
Abstract
Introduction
Invasive coronary angiography (ICA) is associated with higher complication rates in patients following coronary artery bypass surgery (CABG). CT coronary angiography (CTCA) has emerged as an attractive alternative. We assessed the impact of CTCA on subsequent ICA.
Methods
We identified 213 CABG patients undergoing CTCA between 2015 and 2018. In 151 the indication was suspected recurrence of angina. We then identified patients undergoing ICA within 1 year of CTCA.
Results
CTCA obviated the need for ICA in 115 cases (76%). CTCA was better at identifying targets for percutaneous coronary intervention (PCI) to saphenous vein grafts (SVG’s) than to native vessels (89% vs 47%). 7 out of 10 lesions of “probable” significance by CTCA proved flow-limiting, and 4 out of 13 “indeterminate” lesions. CTCA concordance was 97% for left internal mammary (LIMA) grafts.
Conclusion
CTCA directed management in a majority of patients without ICA. It identified a cohort of patients likely to be candidates for SVG PCI, but was less effective in identifying PCI targets in the native vessels. CTCA renders invasive LIMA cannulation redundant unless a target lesion is suspected.
Keywords
Introduction
Cardiac computer tomography coronary angiography (CTCA) is a well-established first line imaging modality for the assessment of patients with chest pain with low-to-intermediate probability of coronary heart disease (CHD). 1 Since 2011, its use has increased almost 3-fold in the United Kingdom driven by its strong sensitivity and powerful negative predictive value. 2 Multi-slice detectors can acquire images in a rapid fashion with less contrast use, radiation exposure and overall cost when compared to invasive coronary angiography (ICA). 3
In patients with previous coronary artery bypass grafting (CABG), CTCA offers potential advantages over ICA. The need for an effective diagnostic modality in this patient cohort cannot be understated. It is estimated that 25% of venous bypass grafts are occluded within five years of surgery. 4 ICA remains the standard invasive option, but risks include myocardial infarction, stroke from catheter embolization and mortality. 5 CABG patients also present additional complexities. 6 Identifying graft location and achieving successful co-axial cannulation can also be more problematic if the precise anatomy is not known beforehand. 7 These complicating factors result in longer procedure times, greater radiation exposure and contrast use, and a higher risk of renal injury and graft dissection. CTCA by contrast is more accurate in evaluating both graft anatomy and patency (sensitivity 98%, specificity 97%). 8
A strategy of performing adjunctive CTCA in CABG patients before ICA is yet to be fully established, but could allow graft and coronary anatomy to be charted beforehand to supplement the assessment of whether invasive revascularisation is required. Any subsequent ICA procedure could then be focused towards the target lesions.
We sought to examine the real-world utility of CTCA in patients who have undergone CABG, and its implications for clinical management at a large Scottish tertiary referral centre.
Methods
We retrospectively identified all patients with previous CABG who were referred for elective CTCA between 2015 and 2018 at our tertiary referral institution. The choice of CTCA as imaging modality was entirely at the discretion of the referring cardiologist, and we did not have comprehensive information regarding preceding non-invasive testing if any. All studies were performed using a GE Discovery CT750 HD 64 slice multi-detector computed tomography (MDCT) scanner. Coverage was from diaphragm to lower neck and scan timing was derived using the test bolus method. Sequential scanning with mid-diastolic prospective ECG-triggering was used wherever possible. Padded or retrospective helical scan modes were employed at higher heart rates at the discretion of the supervising Physician/Radiologist. Dose parameters and contrast material volumes were selected according to patient size.
Each report was analysed to identify the indication for the scan, and the classification of the stenosis. Left internal mammary artery (LIMA) and non-LIMA graft lesions were reviewed separately. Lesions in the graft and native vessels were grouped into “probable” (severe) or “possible” (moderate or indeterminate) stenoses. All patients who underwent further ICA and/or percutaneous coronary angiography (PCI) within 1 year of the index CTCA scan were reviewed to evaluate the correlation between modalities.
Results
In total, 213 patients were studied. The main indication for CTCA post-CABG was angina (71% of patients). In 115 of 151 (76%) cases, the CTCA findings guided management to successfully obviate the need for further ICA (Figure 1).
