
Abstract
We discuss the case and differential diagnoses of an elderly man who presented with bilateral facial palsy. He had injured his forehead in the garden during a fall on his face and the open wound was contaminated by soil. He then presented to the emergency department with facial weakness causing difficulty speaking. The penny dropped when he started developing muscle spasms affecting his lower jaw a day after admission. It also became clear that he could not open his mouth wide (lock jaw). The combination of muscle spasms and lock jaw (trismus) made tetanus the most likely possibility, and this was proven when he had samples taken from his wound and analysed under the microscope, which showed Clostridium tetani bacilli. C. tetani spores are widespread in the environment, including in the soil, and can survive hostile conditions for long periods of time. Transmission occurs when spores are introduced into the body, often through contaminated wounds. Tetanus in the United Kingdom is rare, but can prove fatal if there is a delay in recognition and treatment.
Case history
A 74-year-old Caucasian man, who had a fall with head injury a week prior to presentation, came in to hospital with a one-day history of progressive bilateral facial muscles weakness, with difficulty speaking and swallowing. He had fallen face-forwards in his garden without loss of consciousness, but had sustained a wound on the right side of his forehead. He did not seek medical attention at that time, thinking it was a minor skin wound. There were no sensory symptoms, bowel or bladder problems or double vision. A day after admission, he started developing lower jaw muscle spasms, and subsequently had difficulty opening his jaw.
There were no constitutional or systemic symptoms such as fever, night sweats, change in appetite, shortness of breath or chest pain.
There was no significant medical history and he was not on any regular medications. He was a fit and healthy man prior to the current illness, but he was not sure about his prior immunisation history.
He had retired from work, lived with his wife and was independent in basic activities of daily living. There was no recent travel history. He did not smoke or consume alcohol. There was no family history of neurological problems.
Examination
On examination at presentation, he was alert and orientated. There was a 3 × 4 cm healing superficial wound on the right side of his forehead. Pupils and eye movements were normal. There was bilateral facial weakness and ptosis. Intermittent spasm of his jaw muscles was noted on the second day of admission. Jaw jerk was normal, but corneal reflexes were absent. Limb examination showed normal tone, power and deep tendon reflexes. There was no sensory loss. Systemic examination was unremarkable.
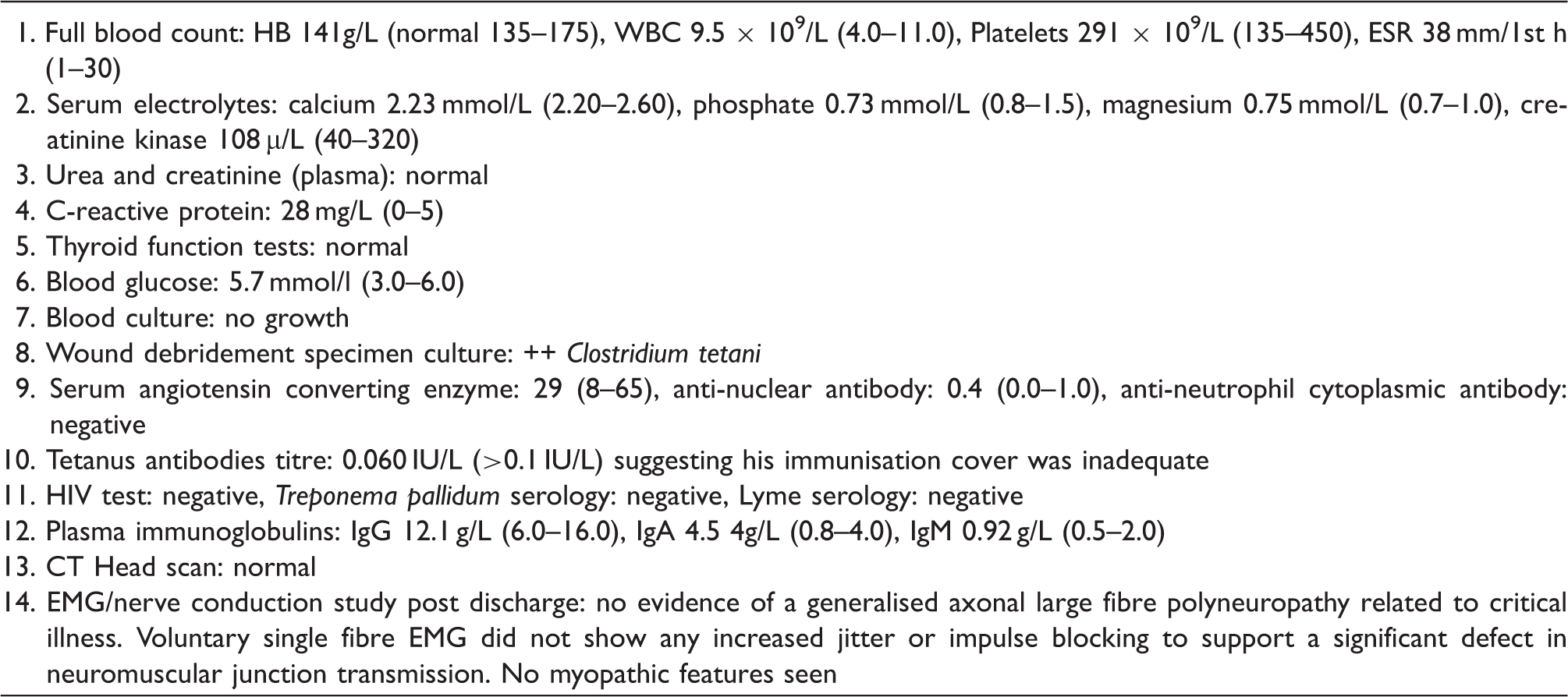
Laboratory and imaging tests while in hospital (normal range in parentheses).
