
Abstract
Background and aims
Indiscriminate coagulation testing in emergency general surgical patients can lead to inappropriate delay in surgery, cause unnecessary concern and is associated with significant cost. The British Committee for Standards in Haematology recommends against coagulation testing to predict peri-operative bleeding risk in unselected patients. Our aim was to assess the appropriateness of coagulation tests performed in emergency general surgical patients and evaluate the effect of a series of educational interventions on clinical practice.
Methods and results
Appropriate indications for performing coagulation testing included a positive bleeding history, the presence of liver disease/cholestasis, sepsis or use of anticoagulants. Initial data on 142 patients were collected over 2 weeks of receiving. Following analysis, indications for appropriate coagulation testing were highlighted and data were collected on a further 190 patients. Comparing the audit cycles, we observed a decrease in the proportion of patients who underwent routine testing (49.3% vs 32.6%; p = 0.002) and inappropriate testing (67% of tests vs 34% of tests; p < 0.001). Despite being highlighted, there was no evidence of improved documentation of bleeding histories on admission.
Conclusions
This observational study suggests that simple educational messages can reduce the inappropriate use of coagulation screening tests in general surgical emergencies. This seems to result from clarification of the appropriate surgical indications for coagulation testing in this group.
Introduction
Bleeding is a recognised and feared potential complication of surgical procedures. Bleeding in the peri-operative period is associated with poorer outcome for patients, increased use of resources such as blood transfusion and an increased need to return to theatre or perform alternative procedures to control bleeding.1,2 There is a long held general perception that screening tests of a patient’s haemostatic system may allow identification of those who are at risk of peri-operative bleeding. However, there is very little evidence to support this assumption. 3 There are several good reasons for the apparent lack of correlation between routine coagulation test results and the bleeding outcome of patients with surgical presentations. These include the limited sensitivity and specificity of the routinely used tests, the prothrombin time (PT) and the activated partial thromboplastin time (aPTT), to fully inform on the risk of bleeding. 3 In addition, our understanding of the trigger factors for bleeding has improved. For example, in advanced liver disease, bleeding is most often triggered by sepsis or volume overload rather than by any change in an often chronic coagulopathy. 4 Likewise, in major trauma, our improved understanding of the risk factors for bleeding has resulted in the broadly accepted policy of permissive hypotension and the widespread use of the anti-fibrinolytic drug – tranexamic acid. 5
Routine coagulation testing in surgical units typically involves measuring the PT and aPTT, with many laboratories also, inappropriately, reporting an International Normalised Ratio (INR) in patients who are not on warfarin or other coumarin. In these circumstances, the tests are used as a screening tool to purportedly assess and predict an individual’s risk of bleeding. However, this process is not evidence-based and is somewhat misguided for several reasons. First, coagulation tests were originally developed to aid in the diagnosis of inherited coagulation factor deficiencies and were not intended as a screening test to predict bleeding. 6 Second, the PT and aPTT are not sensitive or specific for the range of bleeding disorders that they are assumed to cover. 7 So, a normal coagulation test does not exclude the risk of bleeding and a prolonged test does not necessarily predict bleeding. Examples of this include the failure of the PT and aPTT to identify patients with Von Willebrand disease (the commonest inherited bleeding disorder), factor XIII deficiency and platelet function disorders (including acquired defects commonly due to the use of anti-platelet medications such as aspirin, clopidogrel and ticagrelor).3,6 This is because the PT and aPTT do not provide any information on clot stability, fibrinolysis, platelet dysfunction or the function of von Willebrand factor. 3 Conversely, prolongation of the PT and aPTT has a low specificity for predicting bleeding. 6 This is illustrated by the absence of bleeding in situations where significant prolongation of the aPTT occurs such as the presence of lupus anticoagulant or factor XII deficiency. Of particular relevance to emergency surgical referrals, the PT and aPTT are altered by acquired patient factors such as pH and temperature. Possibly of most relevance, increasing CRP level produces a linear prolongation of the aPTT. 8 Finally, some healthy individuals may have clinically insignificant abnormal results, accounted for by the normal distribution of coagulation times whereby they fall just outside two standard deviations from the mean normal value. 8 Stand-alone coagulation screening therefore may result in false reassurance (false negative tests) and in false positive tests that generate delays, anxiety and further investigation.
