
Abstract
Aim
To present our national case series on primary thyroid squamous cell carcinoma (PTSCC) and add to the current literature about this rare and aggressive disease.
Methods
Scottish pathology departments were contacted and asked to provide details of patients with the diagnosis of PTSCC from the last 10 years. Three patients were included.
Results
Patients 1, 2 and 3 underwent surgical resection. Patients 1 and 3 went on to receive chemoradiotherapy. Patient 1 received nivolumab. Patient 1 died 10 months following diagnosis. Patient 2 and 3 are currently living with no recurrence, over two years post-diagnosis.
Conclusion
This case series has demonstrated an unusually good set of outcomes for a classically rapidly progressing disease with poor survival rates. This raises the question whether there is a subgroup of PTSCC associated with better outcomes and lower mortality. A patient-centred approach will give optimal patient management.
Introduction
Primary thyroid squamous cell carcinoma (PTSCC) makes up 0.7% of thyroid malignancies 1 and is an aggressive disease with a high mortality rate. Historically, the literature has been scarce and primarily comprised of cadaveric studies. In the last 20 years, there has been a greater volume of case reports regarding thyroid squamous cell carcinoma (SCC).
The initial presentation of PTSCC is most often a neck lump. This is an aggressive disease, so the neck lump is usually fast growing and associated with symptoms of compression such as dysphagia and hoarseness. 2 At presentation, patients often have local or distant spread. Important differentials to exclude are metastatic spread from a distant primary or local invasion into the thyroid gland. 3 The advanced stage of PTSCC at presentation often means that there are no curative options available, and these patients are frequently managed with palliative intent.1,2
This national case series aims to add to the limited literature surrounding thyroid SCC and focus on the treatment and outcomes of these patients.
Methods
Pathology departments across Scotland were contacted and asked to provide community health index (CHI) numbers for patients with a diagnosis coded on their systems as ‘thyroid squamous cell carcinoma’, from 2009 to 2019. CHI numbers for 27 patients were returned. Only three patients were included for our case series. Reasons for patient exclusion included: SCC of a distant site metastasising to the thyroid, local invasion of SCC into the thyroid from an adjacent site, mis-coding of diagnosis and duplication of patient records. The individual patient records were then reviewed to obtain clinical and demographic information.
Results
Patients 1 and 3 were male and Patient 2 was female. Patient age ranged from 43 to 74. All patients initially presented with a neck lump. Patient demographics, treatment and disease progression are summarised in Table 1.
Patient demographics, treatment and disease progression.
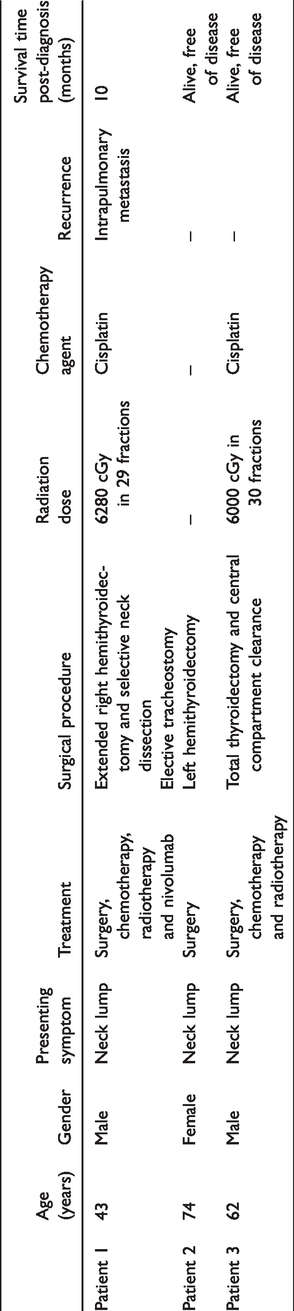
Patient 1 presented with a four to six-week history of a large goitre and difficulty swallowing. The patient had a fine needle aspiration (FNA) of a nodule under ultrasound (US) guidance that showed appearances suspicious of a malignancy. Extended right hemithyroidectomy with selective neck dissection was carried out. Pathology specimens taken intra-operatively and subsequent imaging resulted in a diagnosis of PTSCC, stage T3 N0. Patient 1 was treated with high-dose steroids, cisplatin chemotherapy and radiotherapy. The radiotherapy course was intended to be 30 fractions over six weeks, but only 29 fractions could be carried out due to stridor and distress during treatment. An elective tracheostomy was undertaken for symptomatic relief from shortness of breath and stridor. Seven months following resection, computed tomography (CT) scan showed recurrent SCC enveloping the great vessels that was inoperable. Patient 1 was treated with seven cycles of nivolumab 3 mg/kg every two weeks. Two months after treatment, intrapulmonary metastases were noted on CT, and the patient passed away shortly after.
Patient 2 presented with a short history of a neck lump. FNA and US imaging was carried out, and pathological assessment diagnosed Thy2 U5. CT showed a mass within the left lobe of the thyroid, consistent with malignancy and an enlarged level VI lymph node, stage T3 NX. A left hemithyroidectomy was carried out, and a diagnosis of PTSCC was made from pathology specimens. The patient was discussed with the multidisciplinary team (MDT), and a decision was made that radiotherapy was not to be carried out unless patient became symptomatic and required palliative symptomatic control. Patient 2 has been followed up for over two years post diagnosis and is currently living with no evidence of recurrence.
