
Abstract
Background and aims
Novel psychoactive substances are compounds intended to mimic the effects of illicit drugs. They provide a unique challenge to healthcare, as complications of their use and their impact on services are relatively unknown. This study aims to determine nature of presentations, patient demographics and impact on healthcare.
Methods
Novel psychoactive substances users who presented to a large urban emergency department over 4 weeks were prospectively identified and followed for 1 year. Patients over 13 years old were eligible for inclusion. Information regarding patient demographics and presentations was collected.
Results
During the study period, 53 patients (39 male), mean age 32.6 ± 8.9 (±standard deviation), presented 148 times with complaints relating to novel psychoactive substances use. Study population characteristics included history of illicit drug use (83.0%), intravenous drug use (64.2%), psychiatric diagnosis or symptoms (56.6%), methadone prescription (52.8%) and having no fixed abode (37.7%). Injection was the most common method of use (72.3%), Burst the most commonly named agent (19.6%) and behavioural change the most common presenting complaint (31.1%). Patients collectively spent 10,620 h in hospital over 1 year.
Conclusion
This study highlights differences between the young population targeted by government campaigns regarding novel psychoactive substances use and the presenting population to hospital, and the associated burden on the National Health Service.
Introduction
The emergence of novel psychoactive substances (NPS) or designer drugs has altered the nature of drug abuse in the 21st century. These NPS are associated with a large number of varied presentations at hospitals around the UK 1 and have been linked with anti-social behaviour and mortality.2,3
NPS are synthesised with the intention of reproducing the effects of illicit drugs. 4 Almost half of NPS identified in Europe are synthetic derivatives of cannabinoids and cathinones with marginally altered structures to subvert previous bans. 4 Little is known about these substances – their efficacy, interactions or adverse effects – by either drug users or the scientific community 5 and, owing to lack of regulation of manufacturers, some contain illicit active ingredients.4,6
NPS use presents a growing health concern across the world. This is certainly true in the UK, which was highlighted in 2013 as the single largest NPS market outside of the United States. 7 Despite their popularity, a 2015 review of designer drugs emphasised that ‘the incidence of designer drug problems in emergency departments (EDs), hospitals and other medical settings is largely unknown’. 8
This study aims to determine the number and nature of NPS-related presentations, the patient demographic, and their impact on the healthcare system at a large urban ED.
Methods
This year-long observational study identified a group of NPS users who presented during an initial 4-week period (26 January 2015 to 22 February 2015) to the Royal Infirmary of Edinburgh’s ED, and then subsequently followed them over the year (23 February 2015 to 25 January 2016). At the time, this ED was the largest adult ED in Scotland and was estimated to cater for 113,000 attendances from Lothian, East Scotland, with an approximate ‘majors to minors’ ratio of 1:1 and admission rate of ∼30% (2012 estimates). 9
Patients over the age of 13, with NPS-use both recorded in their routine history and thought to be related to their presenting complaint, were eligible for study inclusion.
Information regarding patient demographics (gender, age at presentation, history of no fixed abode, methadone prescription, psychiatric diagnosis or symptoms (e.g. depression or depressed), and their hepatitis C status), drug use (past and present), method of NPS use, reason for presentation, time of presentation and final discharge from hospital was collected and subsequently anonymised.
For this study, named NPS were categorised into stimulants and synthetic cannabinoids, based on information provided through contact with staff working for www.mycrew.org.uk. 10 Presenting complaints were categorised under five headings: trauma, infection/inflammation, pain (unrelated to infection/inflammation or trauma), behavioural changes and collapse/reduced Glasgow Coma Scale (GCS).
In addition to identification by ED staff, Trak (the hospital information system) was used to identify relevant patients and their records. General Practice and patient records from other hospitals were not accessed.
Results
Demographic details of the patient population of NPS users who presented over a 4-week period (n = 53) in addition to their subsequent presentations deemed related to NPS use.