Furthermore, coagulation testing has significant cost implications. At NHS Grampian, a full coagulation screen costs £4.50 and an INR £1.50. The laboratory receives about 5000 and 1500 such test requests, respectively, amounting to a cost of around £25,000 per month.
Based on a systematic review of reasonable quality studies, the British Committee for Standards in Haematology (BCSH) recommend against the use of coagulation screening tests to predict peri-operative bleeding risk in unselected patients. 9 This is supported by the NICE guidelines of 2016. 10 A structured bleeding history, which includes family history of coagulation disorders, personal history of abnormal bleeding and concomitant use of anti-thrombotic medications is suggested to be of more value in predicting the risk of bleeding.3,9,11
The aim of this study was to assess the appropriateness of coagulation tests performed on patients admitted through emergency general surgery at Aberdeen Royal Infirmary (ARI), based upon the recommendations of the BCSH, and to measure changes in practice following an educational intervention within the department.
Methods and materials
Study population
A closed audit loop of patients admitted to the emergency general surgical department at ARI was performed. Two periods of surgical emergency receiving each consisting of two separate weeks were studied. The General Surgery Department at ARI deals with approximately 70–120 emergency admissions per week. Referrals come from a variety of sources such as general practice and the emergency department. Consecutive emergency surgical patients, aged more than 16 years, admitted during the study periods were included. Elective patients and patients referred from other wards were not included in the study.
Definitions
The BCSH guidelines recommend against indiscriminate coagulation screening prior to surgery or other invasive procedures, suggest the completion of a bleeding history to include the current use of anti-thrombotic medication and recommend testing where there is a clear clinical indication such as liver disease or other disorders commonly complicated by coagulopathy. 9 In our study, appropriate coagulation testing was defined as a test performed on patients fulfilling any of the following criteria: having a positive bleeding history (defined as a personal or family history of coagulation disorder), currently taking anti-thrombotic medication, with liver disease or cholestasis defined by raised bilirubin (>50 µmol/L), sepsis or the need for an interventional radiological procedure. Inappropriate coagulation testing was defined as any test performed, which did not adhere to the above criteria. In cases where a bleeding history could not be found in the record, it was assumed that it was either negative or had not been completed. Because these patients therefore did not have a documented positive bleeding history, there was no indication for testing based on this part of the clinical presentation and so the appropriateness of testing was based on the surgical presentation alone.
Outcome measures
Outcome measures included the total number of tests performed, the number of inappropriate tests performed and the number of repeat tests performed. Evidence of a bleeding history was sought from the patients’ electronic record.
Study design and data collection
Each audit cycle consisted of 2 weeks of prospectively collected emergency receiving patient information. The local patient management system, TrakCare, was used to gather relevant information. The data collected were age, gender, presenting complaint, bleeding history, anti-coagulant or anti-platelet therapy, presence of jaundice (defined as bilirubin >50 µmol/L), operations performed and number of coagulation tests performed. Data were collated and analysed from an Excel sheet.
Intervention
The first cycle (Cycle 1) was between November and December 2015. The second cycle (Cycle 2) was between September and October 2016.
The results from the first cycle were disseminated at a unit quality improvement meeting attended by all hospital medical professionals managing emergency surgical patients. It was then presented as a poster at a local general surgery symposium, attended by large numbers of the unit’s staff. A laminated information sheet listing the main findings and the indications for appropriate coagulation tests was distributed to all four wards and advertised verbally by the authors working in the department at the time (see Appendix 1). Additionally, this was emailed to the entire medical staff (physician associates, foundation doctors, registrars in training, clinical development fellows, education fellows and consultants) of the surgical department. This was repeated at the time of trainee change-over periods.
Following these educational interventions, the equivalent data were collected for the second cycle to complete the cycle.
Statistical analysis
The population was described using descriptive statistics. Comparisons between the groups were made using Pearson’s Chi-square test, IBMSSPS version 24. p values of <0.05 were considered significant.
Results
Patient characteristics
Patient demographics of the two cycles.