Diagnosis
The suspicion of tetanus arose in the accident and emergency department initially but was later corroborated by the observations (jaw spasms and lock jaw) on the second day of hospital admission by a doctor who had previously seen such cases in Asia, where tetanus is more prevalent owing to inadequate immunisation cover. Once confirmed by laboratory evidence, our patient was given a diagnosis of cephalic tetanus presenting with bilateral facial palsy. Cephalic tetanus presenting with a unilateral facial palsy and ptosis has been reported, 1 but to our knowledge, there is no similar case of bilateral facial palsy due to tetanus in the literature.
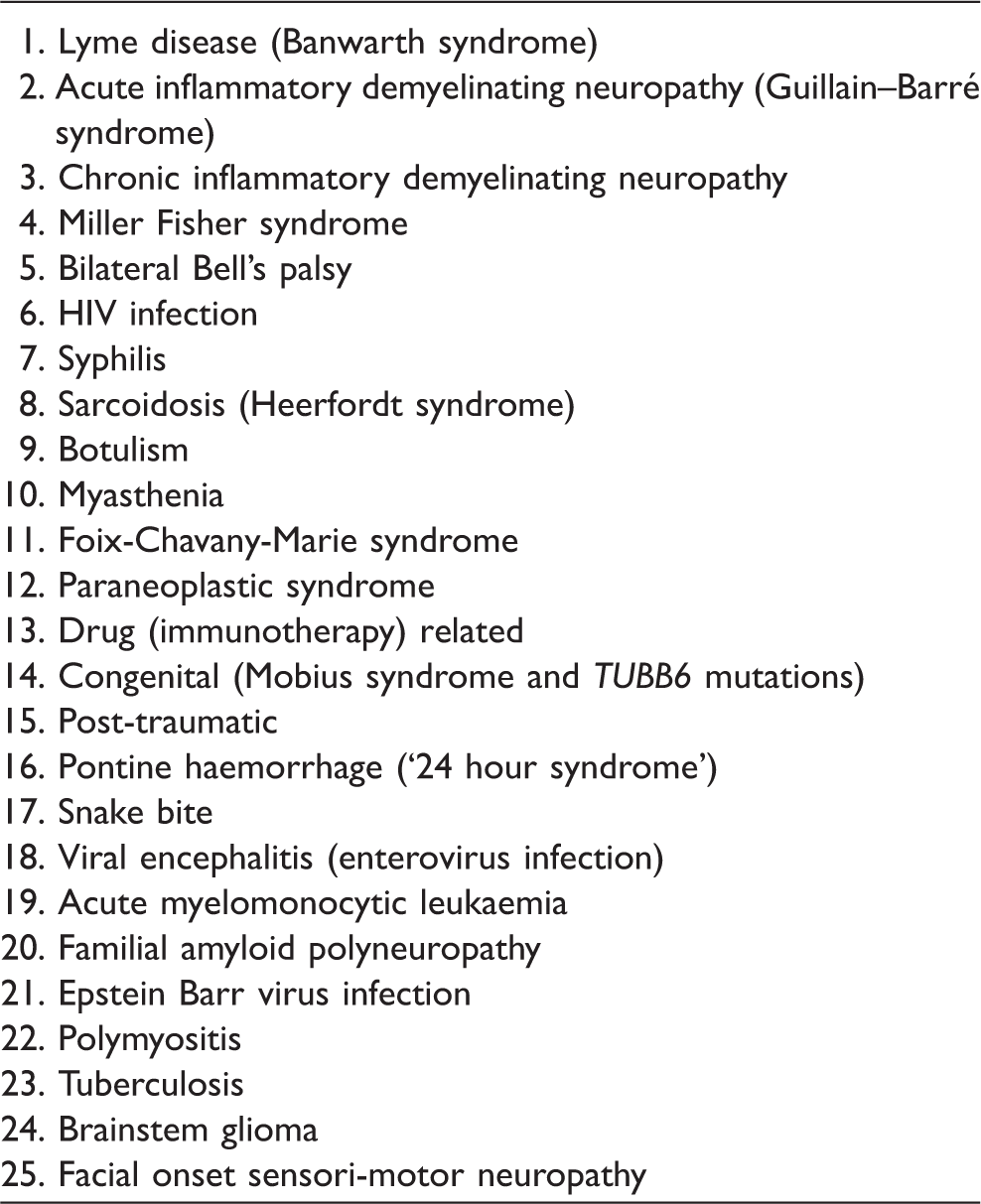
Differential diagnoses
Management
In the accident and emergency department, he was given tetanus toxoid and a dose of tetanus anti-toxin. Wound debridement was performed on the second day of admission, and tissue samples were sent to microbiology for confirmation of the diagnosis. Antibiotics to cover Clostridium tetani were commenced intravenously immediately after wound debridement. By this time (on the second day), his lock jaw was becoming more obvious, and he was transferred to the intensive therapy unit to protect his airway. He had a tracheostomy and was commenced on ventilatory support. He was treated with intravenous benzyl penicillin and metronidazole on the intensive care unit. Microbiology tests confirmed the presence of C. tetani in the tissue specimen from wound debridement.
