
Abstract
The effects of high altitude on the human vascular system are well described. This case demonstrates an interesting combination of vascular complications at high altitude which were both life- and sight-threatening. In May 2017, during an attempt on Mount Everest, a 58-year-old man was forced to descend from 8000 m because of adverse weather. He suffered significant frostbite of his right hand, later requiring termination of the distal phalanx of one of the affected digits. He also experienced increasing breathlessness and went on to develop pleuritic chest pain. A CT pulmonary angiogram performed upon return to sea level revealed multiple small sub-segmental pulmonary emboli. He was anticoagulated for three months and made a full recovery. The patient also reported visual loss in the left eye and on ophthalmic examination was found to have multiple retinal haemorrhages including a left macular haemorrhage, consistent with high altitude retinopathy. The retinal haemorrhages settled with conservative management. The vascular complications suffered by this patient demonstrate the potentially fatal changes that can occur at altitude. They also serve to act as a reminder for physicians, even at sea level of the potential complications in patients returning from high altitude.
Introduction
The effects of high altitude on the human vascular system are well described. 1 Some are acute and self-limiting, whilst others are significant and potentially fatal. A pulmonary embolism in any setting warrants urgent diagnosis and management. Frostbite can lead to significant morbidity, including loss of affected tissue. High altitude retinopathy (HAR) can cause loss of vision if there is macular involvement, although it usually carries a good prognosis and is typically managed conservatively.
This paper describes a patient who suffered all three of these conditions during an attempt on Mount Everest. This particular combination of vascular complications at high altitude was both life- and sight-threatening and in combination has not been previously described in the literature.
Case report
During an ascent of Mount Everest in May 2017, a 58-year-old was forced to suddenly descend from approximately 8000 m owing to a storm. Whilst descending, he became separated from his group and depleted the oxygen within his tank. Despite this, he eventually made it down the mountain to sea level approximately 27 h later.
During this ordeal, he noticed that the vision in his left eye was blurred, and that he was experiencing significant breathlessness, both of which continued even after descent to Kathmandu (1400 m). Moreover, he described how the terminal regions of his ring and little fingers of his right hand had become significantly discoloured and swollen. Whilst still in Nepal, a chest radiograph revealed right basal lung consolidation and he was commenced on co-amoxiclav for presumed pneumonia. Despite antibiotic treatment, his chest symptoms worsened and he presented to the Emergency Department on his return home to the UK.
By this time, he had a one-week history of worsening breathlessness and a dry cough, right-sided pleuritic chest pain and total visual loss in his left eye. Other than having corrective surgery for a right strabismus as a child, he had no other ocular, medical or surgical history. He was a non-smoker and did not take any regular medications.
Clinical observations were as follows: oxygen saturation of 100% on air, pulse rate 80 beats per minute and respiratory rate 18 breaths per minute. He appeared comfortable at rest. On examination, he had reduced air entry at the right base and his calves were soft and non-tender. He was found to have significant frostbite affecting the terminal phalanges of the ring and little fingers of his right hand, up to the distal interphalangeal joints.
Bloods of note were a C-reactive protein of 138 mg/L with a positive D-dimer (no actual figure was available from the lab); all other laboratory tests, including his full blood count and urine and electrolytes as well as a thrombophilia screen and an arterial blood gas were unremarkable. An ECG showed normal sinus rhythm with no abnormalities. Right basal haziness was present on his chest X-ray and a CT pulmonary angiogram revealed multiple small sub-segmental pulmonary emboli in the right lower lobe (Figure 1). A diagnosis of pulmonary embolism was made.
CT pulmonary angiogram showing a PE and a infarcted right lower lung lobe.
