
Abstract
Background
Increased availability of routine investigations results in significant over-investigation, burdening patients with unnecessary tests as well as increasing cost. We aimed to identify the extent of monitoring of liver function tests in lung resections, and to ascertain whether any impact on clinical decision-making occurred.
Methods
Cases were identified using theatre records coded as “lobectomy/bilobectomy” in the three-month period 20 June 2017 to 20 September 2017. Electronic records were used to collect patient data.
Results
A total of 91 cases were included; 77 (85%) patients had 1 set of pre-operative LFTs, 12 (13%) patients had 2 sets, and 2 (2%) patients had 0 sets; 69 (76%) had normal LFTs pre-operatively; 298 sets of LFTs were measured post-operatively, with a median of 3 sets per patient; 61 (67%) patients had either normal or static LFTs post-operatively, 13 (14%) had isolated rise in GGT, 16 (17%) had derangement of ALT and AST, and 1 patient (1%) had deranged ALP. Altered clinical decision-making due to LFTs derangement was recorded in two cases (2%).
Conclusion
Clinicians have an obligation to justify expense, and practise in a cost-effective manner. Our data suggest that the routine perioperative monitoring of LFTs in thoracic surgery does not give any clear benefit to patient care.
How can we further reduce the burden and harm that
patients experience from over-investigation and overtreatment?
Dr Catherine Calderwood, Chief Medical Officer for Scotland, 2014 1
Introduction
The Choosing Wisely campaign was established in the United States in 2015 and quickly taken up by organisations in multiple countries around the world, including in the UK by the Academy of Medical Royal Colleges in October 2016. 2 This global initiative promotes patient-centred healthcare with an emphasis on the optimisation of resource use and efficient clinical decision-making. Of particular focus is the goal to avoid investigations or treatments which add little benefit to overall patient care and may impact negatively owing to side effects or ineffective resource allocation. Similar themes are discussed in the British Medical Journal (BMJ) in its “Too Much Medicine” initiative, 3 as well as being raised in an annual international forum at the Preventing Overdiagnosis Conference, currently in its 6th year. 4
Liver failure has been shown to lead to worse perioperative outcomes in several large series, largely in abdominal and cardiac patients.5–7 To our knowledge, there are no published data showing inferior outcomes in patients specifically undergoing thoracic surgery who have a background of liver failure or deranged liver function tests (LFTs). The incidence of liver failure is rising, largely due to a combination of increasing rates of alcoholic liver disease, obesity (non-alcoholic fatty liver disease; NAFLD), 8 and chronic viral hepatitis. 9 In addition, abnormalities of LFTs may be found in up to a third of the UK population without an established diagnosis of liver disease. However, there is a low risk (3–4%) of these patients developing liver failure within five years.10,11
These shifting epidemiological characteristics are leading to increasing numbers of patients with liver failure amongst those being referred to surgical specialities. Scoring systems such as the Child-Turcotte-Pugh (CTP) Score and Model for End-Stage Liver Disease (MELD) have been validated and can be used in the preoperative assessment of at-risk patients.12–14 While liver failure is not necessarily a contraindication to major surgery, special multidisciplinary consideration and planning of the perioperative journey are required to optimise outcomes. 15 In thoracic surgery, the advent of less invasive techniques such as video-assisted thoracoscopic surgery (VATS) may result in patients with severe comorbidities being considered for resection where in the past they may have been deemed unfit.
We postulate that during a typical surgical patient journey, a significant number of investigations will be performed with little to no clinical indication, and that these represent a potentially unnecessary use of resources. We aim to use the example of inpatient LFT monitoring in patients undergoing thoracic resections to highlight this issue through analysis of our patient series, specifically the extent of monitoring of LFTs and their impact on clinical decision making.
Methods
Data were collected retrospectively from the electronic operative database at a high-volume tertiary cardiothoracic surgery centre. All adult patients whose named operation was coded electronically as “lobectomy/bilobectomy” between June and September 2017 were included in the study. In all cases, the decision to proceed to surgery had been made following multi-disciplinary team (MDT) discussion and assessment of fitness for surgery; therefore, our retrospective data collection excluded patients who had been deemed unfit for surgery at time of initial diagnosis. These patients do not enter the surgical pathway and hence their records are not present on our system; the number of such patients during the study period is therefore unknown.
Specific investigations included in our panel of LFTs are shown in Figure 1. Data were collected from electronic patient record on: number of sets of LFTs performed perioperatively, their values, past medical history of liver disease, and whether any change in clinical decision making occurred (in our centre daily ward round and clinical review notes are input onto an electronic system). The perioperative period was defined as from consultation at pre-operative assessment clinic until discharge after surgery.
Investigations included routinely on LFT panel at our tertiary centre and normal values used in our laboratory.
Only LFTs performed at our centre were included; any preoperative sets carried out locally to the patient for separate indications were not measured. Radiological and pharmacy patient records were also screened to determine whether any additional imaging or altered prescribing occurred because of deranged LFTs. Medications were defined as being a possible cause of LFT derangement on the basis of the potential side effects listed in the British National Formulary (BNF).
