
Abstract
This report presents the fatal case of a 63-year-old man with a new presentation of liver cirrhosis, presumed concurrent acute alcoholic hepatitis and development of Pneumocystis jirovecii pneumonia. The patient had none of the traditional immunosuppressing risk factors associated with Pneumocystis jirovecii pneumonia such as corticosteroid use, haematological malignancy or HIV infection. In the literature, there are two case reports and a case series of two patients which describe the development of Pneumocystis jirovecii pneumonia in acute alcoholic hepatitis. However, all of these previously described cases include identifiable risk factors – namely corticosteroid use and HIV infection. This case suggests that special consideration should be given to Pneumocystis jirovecii pneumonia as a cause of opportunistic infection in acute alcoholic hepatitis.
Introduction
Patients who present to hospital with acute alcoholic hepatitis (AAH) are at significant risk of bacterial infection. 1 However, in addition to typical bacterial pathogens, it is important to consider the possible presence of atypical or opportunistic pathogens.
We report the case of a 63-year-old man presenting with AAH who had findings suggestive of Pneumocystis jirovecii pneumonia (PJP). He lacked any of the traditional risk factors such as HIV, corticosteroid use or haematological malignancy. To our knowledge, this is the first published case of presumed AAH developing PJP in the context of no other identifiable risk factors. We identified two case reports2,3 and a case series of two patients 4 with AAH who all developed PJP on a background of corticosteroid use or HIV infection.2–4 We present findings from the case which highlight the immunocompromised state of patients with decompensated liver disease and the difficulty of distinguishing between infection and colonisation with PJP.
Case presentation
A 63-year-old Caucasian gentleman presented to his General Practitioner with jaundice and weight loss over six weeks in the context of chronic alcohol excess. On assessment in the Acute Medical Unit, he also complained of a one-week history of worsening breathlessness and a cough productive of clear sputum. He denied chest pain or haemoptysis.
He had a background of a steatotic liver on abdominal ultrasound which was attributed to his alcohol excess. He also had a medical history of chronic obstructive pulmonary disease (COPD), previous endoscopic stapling of a pharyngeal pouch, bilateral cataract surgery, duodenitis, diverticulosis, mild peripheral neuropathy, depression and osteoarthritis. His medications included amitriptyline, omeprazole, mirtazapine and a salbutamol inhaler. He had not required previous courses of oral steroids for his COPD.
He initially reported his alcohol intake to be five bottles of wine per week. However, the clinical team strongly suspected that he was drinking more than this. This was based on subsequent collateral history that 90–100 empty bottles were found at his residence. He smoked three cigarettes per day and used 0.5 g of cannabis fortnightly. He denied high-risk sexual behaviour or intravenous drug use. He worked as a catering manager with no obvious exposure to organic antigens.
On examination, his oxygen saturations were 97% on room air, his respiratory rate was 21 min−1 and breath sounds were vesicular. Abdominal examination demonstrated jaundice, clubbing and hepatomegaly. Cardiovascular examination highlighted bilateral pitting oedema peripherally. A neurological examination was unremarkable. He was not confused.
A chest radiograph, electrocardiogram (ECG) and laboratory tests were performed. A transthoracic echocardiogram (TTE), abdominal ultrasound and non-invasive liver screen were all requested, and the patient was referred to the Hepatology team.
Investigations
Initial laboratory investigations demonstrated abnormal liver biochemistry (bilirubin: 164 µmol/L (0–20 µmol/L), alanine aminotransferase: 155 U/L (10–40 U/L), aspartate aminotransaminase: 211 IU/L (15–41 IU/L), alkaline phosphatase: 450 U/L (30–130 U/L) and albumin: 25 g/L (35–50 g/L)), and his international normalised ratio (INR) was 1.3. He was hyponatraemic (sodium: 124 mmol/L (133–146 mmol/L)) and had acute kidney injury (creatinine: 265 µmol/L (80–115 µmol/L)). His baseline creatinine two years previously was 65 µmol/L. Inflammatory markers were raised with a leucocytosis (white cell count: 17.1 × 109/L (4.0–11.0 × 109/L)), neutrophilia (11.8 × 109/L (2.0–7.5 × 109/L)) and increased C-reactive protein (66 mg/L (0–7.5 mg/L)).
