
Abstract
Aims
Much has been written about the use of the Mental Health Act in psychiatric settings. There is, however, little written on its use to detain patients with mental disorder in general hospitals.
Method and results
We therefore carried out a survey of the use of the Mental Health Act in general hospital settings in Aberdeen, and also posted a questionnaire to Scottish Liaison Psychiatrists, asking about their experience of the use of the Mental Health Act in general hospitals. Over a six-month period in Aberdeen Royal Infirmary, we identified 39 detentions. Out of hours, the use of Emergency Detention Certificates was more common than use of Short Term Detention Certificates – the latter is recommended by the Mental Welfare Commission, as patients are afforded more rights. When psychiatric staff were not directly involved, procedural and administrative errors were more likely to occur. Liaison psychiatrists elsewhere in Scotland reported similar observations.
Conclusion
General hospital clinicians are unfamiliar with the Mental Health Act and its use. Errors in its application therefore arise, and are more common when psychiatric staff is not involved. Better education, including the provision of written information and consideration of an electronic system, may improve current practice.
Background
There are occasions when it is necessary to use legal powers to detain and treat patients with mental disorder in general hospitals and emergency departments. This can involve those with known mental disorders as well as those with the acute psychiatric manifestations of a physical disorder. Liaison psychiatrists who work in these settings are often involved in the process of detaining patients or giving advice to general hospital staff; however, psychiatric staff are not always immediately available and owing to the urgency of some situations, general hospital staff may therefore be required to grant detentions themselves. In Scotland, this is done under the provisions of the Mental Health (Care and Treatment) (Scotland) Act 2003. 1
The main civil detentions that can be used in the acute setting are the Emergency Detention Certificate (EDC) and Short Term Detention Certificate (STDC). The EDC can be granted by any medical practitioner fully registered with the GMC, with Mental Health Officer (MHO) consent – or without such consent in situations where this is deemed ‘impracticable’. An STDC can only be granted by a Medical Practitioner approved under Section 22 of the Act, (Approved Medical Practitioner, AMP), with MHO consent. An AMP is a registered medical practitioner who has undertaken training in the Act and is either a Member or Fellow of the Royal College of Psychiatrists, or has four years continuous of experience working in Psychiatry and been sponsored by their local Medical Director. 2
The general hospital setting poses problems less likely to occur in a psychiatric hospital, which may be partly due to general hospital staff being unfamiliar with the Mental Health Act, as it is not a routine part of their work. These can include paperwork and documentation not being completed correctly, an MHO not being involved and certificates not being passed to appropriate administrative staff and therefore not being processed correctly. For example, if an EDC is not processed, an AMP may not be allocated, and detentions may be ‘revoked’ inappropriately by non-psychiatric staff. If the procedures are not followed correctly, the detention is open to challenge and could be considered an unlawful deprivation of liberty.
There is a specific process set out under the terms of the Act, along with guidance provided by the Mental Welfare Commission.
2
The procedure of detaining a patient is as follows:
Practitioner completes a medical examination (and considers criteria to be met) The practitioner seeks the consent of an MHO. The MHO will then either give or withhold consent, depending on their determination as to whether the criteria for detention are met. Once consent is obtained (or the reasons for its absence documented), the EDC form should be completed and passed to the hospital managers or those acting on their behalf (usually the hospital records department, but this will vary by location).
An EDC can be issued without MHO consent, in circumstances where waiting for the assessment would be considered ‘impracticable’ and result in undesirable delay. Should this occur, the doctor must document the reasons for the lack of consent within the relevant section of the certificate. If an MHO assesses and refuses consent, the detention should not be granted, but if the doctor felt there were exceptional circumstances, a second MHO’s opinion could be sought.
