
Abstract
Background and aims
In 2010, a virtual sarcoma referral model was implemented, which aims to provide a centralised multidisciplinary team (MDT) to provide rapid advice, avoiding unnecessary appointments and providing a streamlined service. The aim of this study is to examine the feasibility of this screening tool in reducing the service burden and expediting patient journey.
Methods and results
All referrals made to a single tertiary referral sarcoma unit from January 2010 to December 2018 were extracted from a prospective database. Only 26.0% events discussed required review directly. 30.3% were discharged back to referrer. 16.5% required further investigations. 22.5% required a biopsy prior to review. There was a reduction in the rate of patients reviewed at the sarcoma clinic, and a higher discharge rate from the MDT in 2018 versus 2010 (p < 0.001). This gives a potential cost saving of 670,700 GBP over the 9 year period.
Conclusion
An MDT meeting which triages referrals is cost-effective at reducing unnecessary referrals. This can limit unnecessary exposure of patients who may have an underlying diagnosis of cancer to a high-risk environment, and reduces burden on services as it copes with increasing demands during the COVID-19 pandemic.
Introduction
Early diagnosis and treatment by appropriate specialists is the cornerstone of sarcoma management, and delay or inappropriate intervention can have significant ramifications to patient morbidity and mortality.1,2 In recent years it has become widely accepted that investigations and management of soft tissue and osseous tumours should be performed in conjunction with specialist sarcoma centres. 3 , 4 Guidance provided by the National Institute of Health and Clinical Excellence (NICE) states that all patients with a confirmed bone or soft tissue sarcoma should have their care supervised or in conjunction with a sarcoma multidisciplinary team (MDT). 5 Furthermore, the Scottish Government designated cancer care as one of the key targets for Health care. This standard requires 95% of all patients’ diagnosed with cancer begin treatment within 31 days of a decision to treat, and 95% of those referred urgently with a suspicion of cancer to begin treatment within 62 days of receipt of referral. 6 This is often more difficult in sarcoma due to the non-specific nature of their clinical features and the relative rarity of these cancers, and has led to increasing demand on these services given the high ratio of benign to malignant lesions (reportedly as high as 100:1) and the high incidence of suspected sarcoma compared to the relatively low incidence of actual sarcoma. 7
Historically Scotland’s geography and demographics meant suspected soft tissue and osseous tumours were often referred for investigation by primary or secondary care practitioners prior to tertiary referral. This may have led to potential diagnostic delay, unnecessary invasive investigations and/or surgical intervention without prior biopsy, factors well recognised to be associated with delay in diagnosis and poorer patient outcome. Furthermore, of those patients referred to the tertiary centre, a significant number would be required to travel long distances for multiple outpatient consultations.
Specific to the West of Scotland sarcoma service, our catchment area covers around half of the population of Scotland (around 2.8 million) and a geographic area covering approximately 40 thousand square kilometres. In 2010, due to increasing demand on the West of Scotland Musculoskeletal oncology service, a virtual referral model was designed and implemented. This aims to utilise modern electronic technology and a centralised multidisciplinary team to provide rapid advice and diagnosis for efficient patient care, avoiding unnecessary clinic appointments and providing a streamlined service to optimise timely investigations for those patients. The service accepts referrals for adult patients by letter, or more commonly by e-mail to the Musculoskeletal oncology team. At present this service does not cover paediatric referrals (under 16 years of age). E-mails are monitored daily by the lead clinicians and a Musculoskeletal clinical nurse specialist. Immediate advice can be given with regards to baseline imaging as required, including x-rays, CT, MRI, NM bone scan and blood tests. Patients are discussed at a weekly Musculoskeletal Radiology meeting. To allow patients to be discussed at this meeting effectively, referrers are expected to provide key information: patient demographics, referrer’s contact details, comprehensive clinical history and up-to-date imaging. Patients referred without the possibility of timely investigation are appointed on an urgent basis to the next clinic to avoid any delay in making a diagnosis.
The Musculoskeletal Radiology Meeting runs with key personnel comprising at least one consultant orthopaedic surgical oncologist, Musculoskeletal consultant radiologist and the orthopaedic oncology clinical nurse specialist. Patient’s referrals are discussed with emphasis on the radiological investigations and any available relevant laboratory results. Patient imaging is available on the Scotland wide digital national archiving system which allows access to all digital imagery from all NHS radiology departments across the country.