Results
There were 91 eligible patients over the study period. Mean age was 69 years. Male:female ratio was 42:49. Lobar (lobectomy/bilobectomy) resection was performed in 89 (98%) cases, 2 (2%) cases underwent sublobar resection; 64 (70%) were completed via a VATS approach; the remaining 27 were either planned thoracotomy or initial VATS approach converted to thoracotomy intraoperatively. Median (IQR) length of stay was six (four) days.
Three patients (3%) had a documented history of chronic liver disease (one case of chronic hepatitis C with alcoholism, and two cases of NAFLD); 47 (52%) patients regularly took a medication known to derange LFTs preoperatively, the most common of which was a statin, followed by paracetamol (Figure 2). No patients deviated from our usual outpatient pre-operative assessment pathway as a result of liver disease or hepatotoxic medication.
Potentially hepatotoxic medications taken pre-operatively by our patients. PCM: paracetamol; MTX: methotrexate; BZF: bezafibrate; CMZ: carbamazapine.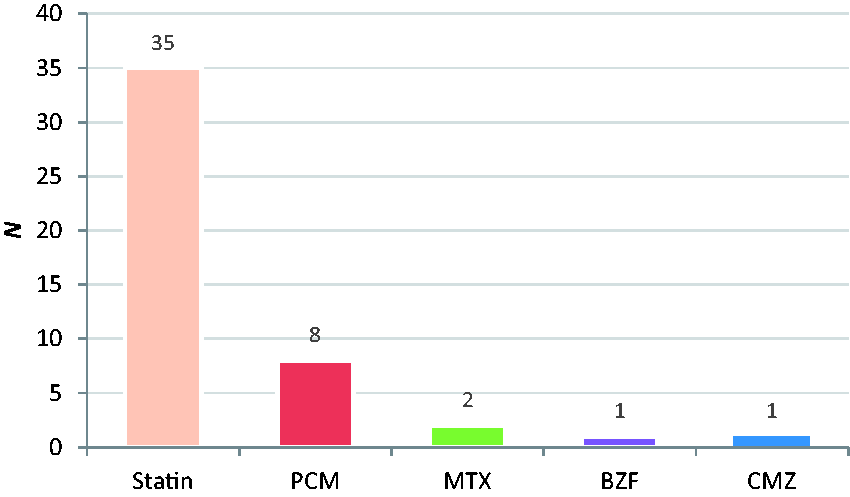
A total of 101 sets of preoperative LFTs were performed in our patient cohort; 77 (85%) of patients had 1 set of LFTs, with 12 (13%) and 2 (2%) having 2 and 0, sets respectively. There was no documented change in clinical condition necessitating the repeat sampling in the 12 patients who had 2 sets. Figure 3 shows preoperative LFT results; 69 (76%) were normal at baseline. Isolated raised GGT was the most common abnormality (15 patients, 16%); range of values was 58–234 IU/L.
Distribution of preoperative LFT results. Distribution of postoperative LFT results, cases included as abnormal if a single set of results were abnormal throughout the postoperative period.
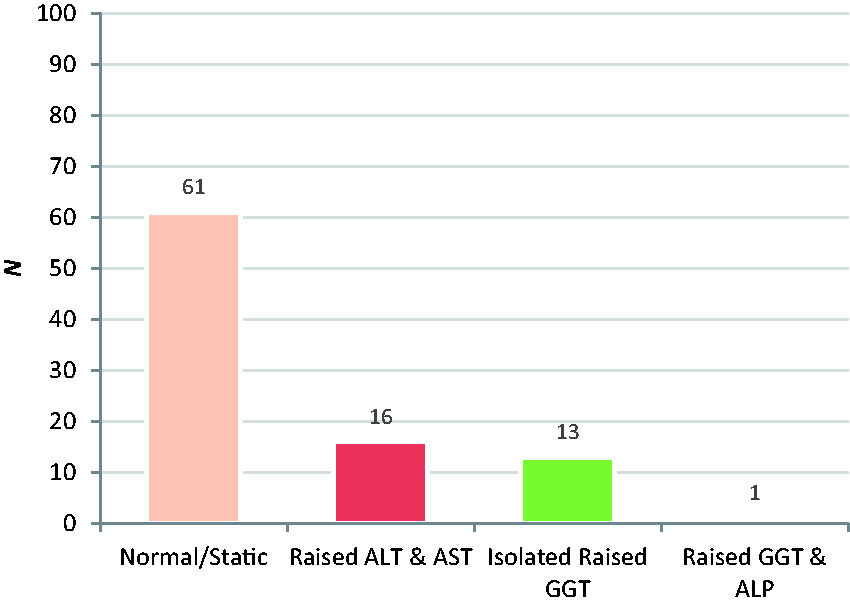
All patients had at least one set of postoperative LFTs; median number of sets performed was 3 (range 1–10). There were a total of 298 sets of LFTs performed over the course of 663 inpatient days. Mean number of sets per inpatient day was 0.47. Postoperative LFTs were within normal limits or static (defined as a change of ≤10% from baseline value) in 61 patients (67%) as shown in Figure 4. Of the remaining 30 patients, the most common abnormalities were a mildly elevated AST and ALT (n = 16; 18%), and a transient rise in GGT (n = 13; 14%).