Serological tests for HIV, hepatitis A, B, C, D, E and cytomegalovirus (CMV) were all negative. Epstein–Barr virus serology was in keeping with previous infection. Immunoglobulins were unremarkable and a liver autoantibody panel was negative. Alpha-1-antitrypsin, caeruloplasmin and iron studies did not suggest an alternative aetiology to alcohol for the liver disease.
The admission chest radiograph showed clear lung fields (Figure 1). The baseline ECG was unremarkable. Abdominal ultrasound performed on day 4 demonstrated a coarsened, enlarged liver with trace ascites. There was no evidence of splenomegaly (9 cm).
Chest radiograph on admission demonstrated normal sized heart with clear lung fields.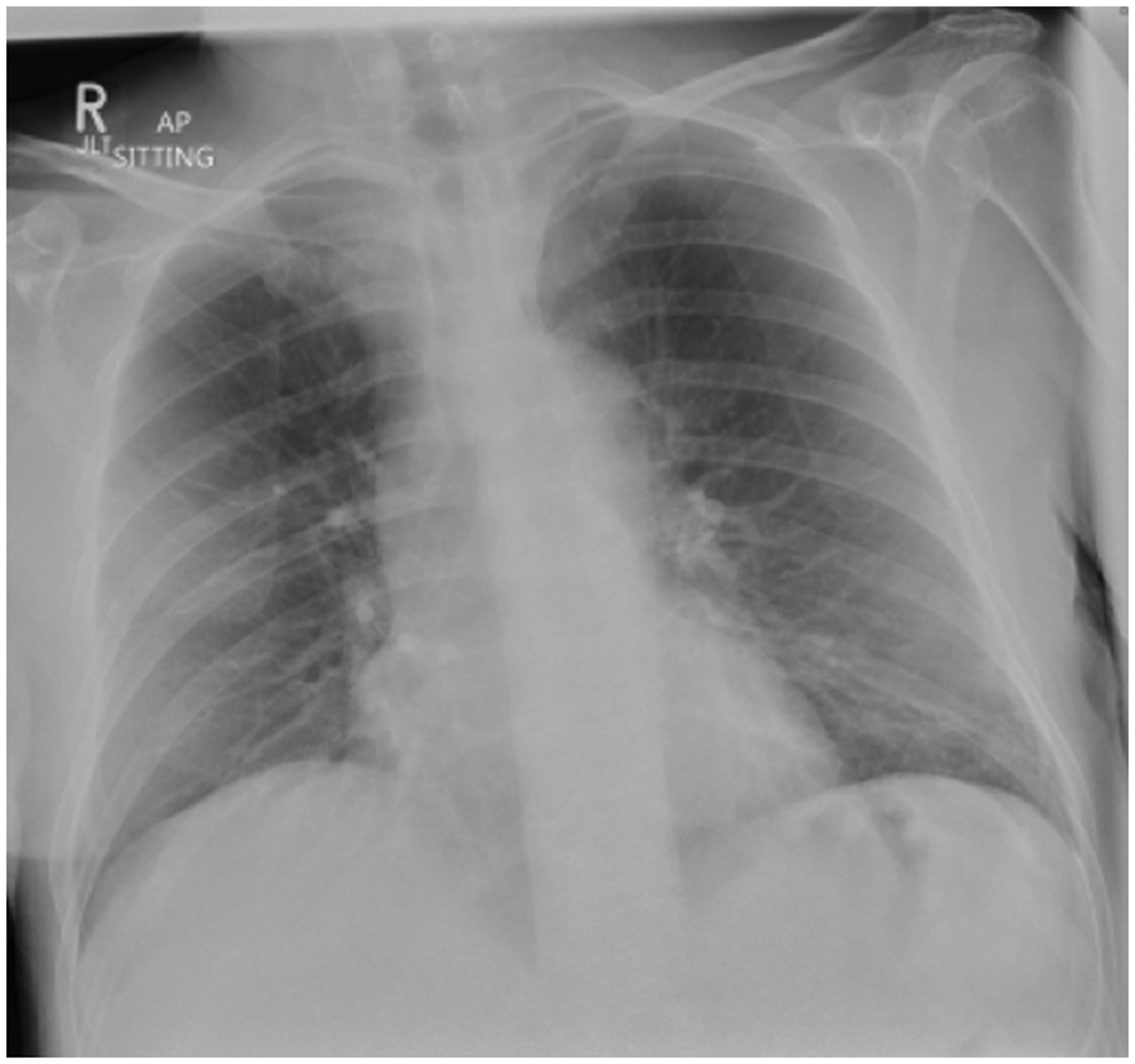
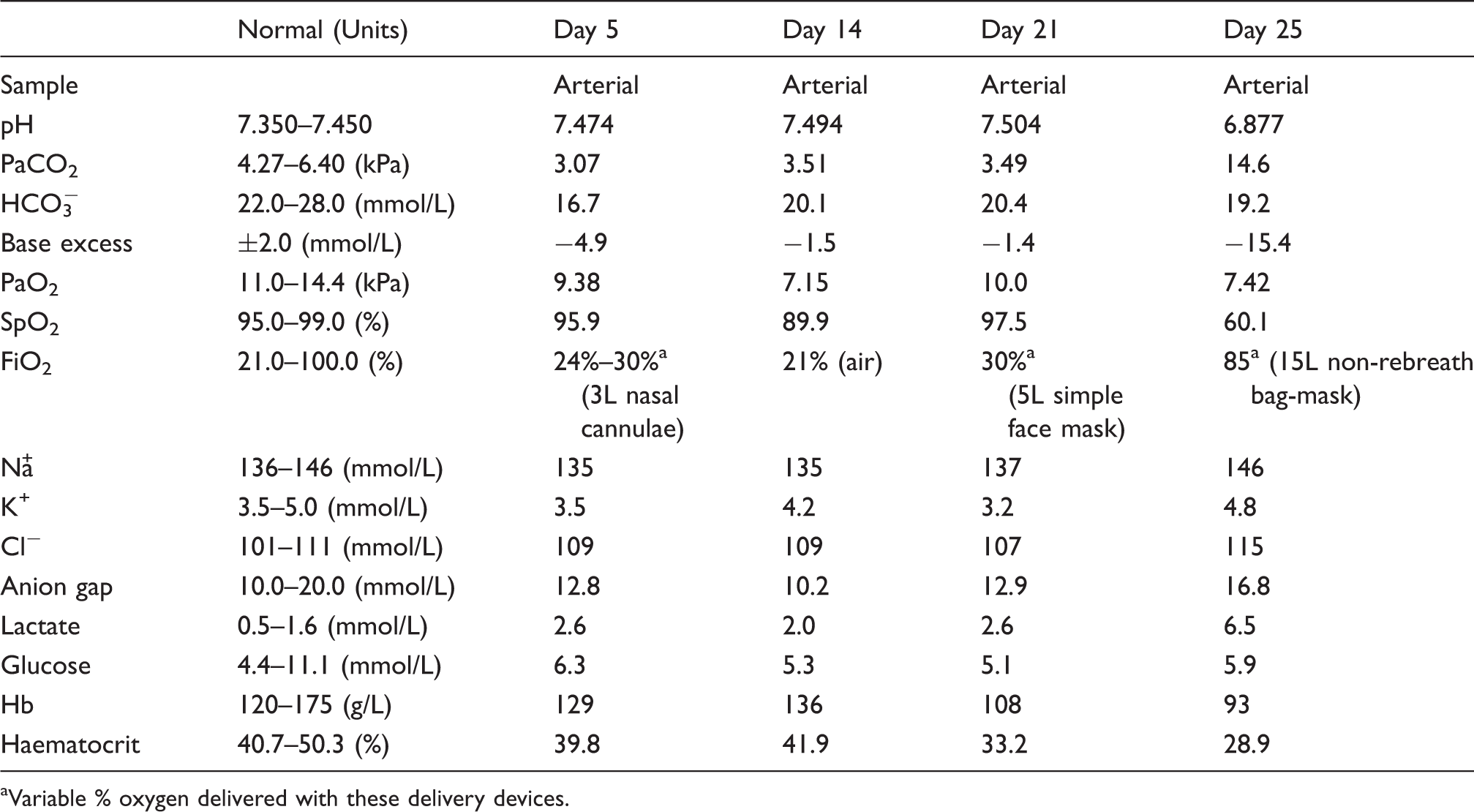
During the early course of the admission, the patient remained mildly breathless (Table 1, column Day 5). Although he had reported a clear sputum, he was unfortunately unable to expectorate a sample for microscopy and culture. He was empirically treated from admission with antibiotics. He received five days of intravenous (IV) co-amoxiclav as well as 72 h of IV gentamicin. After 5 days, his antimicrobials were switched to oral doxycycline to treat hospital-acquired pneumonia in accordance with local policy, which he finished on day 9. However, due to a paucity of signs on examination and the development of a low oxygen requirement, a computed tomography pulmonary angiography (CTPA) was performed on day 6 (Figure 2). This showed no radiological evidence of pulmonary embolism. However, the reporting thoracic radiologist