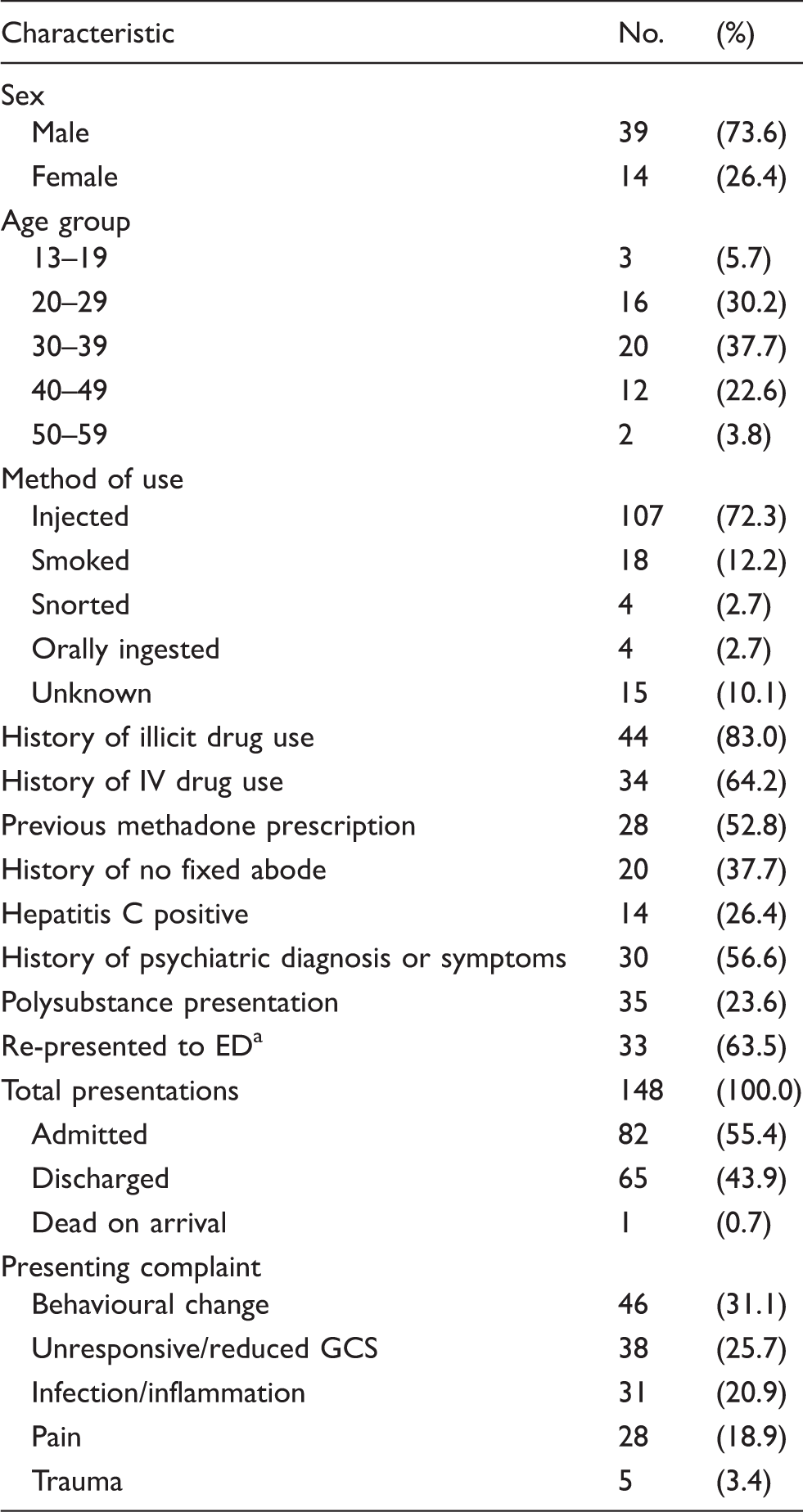
Percentages calculated either based on patient population (n = 53) or total presentations (n = 148).
Percentage based on patient population of 52, with the patient who was dead on arrival excluded.
NPS: novel psychoactive substances; IV: intravenous; ED: emergency department.
