
Abstract
Background and aims
Angiographic guidance for percutaneous coronary intervention (PCI) has significant limitations in interpretation. The superior spatial resolution of optical coherence tomography (OCT) can provide meaningful clinical benefits, although limited data is available on Asian populations. This study aimed to determine whether OCT can provide additional advantages and useful clinical information beyond that obtained by angiography alone in decision making for PCI.
Methods
This was an observational study based on a single tertiary cardiac center in Pakistan, which includes 67 patients who underwent coronary angiogram and stenting. Their pre and post stenting OCT findings were recorded. Any additional intervention was also recorded. The data were analysed using IBM SPSS software version 26.0.
Results
The mean age was 55.00 ± 9.00 years. Majority of the patients were males (65.7%). On angiography, there was an equal number of stable and ruptured plaques (38.8%). Post stenting results showed 29.9% under deployed stents and 34.3% were either undersized or mal-apposed. Out of 67 patients, 50 (74.6%) needed re-intervention after PCI. Among different procedures, post-dilatation was most common.
Conclusion
The main OCT benefit is in borderline lesions on CA, in whom OCT identifies significant coronary stenosis and leads to PCI indication in patients. In the post-PCI context, OCT leads to an indication of PCI optimisation in half of the coronary lesions.
Introduction
For half a century, coronary angiography has been used as the main modality for assessment and guidance during percutaneous coronary intervention (PCI). With its planar two dimensional imaging, it cannot provide intra-luminal details like the degree of stenosis, calcification, or type of plaque. To overcome the inherent limitations of angiography, intracoronary imaging modalities were designed.
Optical Coherence Tomography (OCT) is one of the modalities which uses infrared radiation for intracoronary imaging and improved spatial resolution. 1 With a superior axial resolution, OCT is superior to the intravascular ultrasound (IVUS), the other imaging technique for viewing the vessel morphology by using an ultrasound. 2 The resolution of OCT (10–20 μm) is 10-fold higher than that of IVUS (100–150 μm); however, as a consequence, the penetration depth is lower (OCT: 1–2 mm compared with IVUS: 4–8 mm). 3 Therefore, there is a limit in the ability of IVUS to detect intimal tears, thrombus and stent mal-apposition, whereas OCT has been demonstrated to visualise intimal hyperplasia, intraluminal thrombi, stent edge dissection and mural thrombus after PCI. 3
OCT provides improved intracoronary images of those elements which are close to the inner vessel wall. 2 It provides detailed information about the degree of stenosis, plaque morphology, the lumen diameter, and complications, which enables the operator to select an appropriate stent size.4,5 After stent deployment, OCT can visualise stent mal-apposition, edge dissection, and any geographical detail. This can guide in further intervention if needed as both stent under expansion, mal opposition and geographical miss can contribute to an increase in the rates of subsequent target vessel revascularisation by increased incidence of stent thrombosis or in-stent restenosis and subsequently major adverse cardiovascular events (MACE).6–8
OCT is not routinely used for coronary interventions mainly because there is a lack of uniformly accepted standards for stent optimisation in our institute. The main reason behind this is the paucity of adequately powered local trials. We, therefore, conducted this study to use OCT for the assessment of coronary artery disease and a guide to percutaneous coronary intervention and its impact on decision making in PCI for the first time in our region.
Methods
This was an observational study conducted at our institute after approval from ethical review committe and written informed consent was taken from all the participants. The sample size was calculated from an electronic software. Patients presenting to the catheter lab for PCI with age older than 18 years were enrolled in the study. The indication for using OCT was based on study protocols and was approved by the ethics committee of our institute. The inclusion criteria consisted of completeness of the pullback and good image quality as defined by >70% of analysable frames.
Image acquisition
OCT imaging was performed after the injection of nitroglycerine (100 to 150 µg). The intravascular OCT device (ImageWire, LightLab Imaging, Westford, MA, USA) was inserted into target arteries through a 6 or 7 Fr guiding catheter. Blood clearance was achieved by non-diluted iodine contrast injection at rates of 3 to 5 ml/s. Images were acquired with an automated pull back at a rate of 1 mm/s. Images were digitally stored and submitted for offline evaluation.
Image analysis
All images were screened for quality by two independent, experienced observers and excluded if the frames were of poor quality or with artifacts in any quadrant of the images. Inadequate blood clearance was noted and excluded. A dedicated semi-automated contour detection system (OCT system software B.0.1, Harvest Imaging) was used for OCT measurements. It is an auto calibrated system which allows us to measure the intima, media and any other structure within the vessel wall like stent struts, stent diameter, and stent expansion etc. In vivo scale is shown in green color and proprietary scale is shown in purple color for viewers to understand.
Coronary artery disease assessment
In non-stented arteries, the region of interest was selected based on anatomic landmarks as seen by angiographic images containing the OCT catheter position and declared as borderline on coronary angiogram. Plaque morphology was assessed and recorded by two experienced analysts. In the stented arteries, position and apposition, thrombus and neo-atherosclerosis were analysed and recorded. Mal-apposition values were obtained by 3600 chords, distributed between the lumen and stent contours. Neo-atherosclerosis was defined as occurring between stent struts with different transition optical properties.