observed that there was upper lobe predominant centrilobar emphysema as well as patchy ground-glass opacification seen throughout the lung lobes which, in the absence of pleural effusions, would be radiologically compatible with atypical infection or PJP. The possibility of PJP had not been proposed in the differential prior to the CTPA.
CTPA showing ground-glass opacification throughout all lung lobes with no associated pleural effusions. Arterial blood gas trend through the patient’s admission. Variable % oxygen delivered with these delivery devices.
Differential diagnosis
We felt that this patient’s presentation was consistent with decompensated liver disease and were confident in making a clinical diagnosis of AAH without biopsy. In our centre, we do not regularly perform a liver biopsy to confirm the diagnosis of AAH. This is due to concerns about potential complications of the biopsy as well as the practical issue of performing a transjugular biopsy and the time required for histology interpretation. This clinical approach is in keeping with the view of colleagues elsewhere in the United Kingdom. 5 However, what was less clear to us was the cause of his breathlessness. The broad differential we considered at the time included lower respiratory tract infection, exacerbation of COPD, atypical pneumonia, general deconditioning, heart failure, hepatopulmonary syndrome and pulmonary embolism. Patients with AAH and cirrhosis have impaired immune function and given the known increased prevalence of bacterial infection in patients with AAH we had empirically treated him with broad spectrum antibacterials before performing further investigations.