3
This final step of passing the certificate to the hospital managers is necessary for the lawful detention of a patient in hospital. Failure to do so will result in the detention being open to challenge. In the case of the EDC, the duties placed on the hospital managers under Section38(3)(a) include notifying a range of parties (including nearest relative, named person if one is nominated, and the Mental Welfare Commission) within 12 h of receiving the certificate, as well as the Local Authority if the certificate was granted without MHO consent. In the case of a STDC, within seven days, the Managers must also notify the Mental Health Tribunal for Scotland and the Mental Welfare Commission, and send a copy of the certificate.
STDCs are described as being the preferred ‘gateway order’ into detention under the Act and should be granted where possible in preference to an EDC. As compared to the EDC, the STDC can only be granted by an AMP, the consent of an MHO is mandatory, and it confers more rights on the patient and their named person, including the right to make an application to the Tribunal to revoke the certificate. 3
In Aberdeen, certificates can be processed through various routes. During working hours (9 am to 5 pm, Monday to Friday), certificates are handed to the Records Department, Aberdeen Royal Infirmary. Outwith these hours, certificates are passed to the hospital ‘Site and Capacity’ Office (staffed by senior bed manager/nurse managers out of hours) and are taken to the Records Department the next working day. Some are processed by the Mental Health Act administrator at Royal Cornhill Hospital – the local psychiatric inpatient hospital – if the patient is transferred immediately after a detention has been granted.
Aim
The aim of our study was to gain a greater understanding of the approach to, and difficulties encountered in, the process of detaining patients in the general hospital setting. We posed the following questions:
How many people are detained under provisions of the Mental Health Act in the general hospital? Who detains patients? Is due process followed? Is the paperwork being properly processed? How are these issues managed in other Health Boards?
Method
There were two strands to this study. The first was a survey of detentions granted in the general hospital settings in Aberdeen, and the second was a survey of the experiences of Liaison Psychiatrists around Scotland.
Survey of detentions in general hospitals in Aberdeen
This survey was carried out in the main inpatient general hospital settings in Aberdeen, which serve Aberdeen and Aberdeenshire, along with providing specialist services to patients from Moray, Orkney and Shetland. Aberdeen is a city in North East Scotland with a population of approximately 214,610 people, 4 with a further estimated 262,190 in Aberdeenshire. 5 The main site is the Foresterhill Health campus, which comprises Aberdeen Royal Infirmary, Royal Aberdeen Children’s Hospital and Aberdeen Maternity Hospital. Other inpatient hospital sites include Woodend Hospital (elective orthopaedic surgery, geriatrics and rehabilitation) and Roxburghe House (palliative care). 6 Aberdeen Royal Infirmary is a tertiary hospital, one of the Scotland’s four major trauma centres. It has approximately 700 inpatient beds, 7 and an emergency department.
The survey was carried out between March and October 2017. All inpatient detention certificates were examined. A record of patients detained during the study period was kept by the liaison psychiatry department, and additionally certificates were reviewed in the medical records department in ARI and at RCH. Detentions granted in community settings (for example by general practitioners (GPs)) were not included.
Survey of liaison psychiatrists elsewhere in Scotland
Liaison psychiatrists working in Scottish general hospitals were asked to participate in an online survey and complete a questionnaire consisting of 10 questions (online Appendix 1) – they were contacted via the Royal College of Psychiatrists in Scotland Liaison Faculty.
Responses were collected over a period of one month with one reminder. The survey was closed after 28 days, and the data were analysed using the SurveyMonkey online platform.
Results
Survey of detentions in general hospitals in Aberdeen
During the six-month study period, 39 detentions were identified. All were EDCs and STDCs. There were no uses of the Nurses Power to Detain or Compulsory Treatment Order applications.