Statistics
Data analysis was done using Statistical Package for Social Science (SPSS) version 26 (IBM Corp., Armonk, NY). Categorical variables are presented as counts and percentages, and continuous variables are presented as mean + standard deviation (SD).
Results
There were a total of 67 patients that participated in the study. The mean age of the participants was 55 ± 9 years. There were 44(65.7%) males and 23(34.3%) females. The demographics and baseline characteristics of the patients are shown in Table 1.
Demographics and clinical characteristics.

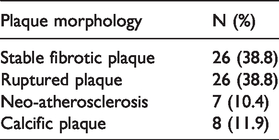
There were 26 (89.6%) patients of acute coronary syndrome (ACS) with plaque rupture and 3 (11.4%) with stable plaque. OCT in the native coronary artery and the plaque characteristics are shown in Table 2.
Plaque morphology in native coronary artery.
Post-stenting findings in the OCT are given along with the re-intervention if needed in Table 3.
Post-stenting OCT findings.
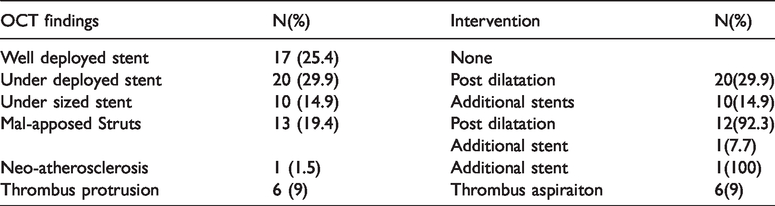
The complicated or mal-placed stents were treated using a re-intervention. Out of 67 patients, 32 patients (47.7%) were treated with post dilatation, 11 patients (16.4%) required additional stent placements and 6 patients (8.9%) needed thrombus aspiration.
Discussion
To our knowledge, this is the first in vivo study of coronary plaque morphology and intervention with OCT in various coronary presentations in Pakistan. In this single-center observational study, we evaluated the applicability of OCT in native coronary arteries for assessing the nature of the atherosclerotic process in different coronary syndromes and the feasibility of OCT for post-stent recognition of different processes leading to further interventions.
The findings of this study reinforces our understanding of the pathophysiology of coronary plaques and impediment of stent optimisation after coronary angiogram guided PCI. There was a trend towards fibrotic plaques (38.8%) in stable coronary artery disease (SCAD) and ruptured plaques (38.8%) in acute myocardial infarction (AMI). These findings indicate that lipid being the main component for a vulnerable plaque, it’s the fibrous cap which may be a prerequisite for rupture of a plaque leading to AMI or ACS.9–13 A study on IVUS showed plaque rupture in 66% of patients while our study suggested that almost 89.6% of the patients have plaque rupture in AMI. 14 This indicates that IVUS probably underestimates the incidence of plaque rupture. This can be because of the discrete sampling method and the IVUS study enrolled patients after 2 weeks of the acute event.
Baseline characteristics like hypertension (55.2% vs. 56.5%), and smoking (46.3% vs. 42.5%) were comparable to a study while dyslipidemias (37.3% vs. 55.9%) was less as compared to the patients in that study. Diabetes (56% vs. 27.5%) was more common in our patients. 10
There was no significant difference in plaque morphology between the two genders in our study. This is following various studies that compared men and women in terms of plaque characteristics through OCT.15,16
Another application of OCT is as an adjunct to coronary angiogram-guided PCI. Tedious structural details and information can be evaluated after coronary intervention with greater accuracy compared with IVUS.17,18 In our study, 74.6% of the patients required further interventions after PCI. This emphasises the need for an intracoronary imaging modality for optimal intervention. One study showed that 25% of the patients required stent optimisation by post-dilatation balloon. 18 A similar percentage (29.9%) is seen in our study. The reason can be a selection of comparatively smaller stents or inadequate lesion preparation based on angiographic views.
Our study had several limitations. It was a single-center study with regulated use of OCT resulting in a low sample size. Secondly, it was not compared with other imaging modality like IVUS. Multi-center randomised controlled trials are needed to define the superiority of OCT over angiography-alone PCI and comparison of different light-based modalities is needed to compare results of stent optimisation after PCI.
Conclusion
The resolution of OCT provides a histology-grade definition of coronary plaque and it allows for a better understanding of coronary artery disease as well as the stent microstructures. It provides a promising new technology for intra-coronary imaging because of its high resolution and broad dynamic range. OCT guided PCI is superior to angiography-alone guided PCI because of the optimisation techniques which can be assessed during and after stent placement.
Highlights
This study suggested that various coronary clinical scenarios can be visualised in terms of plague morphology using the OCT After percutaneous coronary interventions with OCT, majority of the stented lesions require a re-intervention like stent optimisation or an additional stent due to mal-apposed struts or edge dissections Overall safety of the coronary intervention is increased with intravascular imaging modality and OCT should be sparingly used as an adjunct to percutaneous coronary interventions
Footnotes
Authors’ contributions
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.