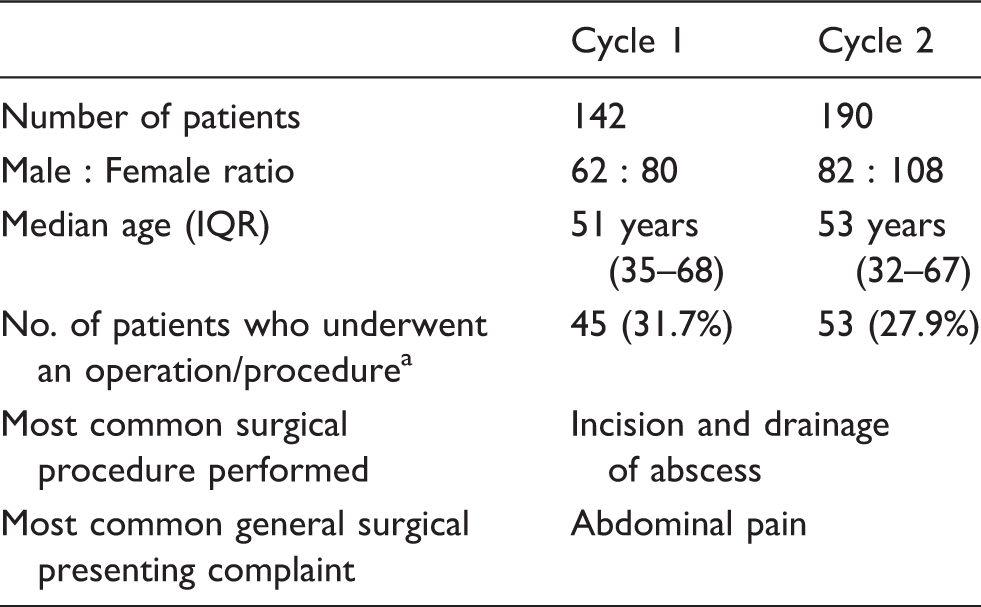
Operation – Open and laparoscopic surgeries; procedures – incision and drainage, ERCP (Endoscopic Retrograde Cholangio-Pancreatography) and interventional radiology techniques.
IQR: interquartile range.
Coagulation test ordering
Coagulation testing.
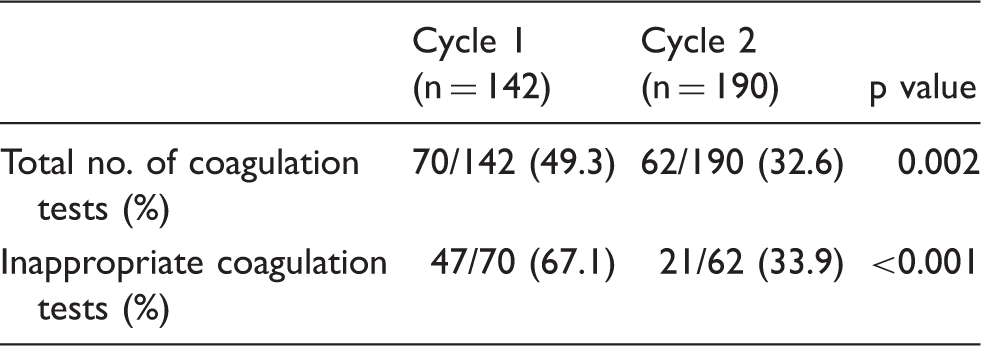
There was a significant reduction in the proportion of tests defined as inappropriate in Cycle 2 (Cycle 1 : 47 of 70 (67.1%) versus Cycle 2 : 21 of 62 (33.9%); (p < 0.001)).
Repeated coagulation testing was similar in the two cycles (Cycle 1 : 28 of 70 patients (40%); Cycle 2 : 21 of 62 patients (33.9%)). However, 16 of 28 (57.1%) repeat tests in Cycle 1 were defined as inappropriate compared to 2 of 21 (9.5%) repeat tests in Cycle 2 (p = 0.003).
Bleeding history
A bleeding history consists of family or personal history of bleeding or coagulation disorder, but no obvious record of this was evident in any case records of either cycle. Apart from the documentation of the use of anticoagulants, the completion of a bleeding history was thus very poorly performed in both cycles.
