
Abstract
Thrombotic thrombocytopenic purpura is a rare condition that presents with microangiopathic haemolytic anaemia, thrombocytopaenia, fever, renal impairment and neurological symptoms. Plasma exchange is a lifesaving treatment for this condition. However, some cases may be non-responsive to plasma exchange, or loss of response may occur. Treatment options for refractory cases include high-dose corticosteroids, rituximab, vincristine, cyclophosphamide, splenectomy, bortezomib and N-acetylcysteine. We present a refractory case of thrombotic thrombocytopenic purpura responding to the last of these therapies.
Introduction
Thrombotic thrombocytopenic purpura (TTP) is a thrombotic microangiopathy caused by severely deficient activity of a disintegrin and metalloprotease with a thrombospondin type 1 motif, member 13(ADAMTS13) which cleaves multimers of von Willebrand factor (vWF). 1 There are two forms of TTP, congenital and acquired. In congenital TTP, mutations exist in ADAMTS13 protein coding genes, while in acquired TTP, there occurs the development of anti-ADAMTS13 auto-antibodies that block enzymatic activity.2,3 Primary treatment modes in acquired TTP are plasma exchange (PE) and corticosteroids. Mortality rates decreased from 90% to 10% with PE. 4 According to the American Society for Apheresis consensus conference in 2012, response is defined as achieving a platelet count of 150,000/mm3 for two consecutive days, a normal or near normal lactate dehydrogenase (LDH), and stable or improving neurologic deficits. 5 Refractory TTP is defined in the literature as an absence of platelet response or loss of clinical deterioration after four to seven days of PE treatment or relapsed within the first 30 days of stopping PE. 6 Relapsed TTP is considered as recurrence of thrombocytopenia, and microangiopathic haemolytic anaemia (MAHA) 30 days after treatment response is achieved. The incidence of patients who do not respond to PEX and corticosteroids and require additional therapy varies between 10% and 42%.7,8
We report a patient whose TTP became refractory at second relapse and who was successfully treated with PE, high-dose methylprednisolone, rituximab, vincristine and N-acetylcysteine.
Case
A 29-year-old female presented one day after delivery by Caesarean section (for foetal distress at 34 weeks) of a healthy baby. She was admitted to the clinic with TTP pre-diagnosis based on anaemia and thrombocytopenia detected in routine tests before delivery. She was complaining of consciousness change and blurred vision. She was noted to be confused and had unequal pupils. Her medical history revealed that she was initially diagnosed with TTP in 2009 and was treated with plasmapheresis. She had TTP recurrence in 2011 following a pregnancy and was successfully treated with plasmapheresis alone. The laboratory studies showed haemoglobin (Hb) of 7.3 g/dL, platelet count (plt) of 9000/mm3, LDH level of 1947 U/L (N: 125–220 U/L), indirect bilirubin level of 2.1 mg/dL (0.3–1 mg/dL), reticulocytosis, haptoglobin level of < 8 mg/dL (40–240) and negative Coombs test. Diffuse fragmented erythrocytes were observed on peripheral smear. Plasma ADAMTS13 activity was 1.69% (>10%) and inhibitor level was 12.04 U/mL (<12); the patient was diagnosed with relapsed TTP.
Plasmapheresis with 1.5 plasma volume and 1 g/day of methylprednisolone (planned for three days) was started. Confusion and anisocoria improved on treatment day 3 and platelet count was increased to 37,000/mm3. On day 5, platelet count was 126,000/mm3 and LDH had reduced to 429 U/L. Despite continuing plasmapheresis treatment, on day 8, the haemoglobin fell to 7.4 g/dL and platelet count to 17,000/mm3, while LDH was increased at 1350 U/L (Figure 1). Frequency of plasmapheresis was increased to twice daily while weekly 375 mg/m2 rituximab and weekly 2 mg vincristine were added to the regimen. A response was achieved with this treatment. On day 25, LDH was reduced to 274 U/L and platelet count improved at 156,000/mm3. Rituximab and vincristine were given for four weeks and then both stopped at the same time.
