
Abstract
Introduction
Duplication of gallbladder is a rare congenital condition. We describe a patient who underwent robotic cholecystectomy for duplicated gallbladder with symptomatic gallstones.
Conclusion
Surgeons performing cholecystectomies must be aware of duplicated gallbladders and robotic cholecystectomy is a feasible option for such patients.
Introduction
Duplication of gallbladder (DG) is a rare congenital condition that occurs in 1 in 4000 births. 1 Such abnormalities of the gallbladder can increase the risk of iatrogenic biliary injuries at laparoscopic cholecystectomy. These malformations can also be associated with cholelithiasis as a consequence of abnormal gallbladder biliary drainage and function. 2 Laparoscopic cholecystectomy is the treatment of choice for selected types of gallbladder duplication. The additional use of intra-operative cholangiography or indocyanine green imaging might assist in the identification of the biliary anatomy at the time of cholecystectomy. This case report describes a patient with duplicated gallbladder, which was subsequently removed by robotic cholecystectomy.
Case report
A 68-year-old male with medical history of hypertension, hyperlipidaemia and surgical history of open pyeloplasty for right-sided pelvic–ureteric junction obstruction underwent abdominal computed tomography (CT) scan in February 2015 for right-sided abdominal pain. His full blood count, liver and renal function, and clotting profiles were all normal. CT scan showed the presence of duplicated gallbladder. Magnetic resonance cholangiopancreatography confirmed complete gallbladder duplication with two cystic ducts entering the common bile duct (Figure 1). Additionally, both gallbladders contained gallstones.
Pre-operative MRCP demonstrating duplicated gallbladder with gallstones within each gallbladder.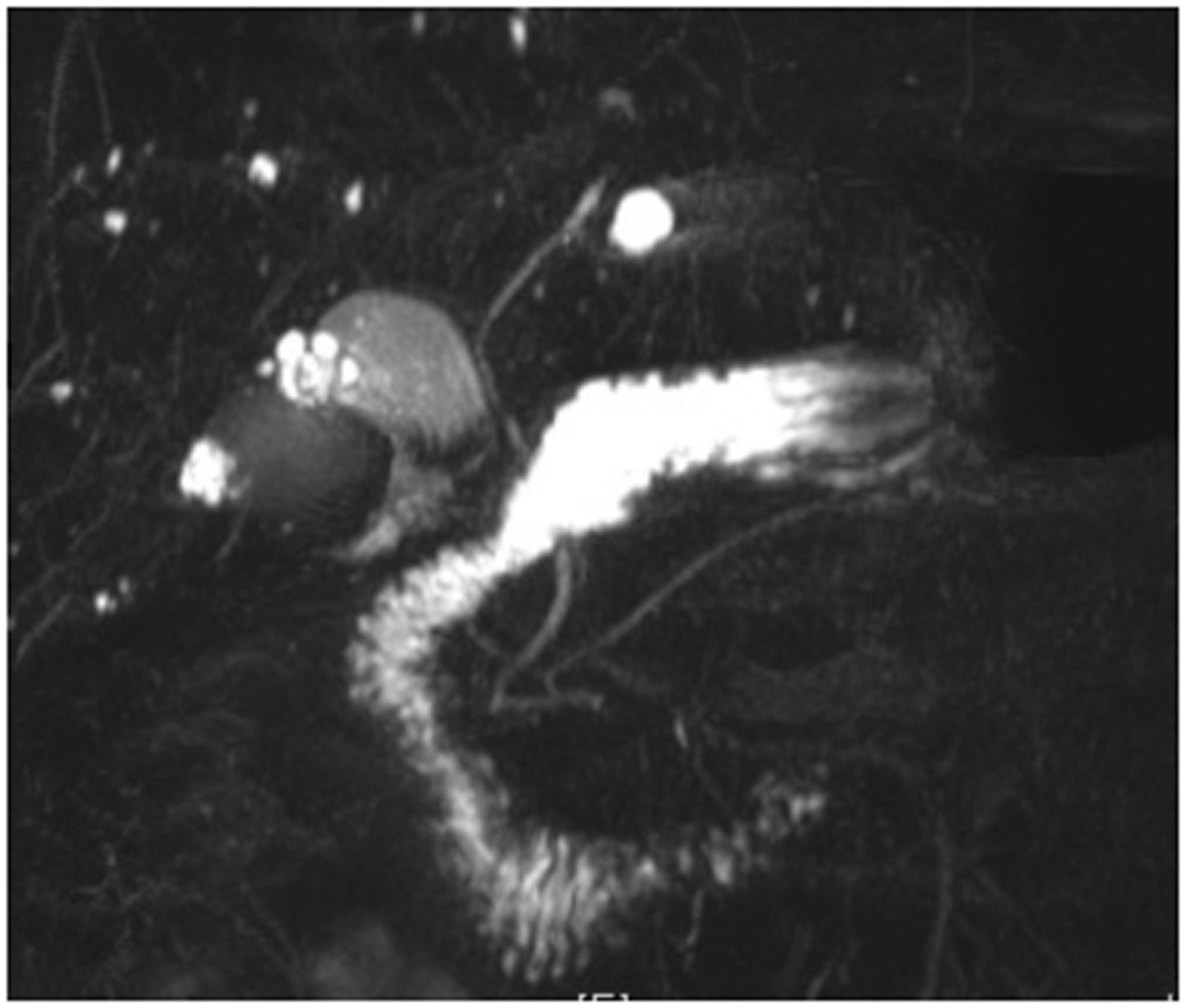