Treatment
PJP was considered following the computed tomography (CT) imaging. However, we felt that the presentation was not typical for PJP because of the absence of recognised factors causing altered host response such as in HIV infection, steroid use, haematological malignancy or previous organ transplant. In view of this, we decided to continue doxycycline. The patient made some subjective improvement. In view of the improvement, we felt that PJP was unlikely at this point. For this reason, we did not arrange a bronchoalveolar lavage (BAL) to confirm or deny PJP infection. The patient underwent a number of other investigations. These included a gastroscopy on day 11, which showed grade 1 oesophageal varices, and an echocardiogram on day 15 which showed normal biventricular size and function with no valvular abnormalities. He also received five days of IV flucloxacillin for a possible cellulitis secondary to a peripheral intravenous cannula.
However, rehabilitation was limited by ongoing breathlessness on exertion. On day 17, antimicrobials were recommenced owing to concern about his chest and a new requirement for nasal oxygen (Table 1, column Day 14). Ceftazidime and fluconazole were chosen based on local guidelines as well as increasing concerns about his being immunocompromised. In view of the previous CTPA result (Figure 2), the case was discussed with specialists in Respiratory Medicine and Microbiology, who recommended further investigations including sputum PJP, viral throat swabs, mycoplasma antigen, β-D-glucan and legionella antigen.