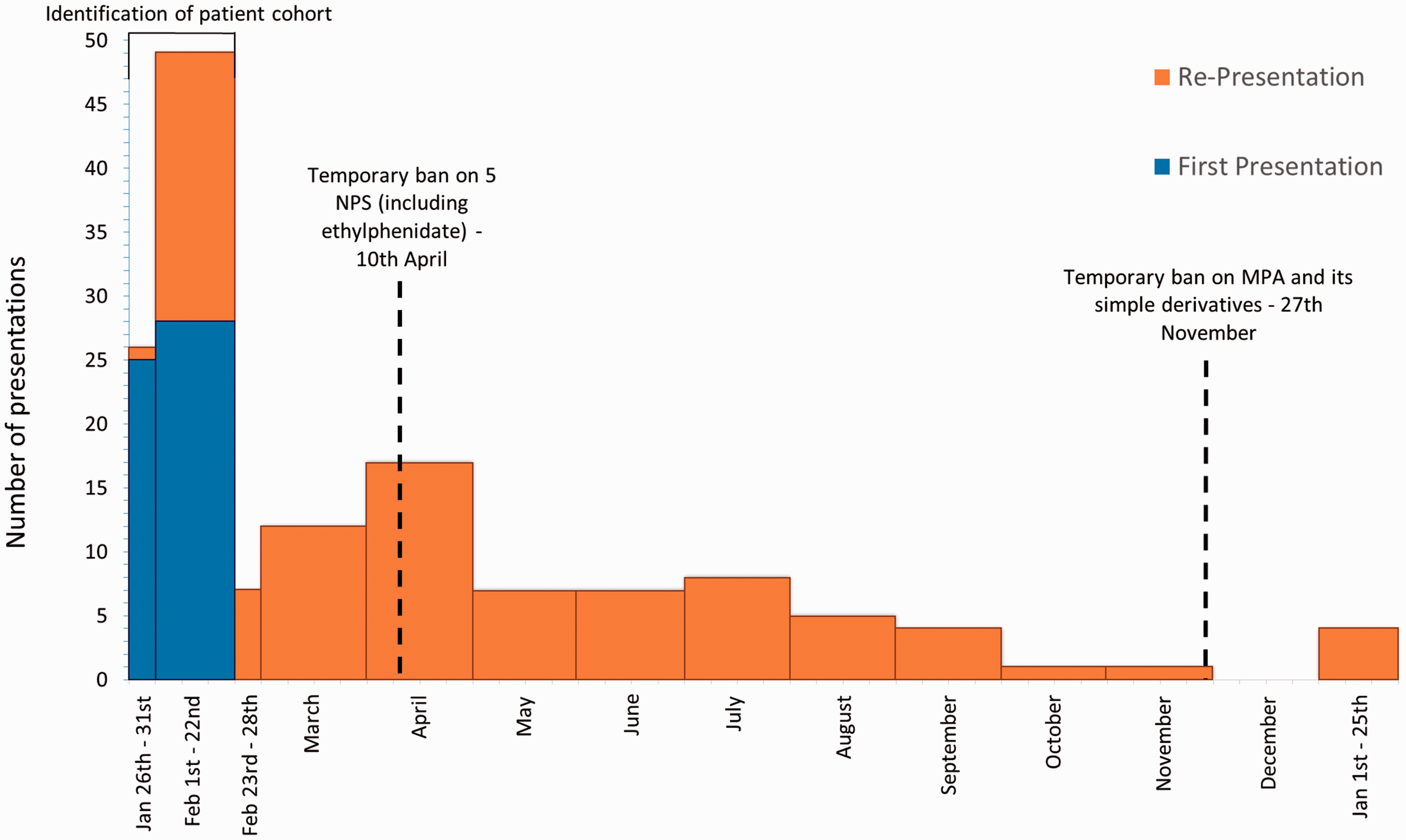
Presentations of NPS users who presented to ED over an initial 4-week period (blue) and presented again (orange) over the course of 1 year. Dashed lines indicate the respective bans of notable NPS (ethylphenidate 11 and MPA 12 ), which frequently featured in the study. NPS: novel psychoactive substances; ED: emergency department; MPA: methiopropamine.
Presenting complaints varied, and most often involved behavioural change (31% – largely confusion or paranoia), collapse/reduced GCS (26%), infection (21%), pain (19%) and trauma (3.4%). The most common method of drug use was by injection (72.3%).
NPS agents recorded in hospital notes associated with an ED presentation.