The aim of this study is to examine the feasibility of this screening tool in reducing the burden on our service, facilitating investigations and expediting the patient journey.
Methods
All referrals made to a single tertiary referral sarcoma unit are entered into a prospectively maintained database. This database was used to extract data on all referrals from January 2010 at its inception to December 2018. New referrals to the sarcoma team are discussed at the Musculoskeletal MDT conference, as well as follow up investigations to determine if the patient requires a sarcoma unit review. The outcomes of each discussion were then grouped into 6 categories. The patient was either reviewed at the sarcoma unit clinic, discharged directly from the conference to local referring team, required further investigations locally, required a biopsy prior to review, referred for discussion at the National Sarcoma Multi-disciplinary meeting prior to review to formulate a management plan, or the aim of the discussion was for review of imaging for pre-operative planning. Demographics of referrals, outcome of review and yearly data variances were analysed to determine the effectiveness of the conference discussion, and a cost analysis was carried out to determine the potential cost savings of establishing this system.
Statistics
Data are presented as Total (Percentage) unless otherwise specified. Comparison of outcomes between years were performed using the Pearson’s Chi-Squared test (χ2). Analysis was performed using SPSS software (SPSS for Windows Version 26.0, SPSS Inc., Chicago, IL, USA). Statistical significance was deemed as a p value < 0.05.
Results
Our centre serves a geographical area of approximately 40,000 km2 and a population of 2.8 million. The database contained 5,714 Events for 3,976 Patients, giving an average of 1.44 discussions per patient. 1,710 (41.7%) of Patients were from out-with our local hospital trust (NHS Greater Glasgow and Clyde). 2,116 (51.6%) of patients are Male. Events had a missing Conference outcome in 280 (4.9%) patients, and these were excluded from the analysis. There was a consistent increase in referral volume from 2010 to 2015, which plateaued thereafter. Table 1 and Figure 1 demonstrates the demographics of the database.
Demographics of events in database by year.

Note: 2010 represents the First year of inception and so all referrals are deemed new patients that year.
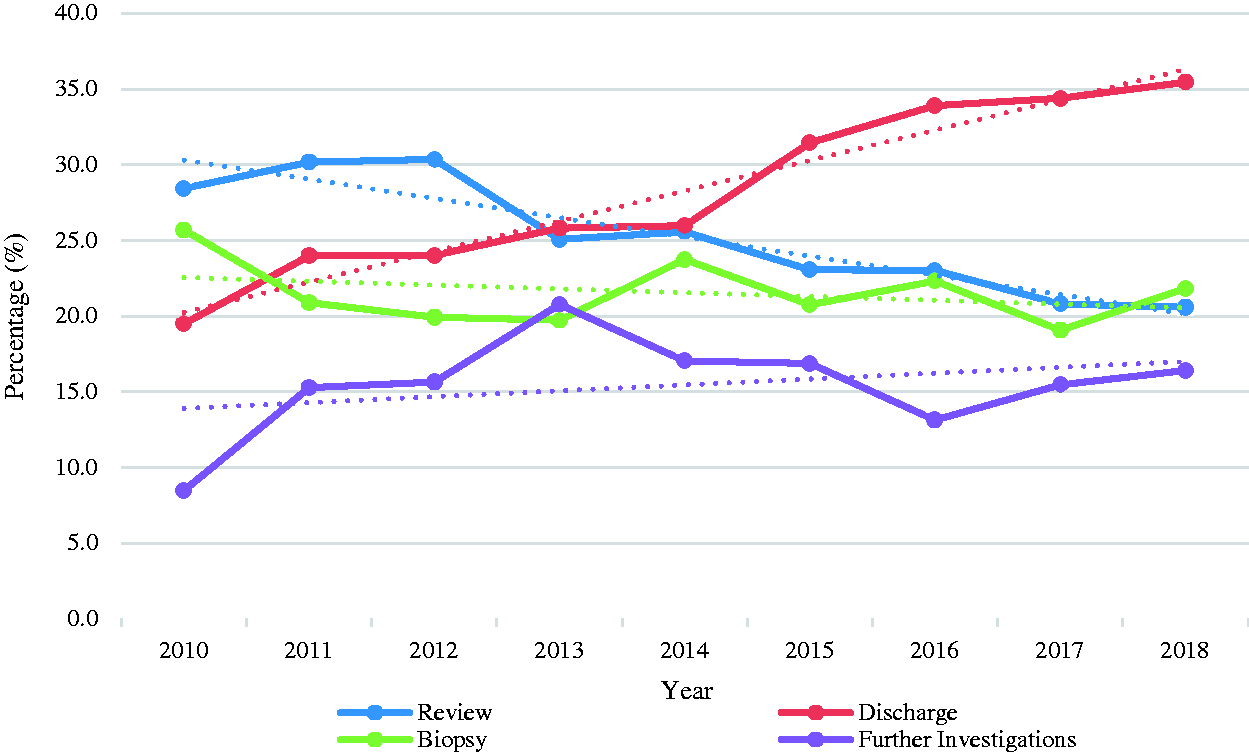
Trends in Outcome of discussions over time, from 2010 to 2018.