Course of platelet count and LDH.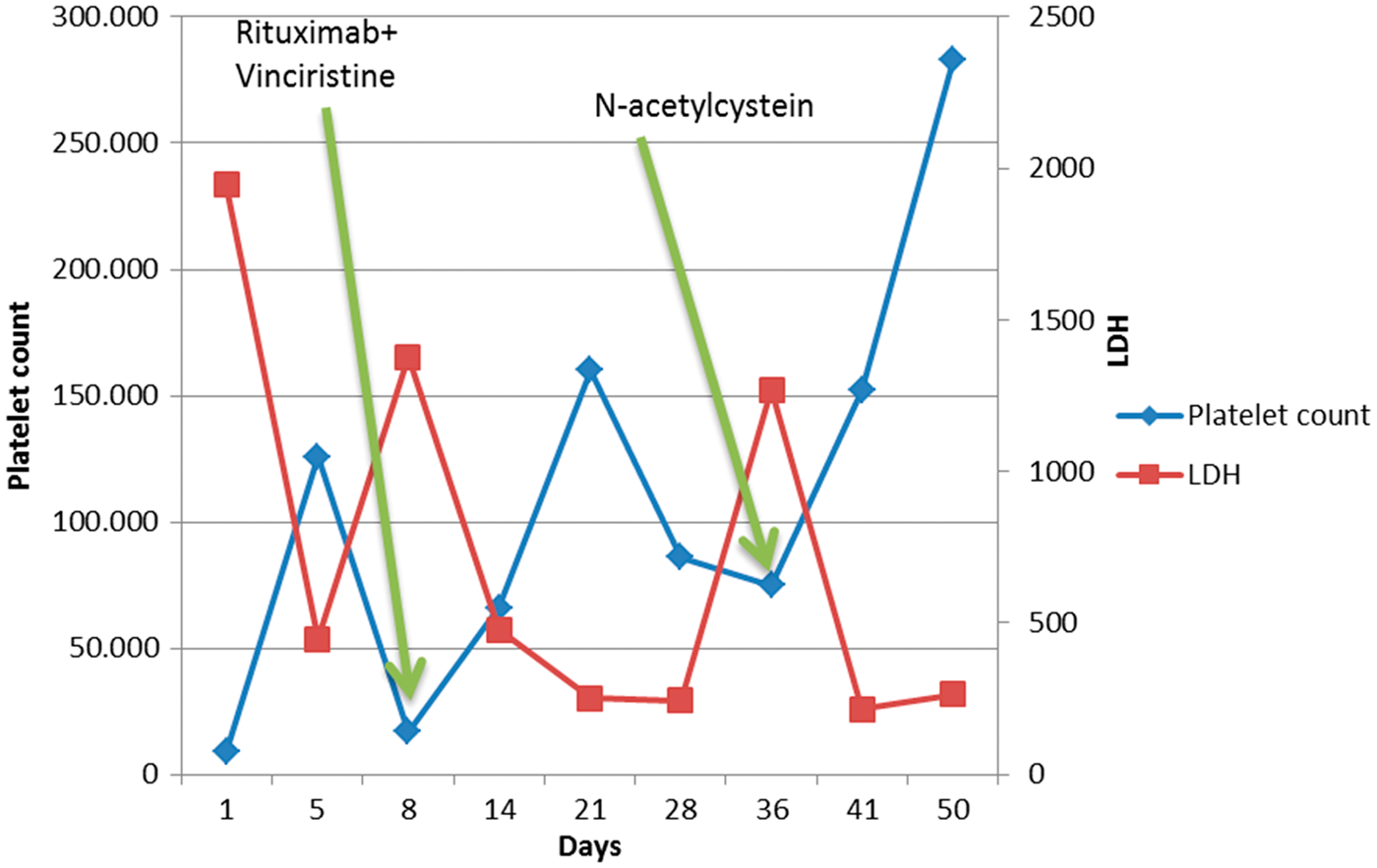
However, despite continuing plasmapheresis twice daily, the platelet count decreased progressively, reaching 75,000/mm3, and LDH began to increase after day 28. Peripheral smear assessment confirmed that the platelet count was low. The patient developed confusion again. In the presence of these findings, this was diagnosed as a further relapse of the disease. On day 36, the patient began 10 g of N-acetylcysteine parenterally daily for five days, and PE was reduced to one session per day, considering that there was not enough response. The platelet count improved to 152,000/mm3 on day 5 of N-acetylcysteine treatment and LDH reduced. Initially, plasmapheresis was further reduced to once every two days and then discontinued, since no reduction of platelet count was observed while the patient was followed up for one week. After one week of no-treatment period, the patient was discharged with platelet count of 285,000/mm3 and LDH of 265 U/L (Figure 1).
The patient remains in remission after six months follow-up at the outpatient clinic.
Discussion
Relapsed TTP is usually expected to respond to the previous treatment regimen. However, refractory cases may occur, with poor response to these regimens, and more intensive treatment is required. The regimen recommended in refractory TTP is 1 g of methylprednisolone for three days and rituximab (375 mg/m2/week) on four occasions, in addition to plasmapheresis. 9 If a response cannot be obtained with this combination, other treatment options include vincristine, cyclophosphamide, bortezomib, cyclosporin, mycophenolate, N-acetylcysteine (NAC) or splenectomy.
The clinical use of NAC in the treatment of TTP has rarely been reported. Studies in vitro and in TTP animal models have shown NAC to reduce ultra-large vWF multimer concentrations.10,11 This may suggest a possible mechanism for a beneficial effect in subjects with acquired TTP. In one case report, complete remission was achieved by adding NAC (150 mg/kg daily for 10 days) to the regimen of a TTP patient refractory to plasmapheresis, glucocorticoid and rituximab. 12 Rottenstreich et al. reported that three patients with TTP had a complete remission by adding NAC to the treatment. When these three cases are examined, it seems that, unlike our case, NAC was administered simultaneously with plasmapheresis and immunosuppressive treatments. One patient is described as having a good response. In the other two cases, it is not clear which treatment is beneficial. 13 In a case reported by Acedillo et al., no response was obtained to NAC. 14 In our case, remission was obtained with concurrent plasmapheresis, rituximab and vincristine treatment. However, once rituximab and vincristine treatment were completed, recurrence developed when plasma was maintained twice a day after one week. At this stage, plasmapheresis was reduced to once daily, and NAC 150 mg/kg (five days) alone was started. After five days of NAC treatment, a complete remission was obtained. Recurrence after administration of plasmapheresis twice daily and adequate dose and duration of immunosuppressive treatment strongly suggests that this response was obtained with NAC therapy.
In conclusion, although plasma exchange is considered lifesaving in TTP, refractory cases may remain unresponsive to PE and the condition can be fatal. Other options clearly must be considered in such cases. In patients unresponsive to high-dose corticosteroid and rituximab regimen, NAC, which is less toxic than cyclophosphamide and other chemotherapeutics, may be considered, perhaps even before these treatments.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.