Locations
Location of Detentions in ARI
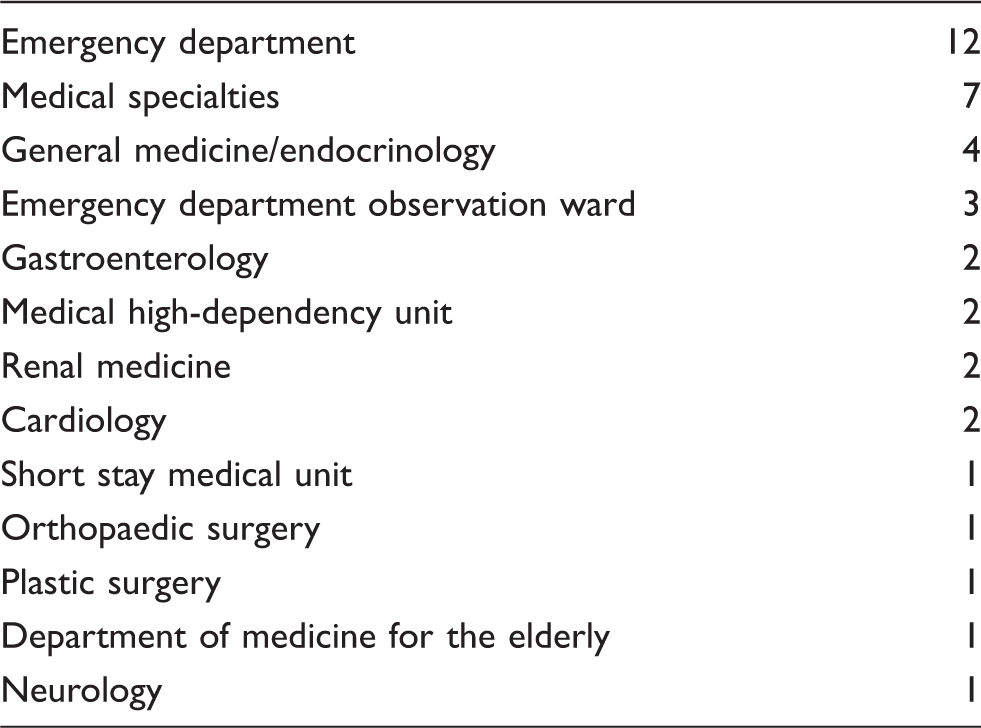
EDC versus STDC
Thirteen (33.3%) detentions were granted during working hours, with 26 (66.7%) granted out of hours. There were 24 STDCs granted compared to 15 EDCs (62% vs. 38%). Of the normal working day detentions, only one EDC was granted, compared with 12 STDCs; this is reversed out of hours, where 14 EDCs were granted compared with 12 STDCs (54% vs. 46%).
Who detains?
EDC
Psychiatric staff were involved to some extent in the majority of EDCs. Eight of the 15 detentions were granted by non-psychiatric staff. In six of these, telephone advice from psychiatric staff was documented; however, in two there was no record of contact with psychiatric staff. One of these forms was discovered by the liaison psychiatrist when an assessment was requested, after the detention would have lapsed. One was discovered incidentally in the ED observation ward the day after the patient was detained: Psychiatric staff routinely attend in the morning, so review may have been assumed. These detentions were granted by GP trainees and medical higher trainees.
Of the remaining seven EDCs, two were granted by AMPs (who documented that it was not practicable to wait for an MHO to attend) and five by non-AMP junior psychiatric on-call medical staff. Of note, only three of the 15 (20%) EDCs had MHO consent; however, all of these had documented that it was too urgent or impracticable to wait for MHO attendance.
Four (26.7%) EDCs were converted to STDCs. Five (33.3%) were revoked within the 72 h detention period if the situation had changed, and six (40%) were allowed to lapse – in these cases, the patients were either discharged from hospital as inpatient treatment was no longer necessary, or they had improved and were able to consent to continued inpatient treatment on a voluntary basis.
STDC
Ten STDCs were granted during working hours, all by the Liaison Psychiatry Team – five by a core trainee (CT) three with AMP status, two by a specialty trainee (ST) five in Psychiatry, and three by the consultant psychiatrist.
Fourteen were granted out of hours: One by a CT with AMP status, one by a locum ST, 10 by STs (ST4, 5 and 6) and two by consultant psychiatrists.
Paperwork processed within 24 h?