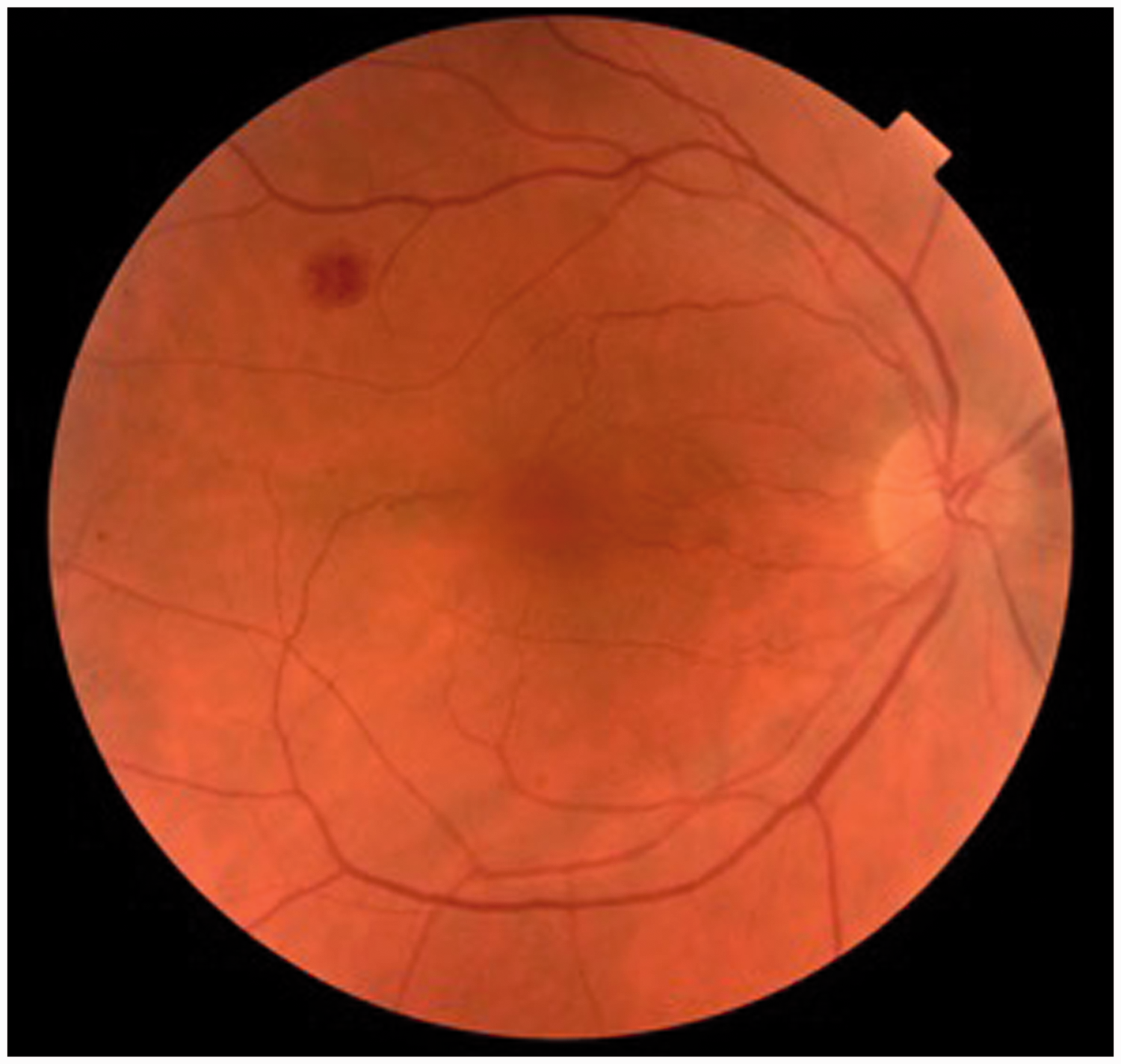
Ophthalmology review noted normal pupillary responses and visual acuities of 6/6 in his right eye, but ‘counting fingers’ only in his left eye. Fundoscopy showed a peri-papillary haemorrhage and a macular bleed in the left eye (Figure 2) as well as a peripheral superficial haemorrhage in the right eye (Figure 3) all confirmed on ocular coherence tomography and consistent with HAR. Intra-ocular pressures were 12 mmHg in both eyes.