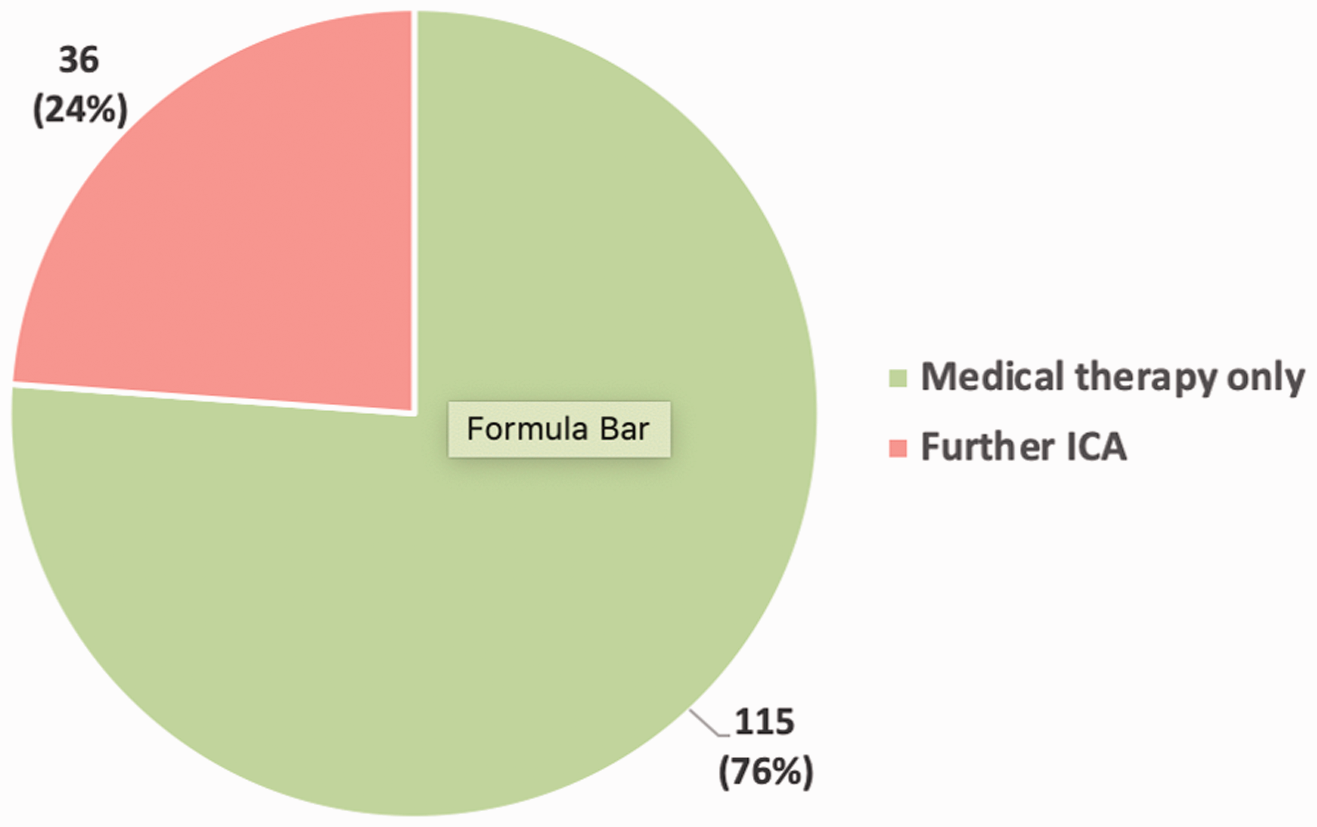
Follow on assessment after CTCA in patients with suspected ischemic symptoms.
39 patients (18%) underwent further ICA after CTCA. In this group CTCA had identified a total of 71 patent grafts and 31 occluded grafts. Both LIMA and non-LIMA grafts were reviewed in turn (Figure 2).