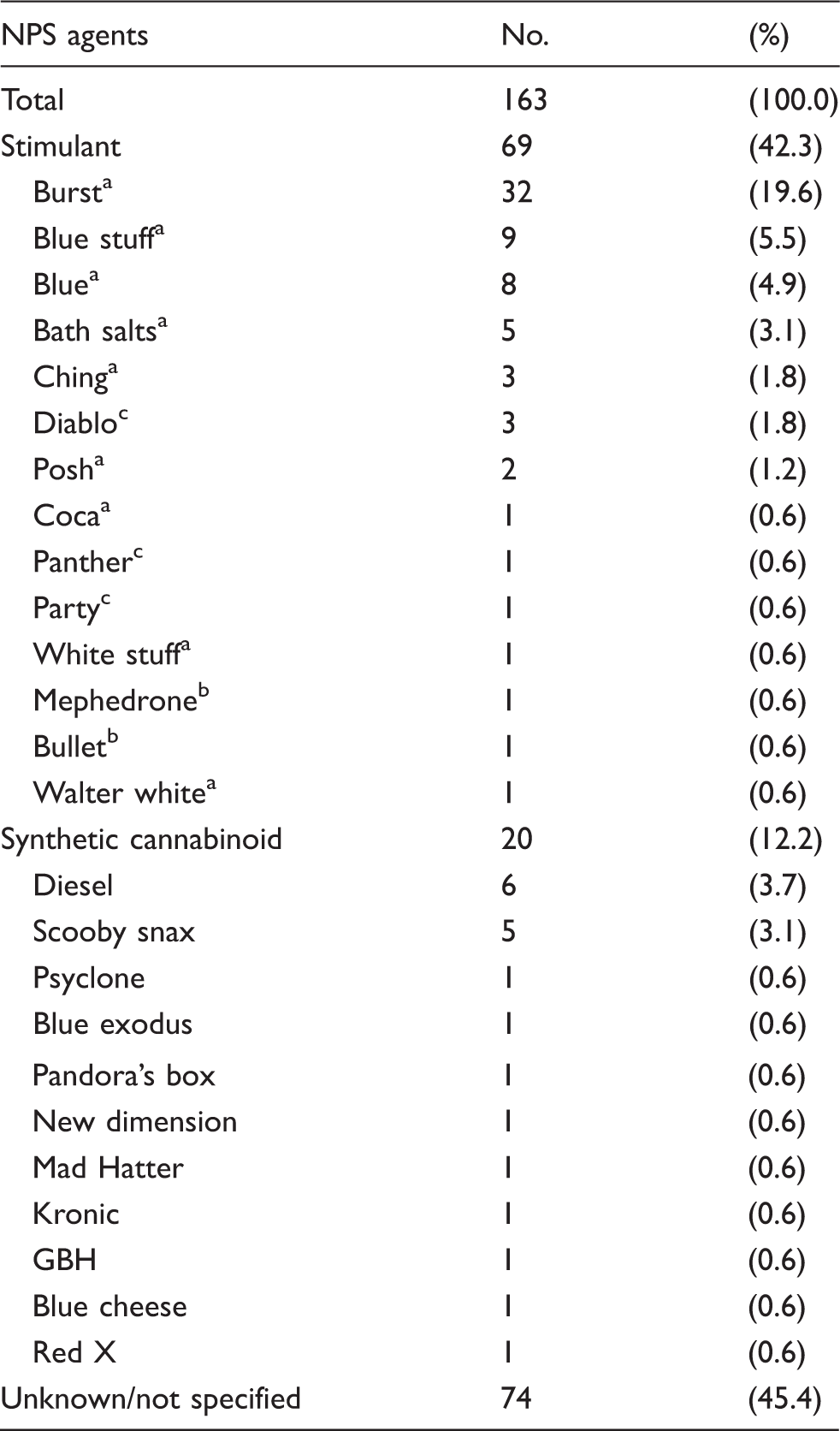
Agent is known to or likely contains ethylphenidate.
Agent contains MPA.
A suspected stimulant, but the chemical compound is not known.
NPS: novel psychoactive substances; ED: emergency department.
A number of patients presented after smoking synthetic cannabinoids with significant physical and psychiatric signs and symptoms. These included dyspnoea, arrhythmias and episodes of psychosis or suicidal ideation. Similar associated symptoms have been described previously. 13 Presentations associated with stimulant use were notably associated with behavioural problems similar to the psychosis and violent behaviours that have been reported with synthetic cathinone use. 5
The time spent in hospital of a patient population of NPS users who presented over a 4-week period (n = 53) in addition to their subsequent presentations deemed related to NPS use over the following 11 months.