High altitude retinopathy: Deep macular bleed and peri-papillary flame haemorrhage in the left eye reducing visual acuity to counting fingers. Superficial peripheral flame haemorrhage in the right eye. Visual acuity was 6/6 as there was no macular involvement. Stages of frostbite in this patient: A) initial skin dislocation and oedema post re-warming, B) re-perfusion of viable tissue, C) mummification and auto-terminalisation prior to surgical terminalisation.

The patient was commenced on apixaban for three months for his pulmonary embolism and his HAR was managed conservatively. He was seen two weeks after his initial presentation, at which point his visual acuity had improved to 6/12 in his left eye. At his three-month follow-up, this returned to 6/6 with complete resolution of the macular bleed in the left eye. The little finger of the right hand (figure 4) was managed conservatively and healed spontaneously without tissue loss. However, owing to pain and the presence of a necrotic area, amputation of the distal phalanx of the right ring finger was performed after the apixaban course had been completed.
Discussion
Our patient was given three diagnoses: pulmonary embolism, HAR and frostbite, all of which are likely to be related to his attempted ascent of Mount Everest. To our knowledge, these three diagnoses together have not previously been reported in a single case in the literature. We will discuss each of these conditions in turn and their relationship to the hypercoagulable state seen at altitude.
Pulmonary embolism at altitude
The reported occurrence of pulmonary embolism at altitude is rare, and to our knowledge has only been described in seven case reports.2–5 Its occurrence could be underestimated, as it may indeed be a cause of sudden death in trekkers, but as post mortems are infrequently carried out in such settings, there is no definite evidence for this. 2
With acclimatisation to the hypoxia of altitude, increased blood viscosity is seen due to haemoconcentration, polycythaemia and a rise in haematocrit. 4 This, added to the cold environment causing peripheral vasoconstriction and ‘sluggish’ blood flow, would seem to make thrombus formation more likely. However, the literature does not support a clear association between the risk of pulmonary embolism and altitude, although a prolonged stay at altitude may be a risk factor.4,5
High altitude pulmonary oedema (HAPE) is the most common pathology causing excessive breathlessness at altitude; pulmonary embolism, being less common, may be misdiagnosed as HAPE. Shortness of breath due to HAPE will usually settle quickly with descent and oxygen, whereas with pulmonary embolism, symptoms will likely persist. 4
If a patient remains symptomatic after descent, there should therefore be a high index of suspicion for pulmonary embolism, and a computed tomography pulmonary angiogram should be carried out. There is evidence that D-dimer levels rise in the absence of thrombosis with hypoxia and so its specificity will be reduced following exposure to altitude rendering its measurement less useful in the acute phase. 6 In this case, there was a delay in presentation and so d-dimer testing was indicated prior to computed tomography pulmonary angiogram.
In terms of patient investigations, a notable omission, which perhaps should have been carried out, was that of lower limb Dopplers. In a case series of pulmonary embolism at altitude, those suffering a pulmonary embolism tended to be aged >50 and had a deep vein thrombosis in the calves as the source of the thrombus. 4
If pulmonary embolism is suspected, urgent investigation and, if appropriate, prompt treatment is warranted to reduce morbidity and mortality.