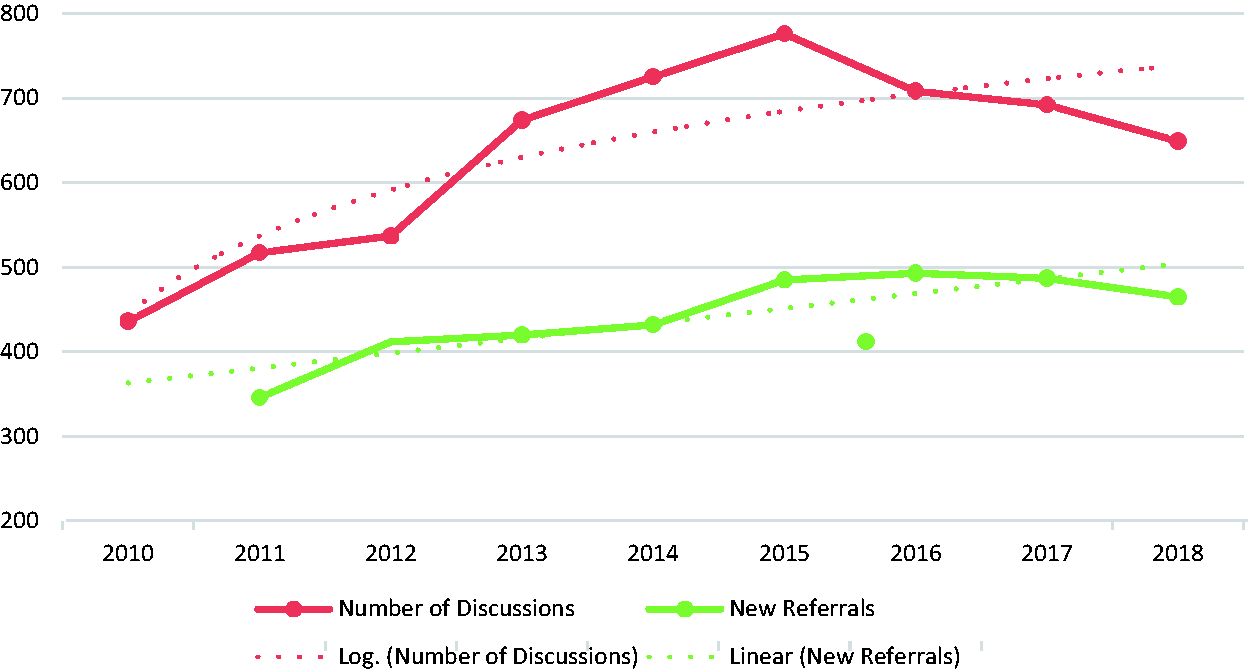
Trends in the number of discussions and number of new referrals over time, from 2010 to 2018.
Table 2 illustrates the percentage of cumulative outcomes of the Musculoskeletal MDT conference discussions by year for the 9 year period studied. Overall, following discussion at the conference, only 1,414 (26.0%) events discussed required review directly from the Conference. 1,649 (30.3%) events were discharged from the sarcoma unit back to the referring clinician. 899 (16.5%) events required further investigations and imaging. 1,222 (22.5%) events required a biopsy prior to clinic review and 104 (1.9%) events were referred for discussion at the National Sarcoma MDT meeting prior to reviewing patient. 146 (2.7%) events were discussed for surgical planning.