The use of anti-thrombotic drugs however was documented in all patients (8/142 in cycle 1 and 12/190 in cycle 2). In cycle 1, all eight patients on anti-thrombotic medication had coagulation tests performed, compared to 11/12 in cycle 2. One patient on warfarin had no coagulation tests performed during their admission.
Operative and interventional outcomes
Forty-five of 142 patients in cycle 1 and 53 of 190 patients in cycle 2 had some form of surgical intervention. Of these, 27/45 patients in cycle 1 and 18/45 in cycle 2 had coagulation testing. Coagulation tests were also performed on 43/97 patients in cycle 1 and 44/137 patients in cycle 2 who did not go on to have an operative procedure. This finding further demonstrates the indiscriminate use of tests, which were clearly seen to be a routine part of the admission process. During the study period, there were no reported episodes in either cycle of unexpected coagulopathic bleeding during any operative or interventional procedure.
Discussion
Many surgical units in the UK perform indiscriminate coagulation testing on emergency patients. To the best of our knowledge, this is the first closed loop audit investigating both the appropriateness of coagulation testing in such patients, and the response to training sessions highlighting these issues. Using current BCSH guidelines to define appropriate practice, the first cycle identified tests performed in patients who had no indication based on their clinical presentation. Following multi-modal education of staff, the second cycle demonstrated a significant reduction in coagulation tests performed (total and inappropriate) without an apparent increase in abnormal or unexpected bleeding episodes. Family bleeding history or personal history of excessive bleeding was not well documented in either cycle.
There is a paucity of data in this area. One study did look at coagulation testing in Accident and Emergency and demonstrated a reduction in the number of inappropriate requests from 82.1% (303/369) to 28.9% (28/97) following team education and the removal of coagulation tubes from the main emergency area. 12
In our study into the management of admitted surgical patients, we also demonstrated a significant reduction in inappropriate coagulation testing following the provision for staff of a multi-modal education programme. It is not clear which component of the programme contributed most, but the results suggest that it is improved attention to the presence or absence of a clinical indication that has produced the outcome. The majority of coagulation test requests in the surgical department are made by foundation year doctors (FY). The overall improvement in requesting coagulation tests suggests that FY trainees have adopted this selective policy of ordering coagulation tests. It was also observed, anecdotally, that senior colleagues began to encourage junior trainees to be more selective in ordering coagulation tests after the educational intervention. If senior surgeons feel comfortable reducing the number of tests performed, this may be more likely to result in a permanent change in behaviour of the junior doctors in their unit.
We also noticed fewer full coagulation tests (PT, APTT, INR) and more INR only requests in cycle 2 compared to cycle 1. In cases such as warfarin monitoring, only the latter is required. Though not an outcome measure, the predicted cost savings by using selective coagulation testing would be significant.
The documentation of patients on anti-thrombotic medication was done well in both cycles. However, no evidence of a bleeding history was documented in either cycle on review of TrakCare. To try and improve practice, the importance of tailoring coagulation tests to each patient and taking a bleeding history is now emphasized at the start of the mandatory induction for all general surgical foundation year doctors. Auditing the documentation of a bleeding history in patient notes is something that could be studied in future.
Limitations of the study include its small sample size and its single-centred nature. Although we identified the numbers of patients tested and were able to comment on the appropriateness of that, we did not identify patients who should have been tested but were not. However, this study is one of the first to describe the outcomes of an educational programme for appropriate coagulation testing in emergency general surgical patients.
Conclusion
Using a guideline-based selective policy for coagulation testing in emergency general surgical patients, this closed loop audit has demonstrated a significant reduction of overall and inappropriate tests performed without an increase in abnormal bleeding episodes. Our study was unable to assess the number of patients in whom testing was indicated but not performed but did reveal a deficiency in taking or documenting a bleeding history. However, we feel our multi-modal approach to educate surgical staff about the appropriateness of testing has led to promising results.
Footnotes
Acknowledgement
Many thanks to Paul Drew, Senior Chief Biomedical Scientist/Haematology Laboratory Manager, Aberdeen Royal Infirmary, for providing data on cost of NHS Grampian coagulation screen.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.