HAR
At altitudes above 4000 m, HAR is common, but its precise incidence is unclear in the literature. 7 What is clear is that at 4000 m and higher, dilatation and tortuosity of retinal vasculature are considered to be a physiological response. 8 However, with further hypoxia, HAR – which is a pathological state characterised by retinal haemorrhages, cotton wool spots and papilloedema – may be seen. 9 Haemorrhages are typically located in the retinal nerve fibre layer and do not affect vision unless there is macular involvement.6–10 If vision is affected, no further ascent is advised until settled. HAR spontaneously regresses and is therefore typically managed conservatively. Several theories have been proposed as to why retinal haemorrhages occur. The most widely accepted is the autoregulation theory: compensatory mechanisms in the retinal vasculature, such as vasodilatation which serves to increase retinal blood flow, are initiated secondary to hypoxia.11,12 Risk factors for the development of retinal haemorrhages include extreme physical strain 13 and a higher baseline intraocular pressure. 14
Frostbite at altitude
The incidence of frostbite in mountaineers has been reported as 366/1000 life-times. 15 Cold induces peripheral vasoconstriction, thus reducing blood flow. The extremities do not have mechanisms for producing local heat (brown fat) and rely on warm blood from the core. To preserve core temperature, arteriovenous shunts open at the wrist and ankles, reducing warm blood flow to the hands and feet. Freezing of the skin and deep tissues distally ensues, commencing with the tips of the digits. Pallor, numbness, cold and oedema of the skin follows. 15 With increased time of exposure, tissue freezing spreads proximally. Cellular apoptosis due to crystal formation will occur. 16 The hypoxic environment will exacerbate this. 16
Frostbite at altitude appears to be commoner than for comparable environmental temperatures at lower altitudes. Cold and altitude both raise the packed cell volume and viscosity, which contribute to sluggish blood flow. In conjunction with cold negatively affecting the endothelium, there is also vascular leakage and oedema formation.
The priority for the patient is to rewarm the extremities (ideally in a water bath at 40℃) either in the field or in hospital. The freeze–thaw cycle must be avoided; therefore, thawed tissue must not be allowed to re-freeze. Aspirin (antiplatelet) and NSAIDs (antiprostaglandin) in combination should be commenced early in an attempt to prevent tissue necrosis. 17 Vasodilators, thrombolysis and hyperbaric oxygen are other medical therapeutic options in hospital. Surgery should be delayed to allow medical therapy to stabilise the tissue damage; otherwise, surgical debridement of necrotic areas is needed.
Altitude and the hypercoagulable state
Exposure to high altitude results in a hypercoagulable state. 18 Both venous and arterial thromboses are more likely to occur in patients with hypercoagulable states. However, when one considers other hypercoagulability and thrombosis risk factors, for example gender, obesity and diabetes, our patient had none. Raja and Mukhtar 19 reported a case in which, despite a negative thrombosis and thrombophilia screen, a 33-year-old soldier developed a central retinal vein occlusion after being deployed at an altitude of 3350 m for two years. Several factors at high altitude predispose to thrombotic disorders – namely hypoxia, dehydration, haemoconcentration, low temperatures, constrictive clothing, as well as severe weather enforcing stasis.18,20
One historic study carried out in rats found that blood coagulability was increased following exposure to extreme cold (i.e. cold injury) and that altitude acclimatisation temporarily aggravated the degree of the cold injury sustained. 21 Chohan et al. 22 found that in the early stages of frostbite, a coagulopathy was evident, and that the damage resulting from this intravascular coagulation could be potentially prevented by using dual antiplatelet and anticoagulant therapy.
At high altitude, all three elements of Virchow’s triad (stasis of blood flow, hypercoagulability and endothelial injury) are present. Interestingly, there has been some commentary suggesting that the triad should actually be a quartet to encompass hypoxia. 23 Rocke et al. 24 recently published a study in which they found that the proteome of platelets was altered by hypoxia, thus favouring a prothrombotic phenotype. Case reports of patients at altitude suffering various vascular events, including pulmonary embolism, suggest that the coagulation cascade is altered by hypoxia. 18
However, the evidence base is contradicting, limited 25 and lacks quantitative data. Our patient was at high altitude and was exposed to low temperatures. He battled and survived severe weather in the form of a storm and was likely hypoxic. It is clear that high altitude thromboembolic disorders are both complex in their aetiologies, multifactorial 17 and can have significant implications for mountaineers potentially death.
Conclusion
This case highlights that multiple changes can occur to the vascular system at high altitude that are both physiological and pathological; physicians at sea level should be aware of these possible diagnoses in patients returning from high mountain ranges. This patient had no pre-disposing conditions, such as clotting disorders, that put him at risk of vascular disease, and there was no indication from blood tests performed that his vascular system was compromised, but he still suffered three significant vascular complications from his attempt on Mount Everest.
Patient consent
Yes.
Footnotes
Acknowledgement
We thank our patient for allowing us to share his story.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.