On day 17, an induced sputum sample was collected. This was the first respiratory specimen obtained during the admission. It was positive for PJP. Although microscopy was negative, the quantitative polymerase chain reaction (PCR) was significantly positive with a cycle threshold (CT) value of 11.2 (normal > 28). 6 After further discussion with Microbiology and then Respiratory Medicine, the patient was commenced on oral co-trimoxazole for probable PJP. This was subsequently escalated to intravenous cotrimoxazole after four days due to increasing oxygen demand (Table 1, column Day 21). His liver biochemistry remained relatively static (bilirubin: 132 µmol/L, INR: 1.0 and albumin: 32 g/L). His renal function had improved since admission (Na: 142 mmol/L, Cr: 123 µmol/L). Serum beta-D-glucan was measured on day 21 of admission. It was <44 pg/mg (negative).
Outcome
After receiving two days of IV co-trimoxazole, a chest radiograph (Figure 3) revealed widespread interstitial change with patchy airspace shadowing in the right lower zone. He then acutely deteriorated with profound mixed respiratory and metabolic acidosis leading to a cardiac arrest (Table 1, column Day 25). In view of his poor nutrition despite nasogastric feeding, his persistent jaundice and declining functional state, the decision was made to abandon initial resuscitation efforts. The case was reviewed at the internal medical examiner group after his death where other contributing factors to this acute deterioration were considered, such as fluid overload from IV co-trimoxazole administration and concurrent bacterial pneumonia. However, after discussion, the cause of death was documented as PJP.
Radiological deterioration with widespread interstitial change and patchy airspace shadowing in the right lower zone with a shallow pleural effusion.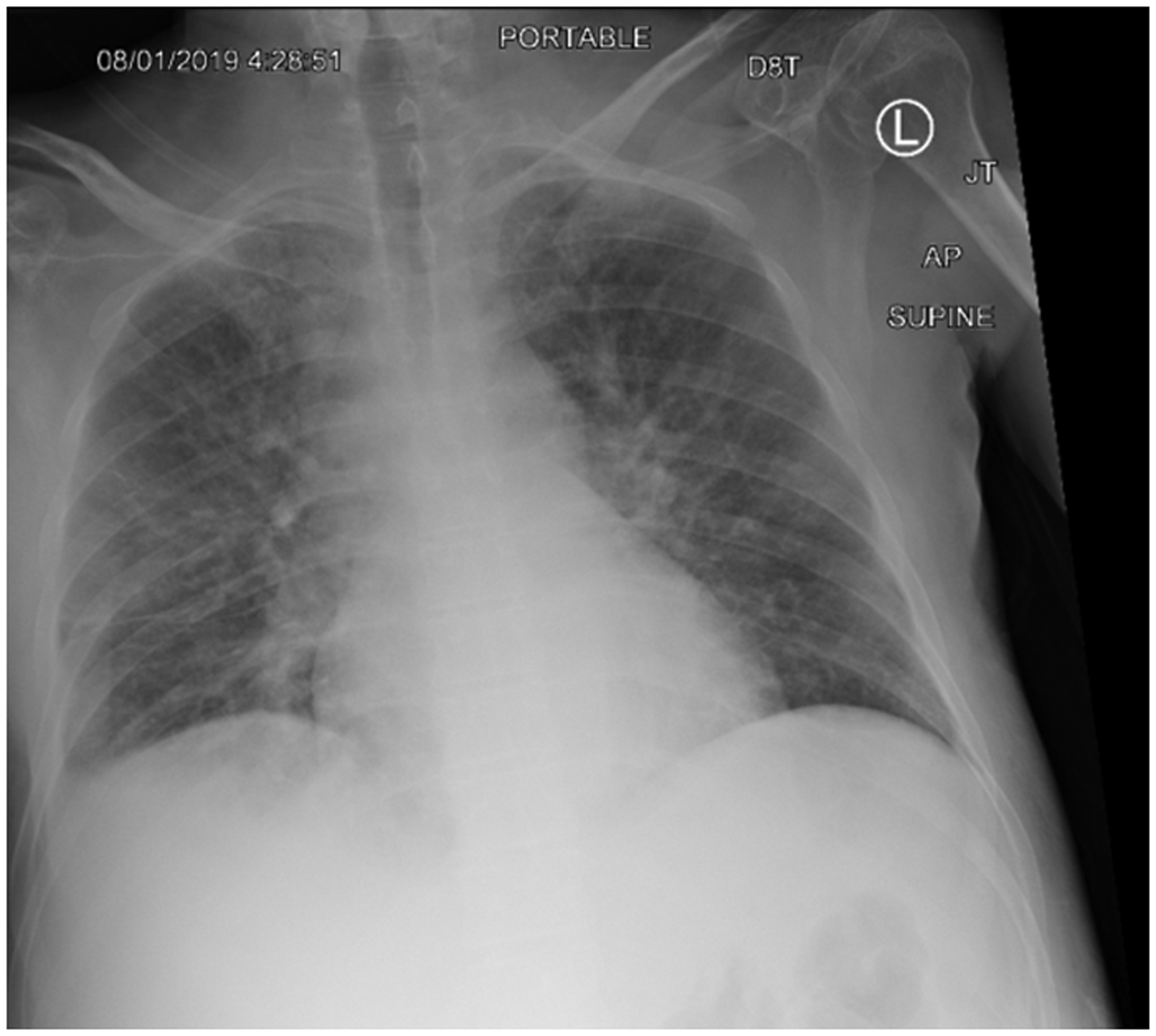
Discussion
Bacterial infection is the most common cause of acute decompensation in patients with cirrhosis. 7 This is associated with a high mortality, often in excess of 30%. 8 Observational studies show that 39% of patients with underlying alcohol-related liver disease (ArLD) develop infection at admission or during hospitalisation. This is 1.4 times greater than non-alcohol-related cirrhosis. 9 The mechanisms responsible for the increased risk of infection in liver disease involve impaired host innate and adaptive immune response, bacterial overgrowth and bacterial translocation. 10
Pneumonia accounts for 14% of all infections in liver cirrhosis and is most common in ArLD. 1 People who consume excess alcohol appear to be predisposed to typical respiratory pathogens such as Streptococcus pneumonia as well as Gram-negative bacteria and atypical pathogens, including Legionella pneumophilia and Mycobacterium tuberculosis. 10 Given their relatively immunocompromised state, it may be important to also consider opportunistic infections.