Outcome of conference discussion by year.
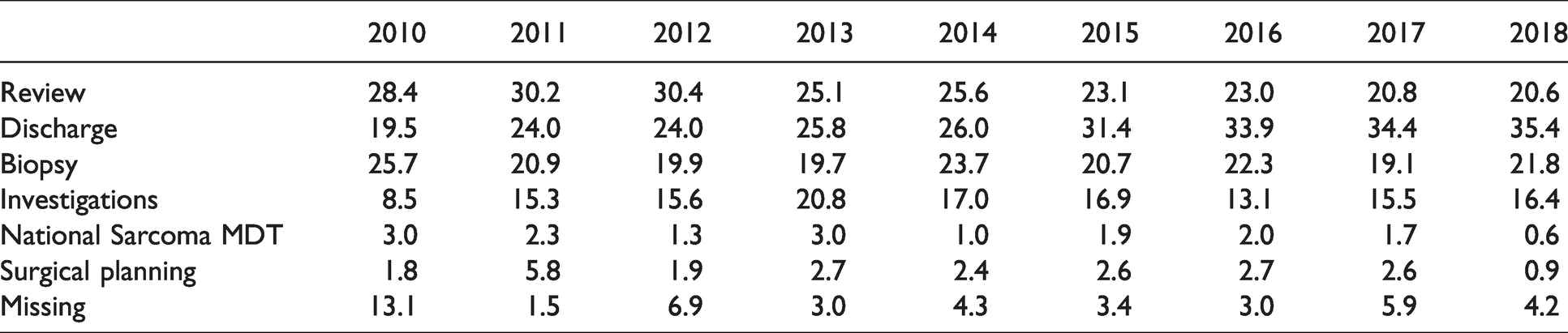
Figure 1 and Table 2 illustrates the changing outcome demographics per Year. Despite the increased volume of referrals (Figure 2), we noted a statistically significant reduction in the rate of patients reviewed at the Sarcoma clinic, and a higher discharge rate from the Musculoskeletal MDT conference in 2018 in comparison with 2010, with a p value of <0.001. Comparing variations in outcomes between years, there are statistically significant year-on-year variations between 2010 to 2014 (p < 0.05), and thereafter the variations become non-statistically significant.
Excluding discussions for surgical planning and referrals to the National Sarcoma MDT, and at a saving of 1 clinic appointment per virtual consultation, we estimate 3,956 clinic appointments were saved over the time period. Based on published national statistics from the Information and Statistics Division Scotland, the average cost of an orthopaedic clinical consult within our unit was 169.54 GBP. 8 This gives a potential cost saving of 6,70,700 GBP over the 9 year period, and an average cost saving of 74,522 GBP per annum without adjusting for inflation costs.
Local analysis carried out by Kosomnuk, University of Strathclyde 2014, looked at the relevant societal and patient costs per appointment at the Orthopaedic Oncology clinic at our Unit. This used an economic analysis as well as questionnaires to patients attending clinic to investigate the minimum cost per patient considering time and distance patients travelled, direct and out-of-pocket expenses and opportune costs secondary to accompanying adult. Based on this analysis and using the weighted average, the minimum saving per patient visit is 33.65 GBP. Therefore, the minimum societal saving over the 9 year period is 1,33,119 GBP, which equates to 14,791 GBP per annum.
Discussion
A multi-disciplinary meeting which triages referrals utilising local clinical assessment, local imaging and review of the above information at a combined surgical and radiological conference is a cost-effective method of reducing unnecessary referrals.
We noted a significant year-on-year increase in the initial volume of referrals from inception of this system, with a 48.9% increase in the number of discussions from 2010 to 2018. We hypothesize that the reasons for this are multi-factorial, and likely relate to an increased awareness of the system, which provides referring clinicians with quick, reliable advice on complex oncological imaging findings and further guides further investigation and treatment. Finally, the increasing medico-legal nature of medicine, and fear of missing an Oncological diagnosis by clinicians, drives earlier referral and discussion with the MDT. Re-discussions of existing patients accounts for only a small number of this gradual increase in Events, and Table 1 shows that the rate of New Referrals as a proportion of discussions shows an increasing trend which supports this. Despite the increase in the number of discussions and referrals, the proportion of patients requiring review decreased, and the number of patients discharged from the Conference increased. This is an interesting trend, which likely reflects the reduced threshold to refer more benign lesions to ensure that the correct management is followed, and the increased experience and confidence of the MDT in diagnosing and discharging patients to the local referring team. More recently, the rate of increase has plateaued, and we hypothesize that this is a result of restrictions placed on the number of patients discussed per session due to time limitations.