Discussion
Our patient presented with a bilateral facial palsy but then developed spasms of his jaw muscles which, along with the contaminated wound on the forehead and lack of a clear immunisation history, suggested that this was cephalic tetanus. Lock-jaw or trismus is the pathognomonic feature of tetanus, which in the right context provides a clue to the potential diagnosis. The rapidity of onset of a bilateral facial palsy in his case made some other causes of this problem (Table 2) such as sarcoidosis less likely. Although Guillain–Barré syndrome (GBS) can also cause facial diplegia and isolated facial diplegia in GBS has been described, 3 his preserved deep tendon reflexes argued against this being GBS or Miller Fisher syndrome (MFS). His tempo of illness clearly did not suggest chronic inflammatory demyelinating neuropathy (CIDP) or a familial amyloid polyneuropathy (FAP). Our patient had no history of tick bite, or travel to an endemic area of Lyme disease. CT head scan ruled out the possibility of brainstem haemorrhage.
Unlike unilateral facial palsy which is idiopathic in up to 50% of cases (commonly called idiopathic Bell’s palsy), bilateral facial palsy is idiopathic in only 20% of cases. 4 Therefore, it requires further investigation to search for the underlying aetiology. 4 This depends on the tempo of the illness, associated features, and preceding history including history of travel, exposure to toxic agents and sexual contacts. Particular attention should be paid to deep tendon reflexes on examination as their loss is a pointer towards GBS, MFS or CIDP. Lyme disease is the first infectious disease that should be considered in endemic areas and any history of tick bite or rash elicited. Lyme and HIV serology should be arranged in those at risk. Cerebrospinal fluid examination (CSF) to look for albuminocytologic dissociation (i.e. elevated CSF protein but not cell count, which is seen in GBS), pleocytosis (elevated cell count is seen in infectious disorders) and viral PCR is recommended. Other tests to consider are anti-ganglioside antibodies, chest X-ray, serum angiotensin converting enzyme and an MRI brain scan to exclude any brainstem pathology.
Tetanus is a preventable (with vaccination) and treatable illness. Immunisation against tetanus in children is almost universal in western countries, but people may miss booster doses later in life, thereby putting them at risk. Treatment of patients with tetanus may involve the use of muscle relaxants such as diazepam, ventilatory support in an intensive care unit, management of dysautonomia with drugs such as beta-blockers, neutralisation of tetanus toxin with human tetanus immune globulin 3000–6000 IU, wound debridement and administration of antibiotics such as metronidazole intravenously and intramuscular benzathine penicillin as a single dose; or intravenous benzyl penicillin to eradicate Clostridium tetanus bacilli. 5 Antibiotic treatment is started empirically before microbiologic confirmation is available and other therapies such as magnesium sulphate, dantrolene and intra-thecal baclofen have some evidence of efficacy in tetanus but are best offered on the intensive care unit. 5 Timely recognition and treatment is essential to reducing morbidity and mortality. Most patients with generalised tetanus will require intensive care treatment. With intensive care treatment and tracheostomy, the mortality rate of tetanus has reduced from about 45% in the 1950s to 15% 6 in the 1980s to 7% 7 in recent years.
Our patient made a good recovery and was able to go home, walking unaided. The good outcome in his case was down to prompt recognition of the physical signs that helped in getting the diagnosis right and the treatment that he received in the intensive therapy unit.
Learning points
Prompt recognition of the symptoms of tetanus by acute medical physicians is crucial to instituting appropriate treatment in a timely fashion. Lock jaw or trismus raises concerns about tetanus in a person who has evidence of a puncture or contaminated wound. Intensive care unit treatment of patients with generalised, neonatal and cephalic tetanus reduces morbidity and mortality. Tetanus is a clinical diagnosis; ancillary testing only provides supportive evidence and helps exclude other differential diagnoses.
Footnotes
Authors’ contribution
All authors contributed equally to the article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.