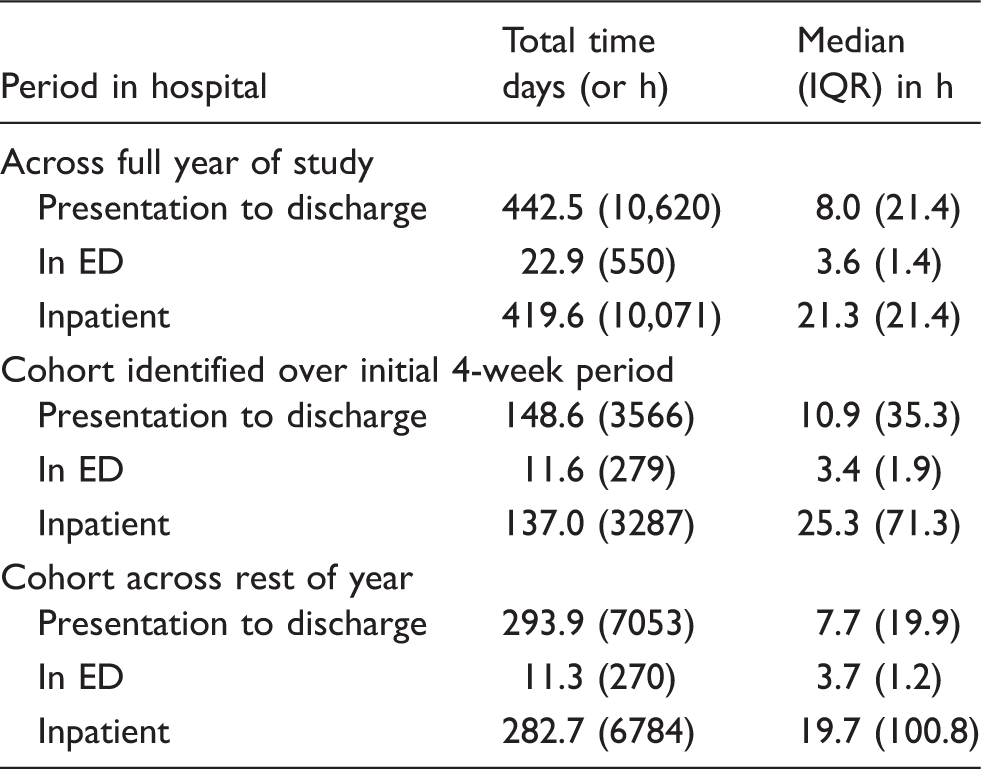
Median used considering presence of outliers.
NPS: novel psychoactive substances; IQR: interquartile range; ED: emergency department.
Discussion
Many might consider the age of patients presenting during the study a surprising finding, and this has important implications for public health. Campaigns aimed at NPS users may not be targeting the most appropriate audience. Much of the current literature describes NPS use as if it were almost exclusively a young people’s problem,8,14,15 with a recent 2015 UK government campaign targeting 11- to 18-year-olds. 16 Several surveys investigating the use of NPS have identified the highest use among younger people and club/festival goers, rather than the general adult population.1,17 Although the use of NPS among younger people is not disputed, our study suggests that the patient population may be older. This may reflect a limitation of surveys, often administered online, which may neglect users who are older or socioeconomically deprived. 14 In our study, only one patient (aged 17) from 53 was under 18; our findings question whether the population targeted by police initiatives is representative of the patient population. 16
In addition to this age disparity, our study identifies common characteristics in the population, including previous or current illicit drug use and having no fixed abode. Our subjects thus come from a vulnerable group in society, perhaps more susceptible to presentation to secondary care than healthy teenagers and young adults who occasionally use the drugs in a set social scene, such as a nightclub. This ‘vulnerable demographic’ may also be more likely to inject NPS and hence suffer the injection-specific adverse effects such as injection-site infection or inflammation. This is plausible as episodes of homelessness are associated with injection of traditional illicit drugs. 18
The age of NPS injectors in Lothian 19 strongly mirrors that of the patients in our study; hardly surprising given the predominance of intravenous (IV) use previously found in our patients. Age-related differences in method of use may exist; however, we did not find a significant difference in mean age between those who injected (34.9 years ± 7.9 SD, n = 39), or smoked (27.6 years ± 11.13, n = 9) NPS in association with their first presentation (unpaired t test with Welch correction t(9.95) = 1.86, p = 0.09). That said, overlap between groups may have masked differences and those who used NPS orally were too few in number for comparison. The prevalence of IV use may relate to an associated high frequency of use, and hence increased risk of harm, with 52% of those attending a Lothian needle exchange typically injecting at least once per day. 19
In view of previous opioid use, several patients had ongoing receipt of methadone prescription. Their concurrent use of NPS, not routinely screened in urine drug testing, may suggest sub-optimal opioid replacement or may potentially result in interactions and overdose. 20
Presenting complaints due to infection were common – most notably involving Staphylococcus aureus and Streptococcus pyogenes, in both of which IV transmission is implicated. 21 Almost all infections were at the sites of injection, resulting in cellulitis or abscess formation. Health care professionals should be aware of high rates of infection with hepatitis C among these patients, accounted for by a high incidence of previous IV drug use, and hence should treat them all with care and with consideration of personal protective equipment.