The Act states that an EDC should be processed within 12 h of the Hospital Managers receiving it, and that the Mental Welfare Commission should be sent a copy of the form as soon as practicable and no later than seven days after. The certificates record the date the notification was completed.
Each certificate stated that the hospital managers sent notification to the relevant parties within the required 12-h timescale, after the form had arrived in their department. The date of notification is recorded on the form, but unfortunately not the time, as there is nowhere for this to be specifically recorded, so for the purposes of this study, we recorded whether the forms were processed by the department within 24 h of the certificate being granted.
Of the 13 certificates granted within working hours, 11 were processed by the records department within 24 h. The two that were not had in fact been handed to the Site and Capacity Office as they had been granted at the end of the day.
Twenty-six were granted out of hours: 13 were processed within the next day and 13 were not. Of those that were not: Three were granted at weekends or public holidays and were processed the next working day. In nine cases, there was an apparent delay in the forms reaching the records department following the detention being granted. A small number may have been delayed in processing owing to the administrator’s workload. This will have resulted in a delay in notification of the relevant parties. It appeared that three forms (two known to have been handed to the Site and Capacity Office, and one discovered incidentally in patient notes) were not processed, and therefore the Mental Welfare Commission was never informed of the detention, which may mean those detentions could be considered unlawful.
It was discovered that the hospital records department had been sending STDC forms to the Mental Welfare Commission but not to the Mental Health Tribunal for Scotland as per their duties outlined in Section38(3)(a). This is a legal requirement and may leave the detention open to challenge, and could impact on a patient’s ability to appeal against detention. This was discovered in one case after the Tribunal advised they had received no notification of the STDC, when a subsequent Compulsory Treatment Order application as made.
Additional notes
On one occasion, a consultant physician attempted to grant an STDC, not realising they did not have this power under Section 22 of the Act. In this case, the attending MHO realised, offered advice and the duty AMP was contacted.
Finally, we do not know whether any other detentions were granted that did not come to the attention of the psychiatric services and were not processed appropriately.
Survey of liaison psychiatrists elsewhere in Scotland
Eleven Scottish liaison psychiatrists who, in total, provide cover for the following hospitals responded to the survey:
Aberdeen Royal Infirmary, Aberdeen Aberdeen Maternity Hospital, Aberdeen Roxburge House, Aberdeen Woodend Hospital, Aberdeen Glasgow Royal Infirmary Queen Elizabeth University Hospital, Glasgow Falkirk Royal Infirmary Victoria Hospital, Kircaldy Western General Hospital, Edinburgh Crosshouse & Ayr Hospital, Kilmarnock Royal Hospital for Sick Children, Edinburgh Royal Infirmary Edinburgh
All respondents indicated that during working hours, STDCs or a mixture of STDCs and EDCs are used to detain patients. This often, but not always, involves input from an AMP. No respondent reported the exclusive use of EDCs. Detention by general hospital staff is more common out of hours than during working hours (nine versus four respondents), with non-AMP psychiatric staff (such as Foundation doctors or Core Trainees on call for psychiatry) also being more commonly involved out of hours than during working hours. Only three respondents indicated that out of hours, AMPs are routinely involved in detentions. STDCs are more frequently used during working hours and less frequently out of hours. Respondents indicated that out of hours, even when psychiatric staff are involved, the use of EDCs is more frequent.
Eight respondents indicated that detention papers are passed to the general hospital managers to process, but two stated they are passed to managers in the psychiatric hospital. One respondent indicated papers were processed by the psychiatric department within the general hospital. Five respondents indicated that the detention papers are taken to the hospital managers by psychiatric staff; four stated that this was normally done by general hospital staff and two respondents each described emailing or posting papers to managers.
Ninety per cent of those surveyed indicated that there had been occasions when patients detained on an EDC were not notified to psychiatric staff in order to request a review. Only one responder indicated that this never happens. All participants had experienced detention paperwork being incorrectly filled out and 90% also indicated having witnessed occasions when MHOs were not contacted by general hospital staff, although 67% said that this was rare. All clinicians surveyed had experienced MHOs being unable to attend. The most frequent problems encountered during the detention process were the unavailability of an MHO as well as detention papers not being passed to the hospital managers in a timely manner.