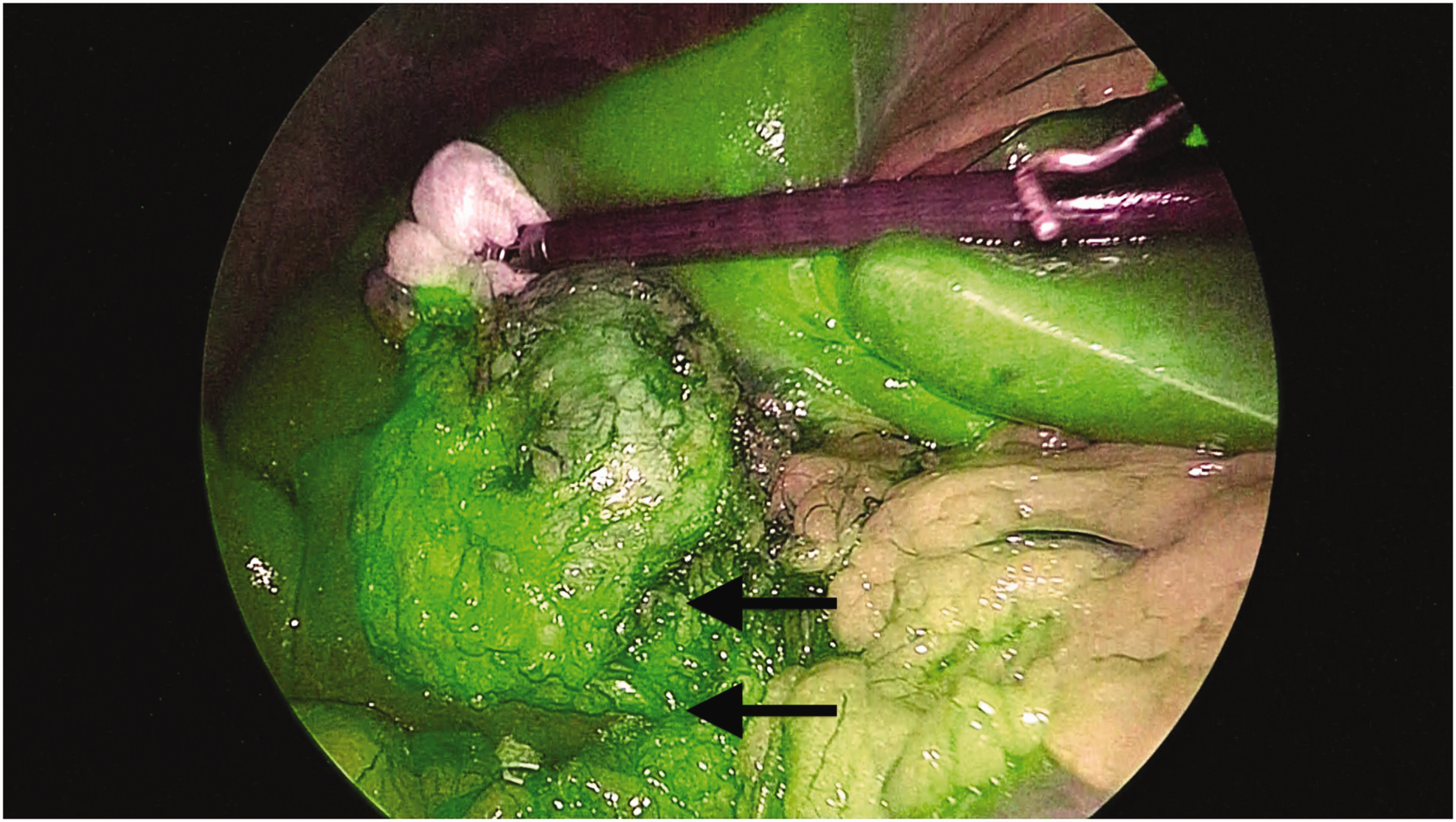
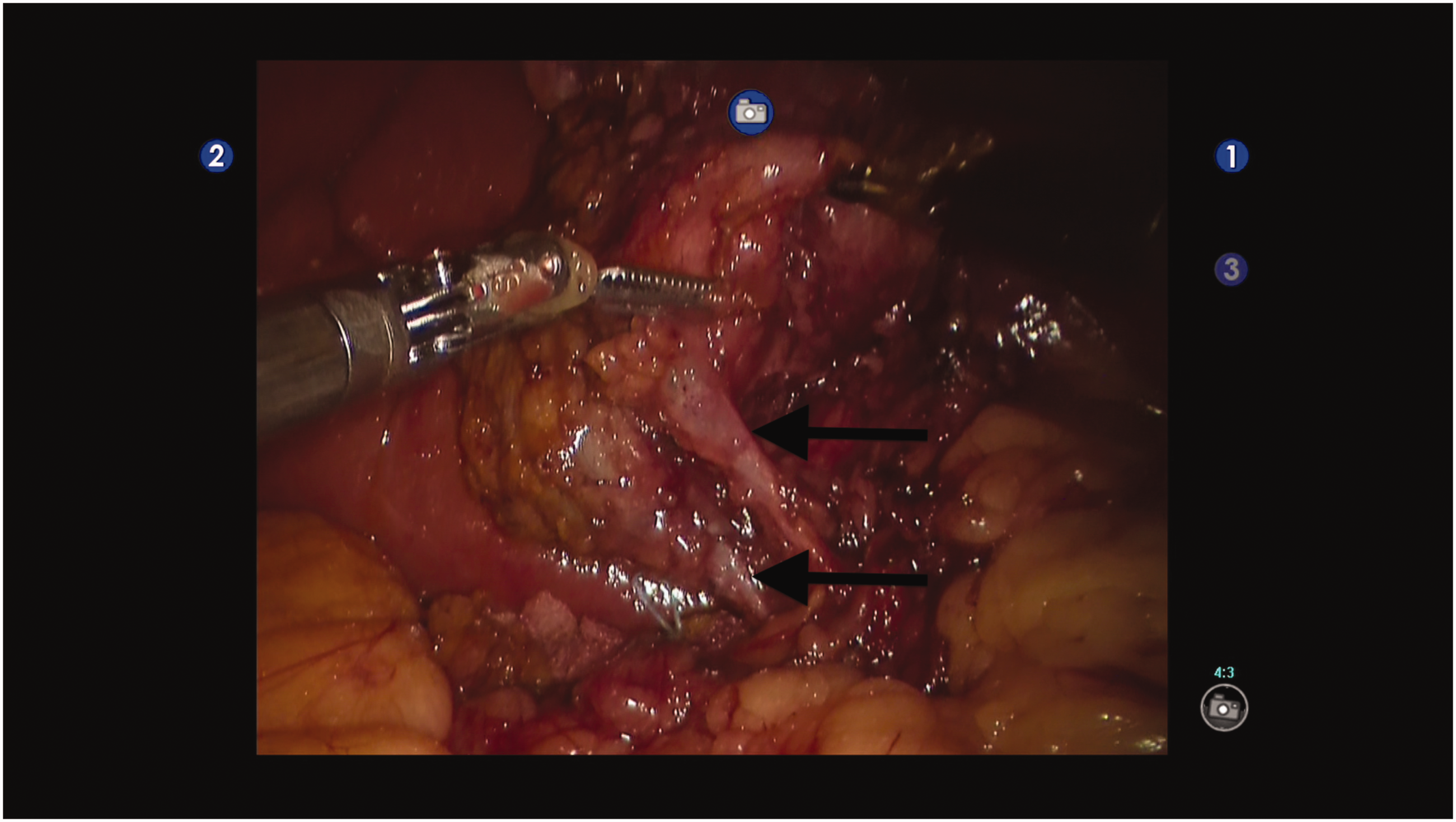
The patient underwent robotic cholecystectomy for duplicated gallbladder in late 2017. The da Vinci S robotic system (Intuitive Surgical, Sunnyvale, CA, USA) was used in this operation (Figure 2). The patient was placed in the reverse Trendelenberg position and dissection was performed with the diathermy hook. The operation started with division of adhesions between the gallbladder and the hepatic flexure. Intra-operative indocyanine green imaging was used to identify the biliary tree (Figure 3). The hepato-cystic triangle was dissected to confirm the presence of two cystic ducts (4–5 mm in diameter each) draining into the common bile duct (Figure 4). Further, dissection confirmed a single cystic artery. Robotic cholecystectomy was then completed as per standard techniques. The operation time was 140 min with blood loss of 50 ml.