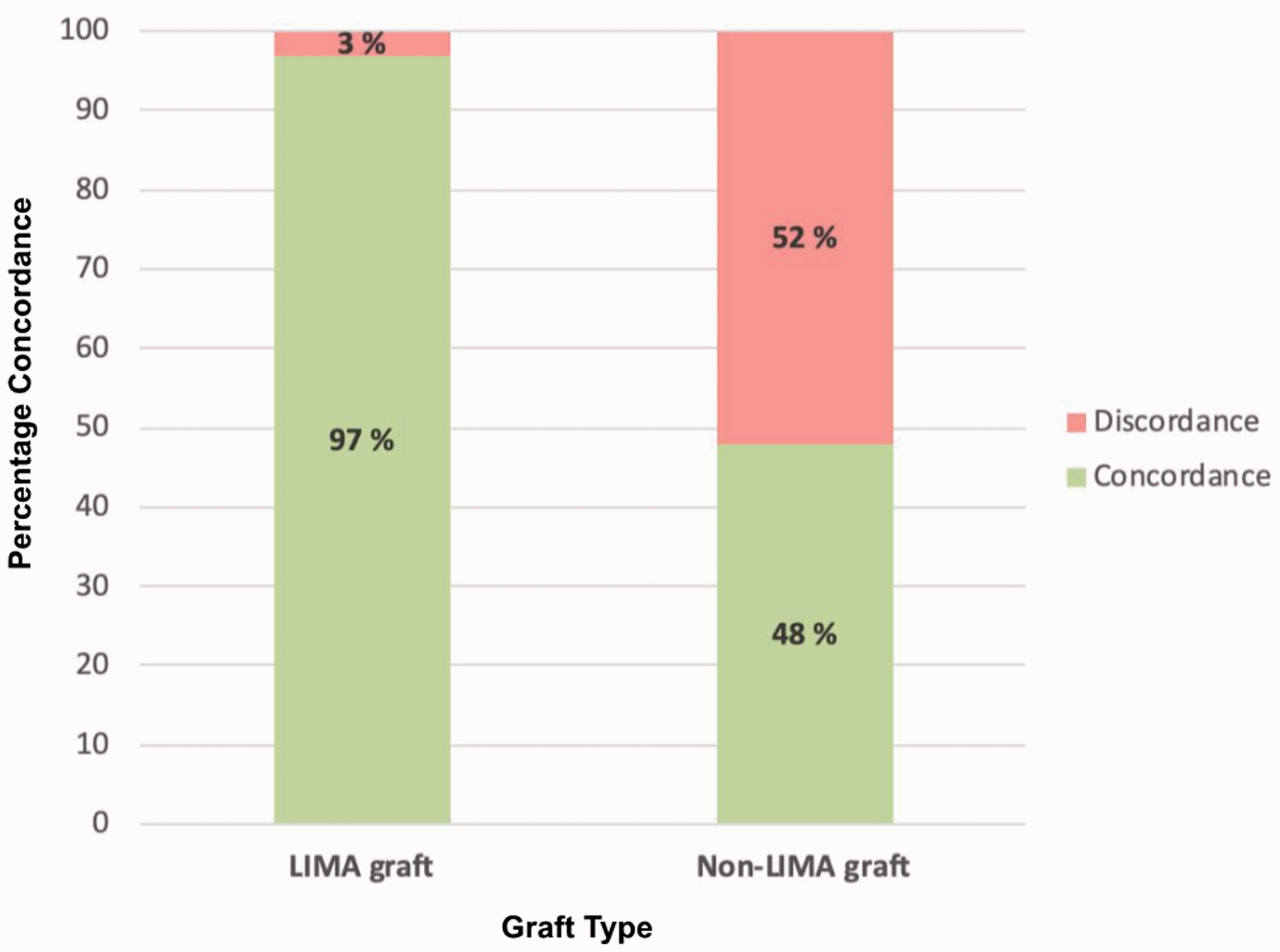
Concordance between CTCA and ICA – by graft type.
Out of 38 LIMA grafts imaged by CTCA, 29 were fully patent, 7 occluded, and there was 1 pre-existing insertional stenosis. Additionally, there was 1 case of subclavian stenosis. During subsequent ICA, selective cannulation was performed in 30 of 38 patients (79%). Complete concordance between CT and ICA was observed in 29 of these 30 (97%) of cases.
For non-LIMA graft lesions, concordance was poorer. CTCA identified 10 “probably” and 13 “possibly” significant stenoses. Following ICA 7 out of 10 of those graded as “probably” significant by CTCA, and 4 of 13 graded as “possibly” significant were adjudged to be flow limiting.
CTCA was better able to distinguish lesions for intervention in graft vessels compared to native vessels (Figure 3). In total, 26 of 39 patients (67%) underwent attempted PCI. In 9 cases intervention was undertaken to the graft vessel, and in 17 cases PCI was performed within the native vessel. CTCA correctly identified specific target lesions in 8 of the 9 patients undergoing graft PCI, but this concordance was lower for native vessels (only 8 of the 17 lesions). One graft lesion was “missed” by CTCA and this was adjudged retrospectively to be due to step artefact.