Sixty-four per cent of respondents indicated that they provide written guidance to help general hospital staff in the detention process and over 80% also said that they provide educational sessions.
Discussion
Our survey highlights several areas where problems can arise in the process of detaining a patient in a general hospital. The unfamiliarity of general clinicians with mental health legislation may contribute, but there are also problems in paperwork being appropriately processed once completed.
The second part of this study has shown that there is variability in processes and staff involved depending on location throughout Scotland. NHS Grampian has a policy that favours the use of STDCs over EDCs, with a general expectation that AMPs will attend out of hours, more so than most other Health Boards in Scotland. This is reflected in national data, which show that NHS Grampian uses EDCs significantly less than the national average, although these data include all detentions.8,9 EDCs were applied in just over half of out of hours detentions in Grampian, but this may also have been influenced by unavailability of an MHO, which may necessitate use of an EDC even if an AMP is involved.
In Aberdeen Royal Infirmary, during this study period, there were three detentions per month on average. There are around 700 inpatient beds, so the proportion of detained patients is small, so most clinicians will come into contact with detained patients infrequently and will therefore be unfamiliar with the detention process.
Suggestions for improvements
The current system has areas that could be improved. Clinicians who rarely detain patients will be less familiar with use of the Act, so educational efforts, in both its application and where to access appropriate advice, will be necessary. Written guidance on the use of Mental Health Act is already available in several locations including Aberdeen, but it is unclear how effective these efforts are.
There are problems with the appropriate delivery of paperwork to those acting on behalf of Hospital Managers, and in the process itself – In Aberdeen Royal Infirmary, initial results of this study have been highlighted to both the Nursing Management and Records Manager, which has improved communication regarding detentions between these departments. Heightening awareness of problems should therefore continue to reduce errors in the process.
We would suggest that one possible improvement would be the implementation of a fully electronic system. This could take the form of an online certificate that cannot be submitted until relevant parts are correctly completed. Signing electronically would automatically alert relevant parties. There would be logistical issues with this (for example, GPs working in community settings), and it may be necessary to ensure registered and AMPs, and MHOs, had a method of signing this online, but these should not be insurmountable challenges: A fully electronic method should reduce potential for error and delays in submitting and processing paperwork, and potentially be more straightforward to record and audit.
The results of this study will be circulated locally, and shared with the Mental Welfare Commission. Following the circulation of the study results and ongoing educational efforts to clinical staff, a further review of detentions will be repeated locally.
Conclusion
Our study provides a small insight into the use of the MHA in the general hospital setting.
EDCs are used more commonly than STDCs out of hours, and this would seem to reflect the reduced availability of AMPs and MHOs. In comparison with other localities, NHS Grampian appears to more routinely expect AMPs to be involved out of hours, although EDCs are still used more frequently, even when psychiatric staff are involved.
Our study highlights several problems that can occur in the detention process. At times, this is related to the inexperience of general hospital staff – both clinical and administrative – in the use of the MHA. This can lead to problems with the granting of detentions, and in the processing of certificates. This could mean a delay in appropriate review of the detention by senior psychiatric staff, and ultimately if processes are not followed, detentions granted in the hospital could be considered to be an unlawful deprivation of liberty.
We suggest that there is an ongoing need for psychiatrists and those familiar with the law to provide education and advice to hospital staff and increase awareness of the difficulties that may arise. In addition to this, wider system changes, such as a change from paperwork to electronic systems, may offer improvements in this process.
Supplemental Material
Supplemental material for Detaining patients in the general hospital – current practice and pitfalls
Supplemental Material for Detaining patients in the general hospital – current practice and pitfalls by Murray Smith, Rian O’Regan and Rainer Goldbeck in Scottish Medical Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.