The da Vinci S robotic system (Intuitive Surgical, Sunnyvale, CA, USA) used to perform the robotic cholecystectomy. Intra-operative indocyanine green imaging to identify the biliary tree (black arrows). Intra-operative photographs of duplicated gallbladder with double cystic ducts (black arrows).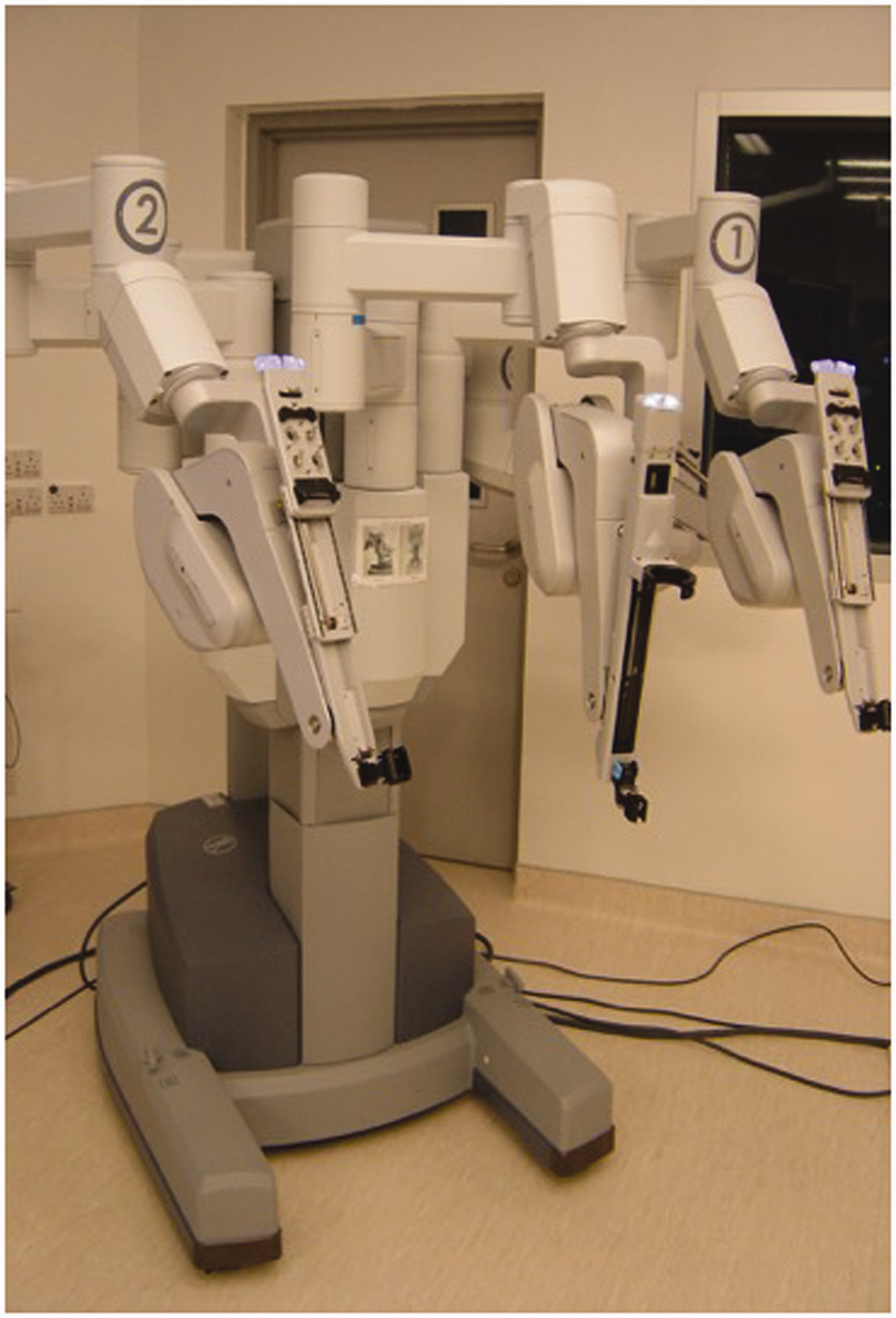
The patient made an uneventful post-operative recovery and was discharged on post-operative day four. The patient was well at the six-month surgical clinic follow-up. Pathology of the specimen showed a 6 × 3 cm and 5.5 × 1.5 cm connected duplicated gallbladder with features of chronic cholecystitis with no malignancy in both gallbladders.