Patient 3 presented with a rapidly expanding right-sided thyroid mass. FNA showed a large cell lesion. Patient 3 had a CT scan that showed a right thyroid mass with peri-thyroid extension and a suspicious paratracheal node. They were treated with a total thyroidectomy and central lymph node compartment clearance. Pathology diagnosis was PTSCC with nodal spread and a satisfactory resection. The patient received adjuvant chemoradiotherapy in the form of one cycle of cisplatin and 6000 cGy in 30 fractions of external beam radiotherapy. Patient 3 has been followed up for over two years post-diagnosis and is currently living with no evidence of disease recurrence.
Discussion
PTSCC is a rare condition, and we have identified only three reported cases in Scotland in the last 10 years. Information Services Division (ISD) has published cancer statistics about the incidence of head and neck cancer, with the most recent data reported from 2017. 4 From 2007 to 2017, there were 2724 cases of thyroid cancer in Scotland. 4 From the data presented in this national case series, PTSCC makes up 0.001% of thyroid cancer in Scotland.
The literature regarding PTSCC demonstrates an aggressive disease with a high mortality rate. PTSCC is more common in females and the elderly population. Tumours are rapidly growing and can be large (>5 cm) at time of presentation. 2 Symptoms such as dysphagia, dyspnoea and hoarseness can be associated with compression from the tumour mass and can often be present at primary presentation. These patients may have local and regional lymph node involvement and distant metastases at presentation. The most common site of metastases is the lung. Diagnosis of PTSCC requires exclusion of distant primary disease that has spread to the thyroid. 5 Tumours of the kidney, lung and breast are the most common to metastasise to the thyroid gland. 5 Despite surgical resection and adjuvant chemoradiotherapy, disease progression is reported to be rapid and associated with a high mortality rate.1,3 Overall survival rates at two years post diagnosis have been reported as only 18%. 2
The pathophysiology of PTSCC is theorised but unconfirmed. The thyroid gland does not contain any squamous cells. It has been hypothesised that this tissue develops from embryological remnants of neighbouring structures, such as the thyroglossal duct. 6 Other theories suggest that inflammatory or malignant processes result in metaplastic squamous cell changes. 6 It has been suggested that PTSCC can develop following radiation to the thyroid. 5
Treatment options which have been employed for these patients include surgical resection, chemoradiotherapy, biological agents and multimodality treatment regimes. Surgical resection has been shown to improve overall survival rates. 2 This may reflect that patients fit for surgery have fewer co-morbidities and less advanced disease. Surgical intervention may also improve survival rates by reducing disease burden and the spread of disease. Resection may also help with symptom control and can be used curatively or palliatively to relieve symptoms such as partial airway obstruction.
Radio- and chemotherapy can be used in conjunction or individually as adjuvant therapies to surgery. In our series, two of the three patients received chemoradiotherapy. However, there are contrasting views in the literature on the association between radiation, chemotherapy and survival. It has been suggested that thyroid SCC has a poor response to chemoradiotherapy due to resistance. 7 Au et al. 2 found no improvement in survival outcomes in patients who received radiotherapy or chemotherapy. The patients who receive these adjuvant therapies are likely to have locally advanced disease or metastatic spread. However, the combination of surgical resection and radiotherapy has been associated with the best survival outcomes.6,7
Patient 1 was treated with nivolumab, a human monoclonal antibody which inhibits programmed cell death protein 1. It has been used in patients with recurrent head and neck SCC and has been shown to prolong survival compared to standard single-agent therapy. 8
This case series presents an unusual set of outcomes for PTSCC. Disease progression seen in Patient 1 is typical of the aggressive nature of PTSCC with recurrence and mortality at six months post-diagnosis being common. Patient 3 was treated aggressively and is now living disease-free over two years post-diagnosis. Patient 2 is particularly uncommon. Patient 2 was treated by surgical resection limited to the involved hemi-thyroid and is alive and disease free over two years post-diagnosis. In the literature, patients who are alive at follow-up have typically been treated with extensive surgical resection and adjuvant therapy.9–11 The authors have been unable to find another documented case in the literature that demonstrates a patient surviving over two years post-diagnosis who received only surgical resection. The case of Patient 2 suggests that there may be a subgroup of PTSCC with a less aggressive disease profile. It is unclear if adjuvant therapies provide survival benefit in patients treated aggressively. Given the rarity of the disease, it is unfeasible to carry out an effective study to determine the benefits of adjuvant therapy. The authors suggest that the treatment of this disease should be patient centred, as there is little evidence base. The benefits of adjuvant therapies must be weighed against their side effects, especially in elderly and frail patients. For these patients, symptomatic relief and palliation where appropriate, is a key aspect of management. 12
Conclusion
This case series has demonstrated an unexpected and interesting addition to the current literature on PTSCC. Poor outcomes and high mortality rates are seen in the majority of cases. An unusual case of limited treatment and survival over two years post-diagnosis may indicate a less aggressive subgroup of PTSCC. Realistic medicine and a patient-centred approach are important in the management of these patients.
Footnotes
Acknowledgement
We would like to thank Douglas McLellan, consultant pathologist NHS Greater Glasgow and Clyde who helped gather information for this case series.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.