Most strikingly, only 26% of referrals required a direct review. In a traditional referral system where the remaining 74% of patients were unnecessarily reviewed, it is likely that this would manifest in over-booked clinics and shorter consultations per patient in order to sustain that workload burden. In addition, patients would have faced delayed appointment time to be seen by the Sarcoma Unit given the finite clinic availability. Both factors could impact on the 26% that required review and further management by the Sarcoma team in a timely manner. Finally, it is likely that investigations would have to be either carried out within our tertiary Unit, placing an unsustainable burden on our Radiology department, or a delay in initiating investigations if the local referring Unit is required to carry out investigations after the patient has been seen by the Sarcoma Unit and appropriate investigations suggested. These delays can potentially result in poorer patient outcomes or a negative patient experience and can be extremely anxiety provoking in patients who demand a streamlined, quick and effective management plan. The meeting also provides an opportunity for sub-specialist radiology review of the available imaging, who benefit from the increased clinical information provided to re-interpret the imaging and clarifying the local radiology reports, and helping guide further investigations if required.
There is clearly a cost saving to the National Health Service with this system. While there are costs associated with the implementation of the Multi-disciplinary meeting which predominantly takes the form of Programmed Activity planning for the clinicians involved, this cost is difficult to estimate and likely is significantly overshadowed by the clinic visits saved. While the cost saving is intangible, the sequalae of a traditional referral system with increasing volume of referrals would have required an increase in clinic availability and direct recruitment of increased staff to cope with that volume of work.
In these unprecedented times of COVID-19, surgical oncologists are being forced to consider triage and rationing of cancer surgery cases, in an effort to mitigate potential shortages personal protective equipment, hospital personnel, and the desire to maximize social distancing amongst patients, colleagues, and staff. 9 However, this poses a challenge for the management of sarcoma and other high risk cancer types, in which a delay to management can result in adverse patient outcomes. 9 , 10 Recently, NICE has issued a clinical guideline for the delivery of anticancer treatments to cancer patients with COVID-19. The NICE guideline provides many recommendations based on the currently available evidence regarding many COVID-19-related and cancer related issues, and recommends minimising face-to-face contact and using local services for investigations if possible. 11 Several expert opinion papers and guidelines have advocated a similar approach specifically for the management of sarcoma, but the evidence to support this is lacking. 12 , 13 To the best of our knowledge, this is the first paper that provides evidence that such a meeting can potentially limit unnecessary exposure of patients who may have a new underlying diagnosis of cancer to a high-risk environment, and reduces the burden on the service as it copes with increasing demands. In addition, the COVID-19 pandemic has resulted in changes in financial reimbursement in pay-per-service health care systems, such as those in North America, which acknowledge and incorporate virtual consultations into the existing health care structure. 14
Our service covers a wide geographic area given the relatively low density population of the West of Scotland in comparison with the remainder of the United Kingdom. Although only 42% of our referrals are from out with our trust, NHS Greater Glasgow and Clyde represents the largest health board in Scotland, and one of the largest in the United Kingdom. Therefore, there is significant transport costs and journey time for patients both within and out with this trust. Typically, the patient population referred to a Sarcoma Unit is of a working age, and so this has implications for employment and sick leave requirements. Therefore, the societal costs can be significant, and given only a small proportion of patients required an initial consultation, this system provides patients with convenience of local hospital follow-up, prevents unnecessary patient journeys and the associated inconvenience and costs.
For the 22.5% of patients that required an image-guided biopsy prior to review, the meeting provides an opportunity for the surgeon and radiologist to agree on a biopsy tract that is appropriate and safe, thereby potentially minimising adverse patient outcomes. 15 This can then be saved to the national Picture Archiving and Communication System (PACS) for future reference at time of biopsy. By doing so, no patients had an inappropriate biopsy tract. Finally, the meeting has clear educational value to trainees in all the involved disciplines and allows a forum for complex requests to be discussed and the development of a close working relationship between the specialities involved.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.