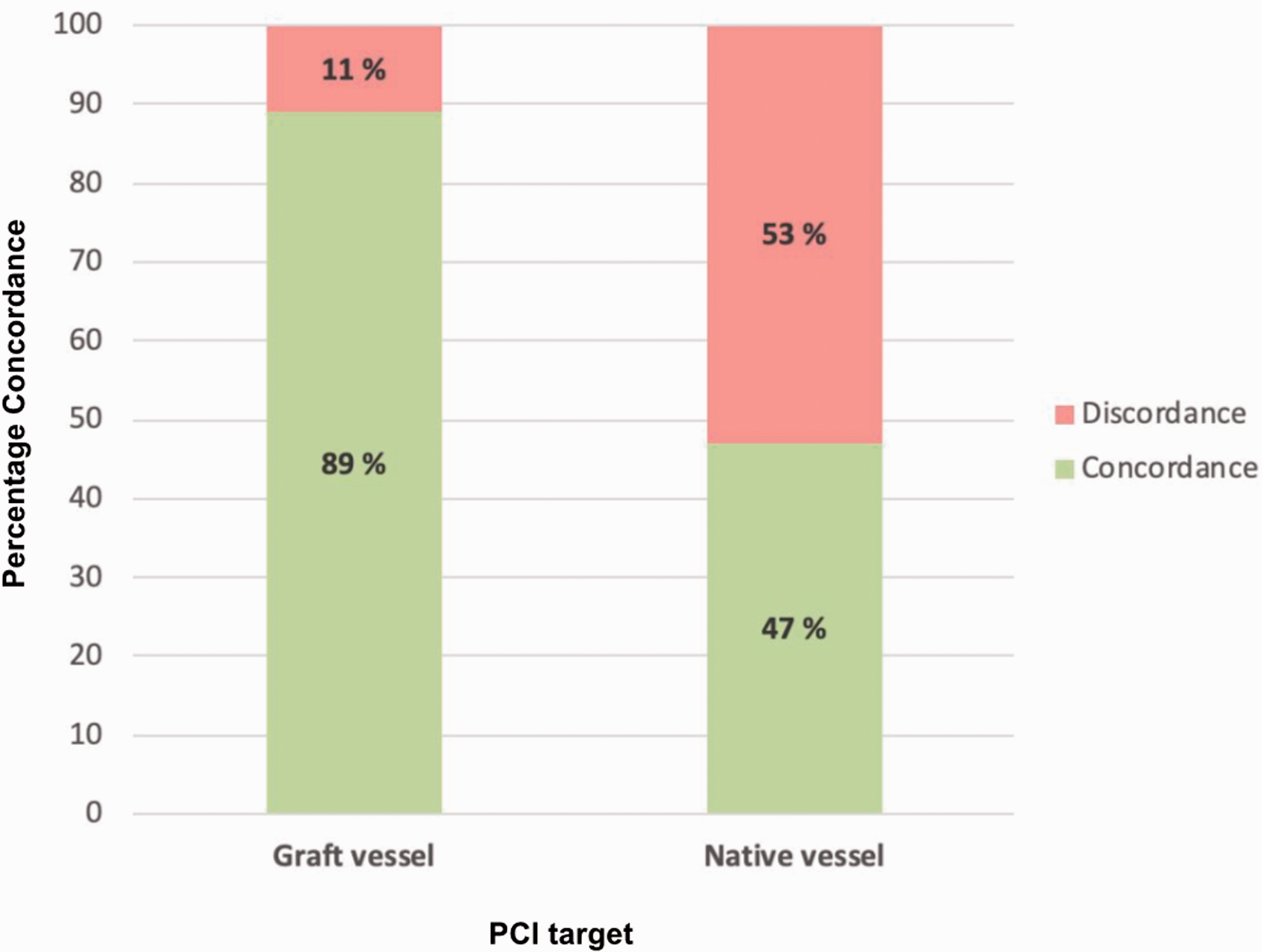
Concordance between CTCA and ICA for identifying appropriate PCI target – by vessel type (PCI: percutaneous coronary intervention).
Discussion
The high failure rate of venous grafts in CABG patients has produced a clear need for an effective imaging modality. 9 Our study demonstrated that CTCA can provide valuable additional information when utilised as an adjunctive assessment during coronary evaluation for patients with pre-existing CABG. In 76% of cases, the up-front use of non-invasive CTCA was able to re-direct management away from further ICA thereby producing significant potential cost savings and lowering the exposure of patients to contrast material, radiation and the clinical risks of further invasive procedures.