One question in this case was whether PJP was the causative organism and directly contributed to the patient’s deterioration. Opportunistic infection with PJP broadly manifests in two categories of patients: (1) HIV-infected population and (2) HIV-negative immunocompromised population. Although patients with liver cirrhosis and AAH are to some extent immunocompromised, the incidence of PJP infection is less well described than in other immunocompromised states such as haematological malignancy. We identified two case reports and a case series of two patients. The first case report is of a HIV-negative patient with liver cirrhosis and AAH, treated with corticosteroids, who subsequently developed PJP and CMV. This was confirmed by BAL PCR. The patient died despite treatment with co-trimoxazole and ganciclovir. 2 The second case report describes another HIV-negative patient with liver cirrhosis and AAH who was treated with corticosteroids. The patient died following a gastric ulcer haemorrhage. PJP and CMV were identified at post-mortem. 3 The case series describes two HIV-infected patients with AAH, both of whom received corticosteroids and went on to develop severe PJP. Both patients died. 4
The most significant risk factors predisposing to PJP development in HIV-negative patients are corticosteroid use and defects in cell-mediated immunity. 11 PJP in HIV-negative patients portends a poor prognosis with mortality rates as high as 30%–60%. 12 The diagnosis of PJP can be difficult in view of its non-specific features and the possible presence of other superimposed infections. Although bilateral perihilar interstitial infiltrates are the classic features of PJP on imaging, there is a wide heterogeneity of the radiographic features described. 13
If PJP is suspected, there are useful investigations that can be performed with good sensitivity and specificity to aid making a diagnosis. The difficulty is that PJP cannot be cultured and therefore it requires a high clinical suspicion in order to perform appropriate investigations. Key investigations include initially obtaining an induced sputum or BAL sample followed by one of staining, fluorescent antibody staining or PCR assay. For induced sputum specimens investigated by PCR, such as the case described, the sensitivity and specificity are 90% and 94%, respectively. For the same sample tested with fluorescent antibody staining, the specificity is similar but sensitivity drops to 82%. For BAL specimens, sensitivity and specificity are 98%–100% with PCR. 14
In this case, PJP DNA was detected through quantitative PCR assay on induced sputum. The CT in PCR refers to the threshold number of PCR cycles run to amplify the nucleic acid matter before the fluorescent signal is picked up. It inversely correlates with fungal burden in BAL specimens and accurately discriminates between infection and colonisation in both HIV-infected and HIV-negative patients. 6 The CT value of 11.2 in the above patient was deemed significantly positive and strongly suggests infection. A CT value below 28 [95% confidence interval, 26–30] in BAL samples is consistent with PJP infection. 6