In 89 (98%) cases, postoperative LFT values either returned to or remained at baseline prior to discharge. All values were improving (trending towards baseline) prior to discharge. In these 89 cases, no alteration in clinical decision-making on the basis of LFTS was identified. The remaining two consisted of one case where repeat LFTs were planned in the community following discharge, and one case where increased monitoring (repeat LFT samples daily for three days) was performed. There were no documented cases where procedural intervention, altered prescribing or radiological investigation occurred because of abnormal LFTs.
Our institution’s laboratory calculated the cost of each set of LFTs on a pro rata basis as £4.50. On this basis, the overall cost to the trust over the study period due to LFT monitoring was £1341.
Discussion
Our data show that during a three-month period in our busy specialist thoracic surgery centre, patients undergoing lobectomy had their LFTs checked on average every second inpatient day. In the majority of patients, baseline results were normal, and most patients did not undergo any deterioration in any measured parameter after surgery. Only one case required altered inpatient care (increased monitoring) due to abnormal LFTs, and one case required additional community monitoring following discharge. In both of these instances, no clear cause for LFT derangement was identified and the results were attributed to likely medication side effects. The derangement (as compared to baseline value) was transient in both cases.
We chose to include patients undergoing the most major routinely performed surgery in our centre as they are likely to suffer a greater physiological disturbance than patients undergoing more minor procedures. Therefore, any clinically significant LFT abnormalities in the perioperative period are likely to be more pronounced in this cohort. Assuming an even distribution of cases throughout a calendar year, our results indicate potential annual cost of LFTs in lung resection patients of over £5000, a significant proportion of which may be avoidable. If our benign and minor cases are incorporated, we estimate that costs will exceed £13,000 per annum. Given that patients are undergoing complex surgery, including exposure to volatile anaesthetic agents which can induce hepatotoxicity, it is reasonable to ensure normal baseline LFTs. We believe that routine repeated LFT monitoring in the postoperative management of thoracic cases does not significantly impact clinical decision making, at significant cost and burden to the service, as well as burden to the patient. Clearly given the physiological stress caused by anaesthetic and surgery, it is reasonable to check LFTs in the initial postoperative period; however, further sampling does not seem to alter management, and we propose that it should be performed only when clinical need dictates, rather than as a routine panel of screening tests. We anticipate that across other specialities there are a variety of investigations which, similarly to our example, are performed without clinical justification and represent a further potential area for service improvement.
There has been a shift in UK healthcare towards fewer inpatient days and shortened waiting lists through national interventions such as enhanced recovery after surgery (ERAS) programmes, fast-track preoperative assessment services, and supported early discharge. This has led to a change in the use of perioperative investigations; increasingly investigations are used as part of a routine protocolised battery of tests where the clinical merit of the information obtained is questionable.
The core ethical principle of non-maleficence underpins medical practice. In the context of the postoperative patient, it is important to identify and consider the harm, direct and indirect, caused by unnecessary investigations. Direct harm includes physical and psychological effects to patients as a result of sampling and further investigation with no merit. The incidental identification of abnormal results which both bear no impact on management and will, in the vast majority of cases, resolve spontaneously, may cause patients undue distress due to their perception that ‘something is wrong’. Indirect harm includes the delay in performing necessary investigations caused by saturation of an already overburdened health service.
Thirteen per cent of our patients underwent repeated preoperative LFT sampling despite normal first result; in none of these cases was there a documented reason for this, and no new LFT abnormalities were identified. It is likely that these patients underwent blood sampling routinely on admission prior to surgery despite the presence of a robust preadmissions service in our centre.
Our data could be used as an example of the burden caused by routinely performing investigations with no clinical indication to allow tailoring of patient journeys to the individual patient, thereby reducing burden on health services. This is applicable across specialties and could incorporate a wide range of investigations, and therefore could lead to large scale optimisation of services and improvement of patient experience.
When opting to not perform investigations, there is a theoretical risk that pathologies may be missed. However, our case series is a representative example showing that in certain circumstances the use of repeated blood sampling as a screening method without clinical change does not improve patient care. We do not suggest stopping all routine bloods as a general rule; rather their need should undergo careful consideration. Clearly this needs to be assessed on a case by case basis; in certain surgical procedures or in specific patient groups, routine monitoring may be indicated. In other patient groups, thorough clinical assessment both before and after surgery can be used to ensure that patients developing hepatic complication are identified without the need to routinely sample LFTs in all patients.
This study is limited by small sample size and single centre data collection. Additionally, our data collection method excludes those patients who did not proceed to surgery following diagnosis because of severe liver disease or significant LFT derangement. Our regional MDT pathway is such that those patients do not undergo surgical consultation unless of borderline fitness for resection. Therefore, our case series is not necessarily representative of the entire population of newly diagnosed lung cancer; however, we believe it is representative of patients who are eligible for surgery.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.