The role of CTCA as an adjunct for pre-procedural planning to guide ICA has also been furthered. In many causes where graft patency has been established, CTCA can obviate the need for graft re-cannulation. If re-assessment is required, pre-procedural mapping of graft ostial can the reduce additional radiation exposure and contrast use associated with unguided probing during ICA. In another single central observational study, prior CTCA appeared to reduce ICA time, and cumulative contrast burden and radiation dosing. 10
In our series we were able to demonstrate how confirmation of LIMA graft patency might alleviate the need for selective cannulation during ICA. This is an important finding since LIMA cannulation poses additional challenges. Firstly, due to its acute origin from the subclavian artery, extensive mediastinal course and smaller lumen, there is a risk of vessel dissection which – given the substantial volume of anterior myocardium subtended – is likely to produce significant myocardial damage and necessitate either emergency redo cardiac surgery or complex bailout PCI.11,12 Secondly, access must be via either the left radial or the femoral route. Left trans-radial access increases the technical complexity of the procedure and results in longer procedure times, contrast use and often lowered angiographic success.13,14 The transfemoral route is also hindered by additional vascular site complications arising from arterial puncture. Thirdly there exists the feared risk of ischemic stroke due to the proximity of the LIMA origin to the left vertebral artery in particular. 15
CTCA unsurprisingly proves better at imaging graft compared to native vessels. Graft vessels have less movement artefact, a wider luminal diameter and tend to be less calcified. Conversely the limited temporal and spatial resolution of CTCA hinders luminal visualisation in the native circulation. This is a particular challenge in CABG patients, in whom the process of atherosclerosis is more severe, often resulting in heavily calcified vessels. The resultant beam hardening and blooming artefacts often restrict or preclude luminal visualisation. In turn this means that it can be difficult to identify native PCI targets in such vessels, particularly in the context of modern complex PCI options such as rotablation, which allow revascularisation of heavily calcified or even totally occluded vessels. It is possible that use of quantitative perfusion CT may ultimately overcome some of these obstacles to provide functional assessments of ischaemia, but current use remains hindered by limited accuracy and radiation burden.19
Technological enhancements will continue to improve the utility of CTCA. Prospective ECG gating (‘step-and-shoot’ scan) can deliver radiation at prespecified points of the cardiac cycle, dramatically reducing the overall dose by almost two thirds. 16 wide-detector array imaging or high helical pitch dual-source scanning can capture the entire heart within a single beat to reduce stair-step artefacts. Faster rotation times improve temporal resolution and reduce image degradation at higher heart rates,17,18 while better iterative reconstruction algorithms further reduce image noise. 16
Limitations
We have demonstrated that CTCA has limitations for evaluation of complex native disease, but we used an older 64 slice scanner. Newer scanner technologies (such as later generation wide-detector scanners and more advanced algorithms) might be anticipated to improve the imaging of native and bypass grafts and further strengthen the adjunctive value of CTCA before ICA.
It should also be noted that for this cohort of patients, we did not re-evaluate the diagnostic processes that lead to the choice of CTCA as imaging modality. If the referring clinician deemed that the patient had possible myocardial ischaemia then they were included in the analysis. The intention of the study was not to re-determine the value of CTCA compared to other non-invasive modalities in the assessment of ischaemic disease. Similarly we did have follow up information to judge why three-quarters of patients did not undergo invasive angiography following CTCA.
Finally, whilst this study was performed at a major tertiary referral centre, it remained a single site observational study. Increasing the numbers of patients in our cohort would have allowed for improved validation of data, though a wide sample of patients were studied. Our conclusions are in keeping with emerging findings, but it is intended to stimulate further research and discussion. We believe that a randomised study of pre-procedural CTCA before ICA in CABG patients is required to help definitively quantify the utility of CTCA in this population.
Conclusion
CTCA can identify a cohort of patients likely to be candidates for PCI post-CABG. In our study, CTCA identified specific targets for graft PCI with a high sensitivity, but was less effective for identifying targets for PCI in the native vessels, due to lesion and procedural complexity. Particularly high concordance was seen between CTCA and ICA for LIMA grafts, which should render the need for selective cannulation redundant, unless a target lesion is suspected. As the imaging quality of CTCA continues to develop, the incorporation of adjunctive CTCA into diagnostic pathways for coronary evaluation has the potential to improve clinical outcomes and optimise resource utilisation.
Supplemental Material
sj-pdf-1-scm-10.1177_0036933020936274 - Supplemental material for The value of non-invasive computed tomography coronary angiography in imaging patients with coronary artery bypass grafts
Supplemental material, sj-pdf-1-scm-10.1177_0036933020936274 for The value of non-invasive computed tomography coronary angiography in imaging patients with coronary artery bypass grafts by T Krysztofiak, F Ahmad, J Adams, DB Stobo, R Good and J Byrne in Scottish Medical Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.