The organism cell wall component, beta-D-glucan is another diagnostic marker. It is also found in the cell wall of pathogens other than PJP. A previous retrospective study has found it to have a negative predictive value (NPV) of 99.8%. 15 However, in the study, 45 of 50 patients presented with an acute, severe presentation which clinically and radiologically was deemed typical of PJP. Therefore, the spectrum of disease studied was not representative of mild or late presentations. The PJP group and control group in this study were not similarly matched. There were significantly less HIV-infected patients in the control group. Furthermore, the investigators were not blinded to the reference standard when they measured beta-D-glucan. A 2015 meta-analysis and systematic review adds further weight to our cautious interpretation of beta-D-glucan in HIV-negative patients. 15 It concluded that a negative beta-D-glucan was insufficient to rule out PCP in HIV-negative patients given its sensitivity of 85% and specificity of 73% in this population. 16 Therefore, in view of this evidence, we do not believe that the low beta-D-glucan can rule out a diagnosis of PJP in the case above, particularly when the PCR result and radiological findings suggested PJP.
This case illustrates many of the challenges of definitively diagnosing PJP infection versus PJP colonisation for clinicians. 17 Distinguishing between infection and colonisation in patients is important because it affects treatment. The main challenges in making the diagnosis include lack of in vitro culturing methods, variability in microscopy techniques and user experience, low fungal burden, clinician interpretation of both PCR assays and serological beta-D-glucan testing.
In line with the British HIV Association (BHIVA) guidelines this patient was started on co-trimoxazole orally and then escalated to intravenous treatment following clinical deterioration. He did not receive intravenous corticosteroids, which may be given in moderate to severe cases (PaO2 < 9.3 kPa). 18 Corticosteroids were not commenced in this case because their indication is strongest for HIV-infected patients, with evidence that for HIV-negative patients the use of early corticosteroids does not alter outcomes. 19
The patient demonstrated deteriorating respiratory function in the context of decompensated ArLD. The lack of improvement in the context of the CT findings prompted sputum sampling for PJP, which was subsequently positive. Although the patient lacked the traditional risk factors described in the development of PJP, he was nevertheless still immunocompromised. Based on the findings, we acknowledge that this case remains a probable diagnosis of PJP. Additional respiratory specimens, an induced sputum or BAL specimen at an earlier stage may have informed management.
Learning points/Take home messages
Development of infection is a significant concern in patients with AAH. Careful consideration should be given to their relatively immunocompromised state and the possibility of opportunistic infection such as PJP. This case serves to underline the difficulty in confirming infection due to PJP and the importance of obtaining the relevant microbiology specimens in a timely manner to inform management appropriately.
Footnotes
Authors’ Contributions
All authors contributed equally to this work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.