Discussion
DG is a rare congenital condition with an annual incidence of around 1 in 4000,1,3 and can be described by Harlaftis’ classification. 4 In type 1, both gallbladders insert into the common bile duct via a single cystic duct. For type 2, both gallbladders have their own individual cystic ducts that either join into the common bile duct or into the right or left hepatic ducts. In type 3, there are three gallbladders with up to three separate cystic ducts, and with type 4, the gallbladder itself is not connected to the biliary tree or gastrointestinal tract. These ectopic gallbladders can cause diagnostic confusion and may result in unnecessary investigation and treatment, with potential patient morbidity. 5 The differential diagnoses of a DG include hepatic cyst adjacent to the gallbladder and type 2 choledochal cyst or biliary diverticulum. 6 To be considered a true duplicated gallbladder, each gallbladder must contain valves at its neck, have a muscle layer and be able to concentrate bile. 7 The risk of malignancy arising from DG is considered low 8 and there is no indication for cholecystectomy for asymptomatic and incidental finding of DG. 9
Preoperative diagnosis of DG is difficult, with detection rates of only 50% by ultrasound scan. 10 However, the use of magnetic resonance cholangiopancreatography (MRCP) and endoscopic retrograde cholangiopancreatography (ERCP) 10 has increased the detection rate of such gallbladder anatomical anomalies.3,11
For patients with symptomatic cholelithiasis in the presence of DG, concurrent cholecystectomies of both gallbladders are recommended at operation to prevent biliary complications from the remnant gallbladder. 12 The general advice is to perform laparoscopic cholecystectomy for type 1 DG. However, the open approach is suggested for type 2 DG, as there is an increased risk of bile duct injuries secondary to the high insertion of the accessory cystic duct into the common bile duct and the additional tissue dissection required to adequately ligate the cystic duct. 10 The use of intra-operative cholangiography and indocyanine green fluorescence imaging can assist in the correct identification of the gallbladder and biliary tree anomalies. 13
In our case, the patient had a duplicated gallbladder containing two separate cystic ducts and a single common cystic artery (Harlaftis type 2 ‘H’ type ductal duplication). Whilst open cholecystectomy is recommended for type 2 DG, we performed robotic cholecystectomy for this patient. In the management of elective complex biliary conditions, there is the potential requirement for primary biliary repair. The robot has a significant advantage compared to the laparoscopic approach because the robot has a stable platform that allows for precise suturing of the bile duct. Additionally, the robotic approach allows the patient to enjoy the benefits of minimal access surgery despite having a condition normally requiring open cholecystectomy.
There have been case reports of successful laparoscopic management of different types of DG,9,14–16 but to our knowledge, there has been only one published report of robotic cholecystectomy for DG. 17 Outcomes after cholecystectomy for DG are favourable, although bile leakage after such operations has been reported. 14 In our patient, the robotic cholecystectomy was uneventful and the patient made a rapid recovery from the minimal access operation.
Conclusion
Surgeons performing cholecystectomies must be aware of duplicated gallbladders so that both gallbladder moieties are removed completely and to anticipate associated biliary anatomical anomalies. Robotic cholecystectomy for duplicated gallbladder is a feasible option for such patients, and may allow minimal access surgery in conditions that might otherwise require open cholecystectomy.
Footnotes
Authors’ contributions
AKYF wrote the draft manuscript. KFL, CCNC, PBSL approved the final manuscript for submission.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.