,000 person years suggests a large increase in incidence when compared to the general population. This justifies the provision of a dedicated dermatology clinic. NMSCs will be an ongoing problem in the foreseeable future with the continuing use of current immunosuppressant regimes and the skin type demographics of patients in Scotland. This service will help monitor and treat patients at an early stage and allow easy access to a vital service.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.