Current literature4,22 suggests that two thirds of NPS use involves drugs of the synthetic cannabinoid and cathinone classes, with cannabinoid use slightly higher. Conversely, in this study, stimulants appeared to outnumber synthetic cannabinoids (42.3% versus 12.2%) though a large number of agents were unknown (45.4%). The predominance of stimulants featured may relate to their tendency to be injected, leading to complications requiring ED attendance, or may suggest differing patterns of use in Lothian, with relatively high rates of stimulant and/or IV use.
The most common named NPS in our study population was Burst (36.0% of total named). This substance contains the stimulant ethylphenidate, which was placed under a temporary class drug order – a 12-month ban while awaiting further review – alongside four other substances on 10 April 2015.11,19,23 Injection of ethylphenidate is a trend beginning in Lothian in 2014 with significant adverse effects on health. 19
Over the study period, re-presentations to ED related to NPS use decreased (see Figure 1), and the timings might suggest the ban contributed to this. That said, one can’t entirely differentiate between reduced usage and reduced reporting. It is possible that the graph displays the natural course of re-presentation rates independent of legislation. It is notable that ethylphenidate continued to feature after its prohibition (10 presentations) suggesting that the drug was still accessible though possibly not to the same extent.
Over the year, the 53 patients spent a collective total of > 10,500 h in hospital – approximately 440 days (see Table 3). This might suggest an extensive use of hospital services, which may be preventable. Our study also identified a large subgroup of patients presenting with soft tissue damage (resulting in infection or pain) that required subsequent and even specialist treatment (vascular surgery).
Recommendations for improving patient care could include early involvement of the substance misuse team, screening for blood-borne viruses, and an additional code (a label which classifies diagnoses, symptoms and procedures for healthcare purposes) 24 for IV drug-using patients.
Our study was limited by the quality of the history taken in ED. Certain histories may be less accurate owing to intoxication on presentation or poor compliance with interview. Secondary accounts from witnesses, such as police, were also used. As polysubstance and illicit drug use were common, these may have confounded findings including presenting complaint.
As a single centre study, the generalisability of findings beyond Lothian is debatable. However, the demographic identified here may be common to many urban EDs that cater for large populations of injection drug users where NPS have replaced traditional drugs.
Conclusion
This study identifies a mismatch in the demographics of patients who present to hospital with complications related to NPS use and the younger populations commonly targeted by government and police strategies. Patients are much older than expected and are very often ex- or current IV drug users with high instances of psychiatric illness, methadone prescription and homelessness. This study also suggests that the NPS using population in Lothian, who present for related ED treatment, are most often using stimulant-type NPS, such as ethylphenidate, and using them by injection.
Footnotes
Authors’ contributions
DEH, CWDI, SRM, BW, RAB, SMM, SLC and ER contributed to the project design, review of notes, data collection and provisional manuscript draft based on the initial 4 weeks of data collection. DEH, CWDI and SRM extended the project design to 1 year and performed the related data collection, analysis and production of a final manuscript. All authors approved submission.
Acknowledgements
We would like to thank Dr Nicola McCullough and Dr Graeme McAlpine for their guidance during the planning and development phase of this project and all ED staff at the Royal Infirmary of Edinburgh for their help identifying patients and recording information. We would also like to thank staff members involved with the organisation MyCrew for their help in NPS classification.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Local University of Edinburgh.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.