
Abstract
Introduction
Near-peer assisted learning (NPAL) has been welcomed in recent years as a favourable method for teaching medical students. It has proven advantages for both the educator and the learner. As such it was identified as an ideal approach for delivering the local curriculum within a paediatric surgical setting. Short duration of placements further suggests that structured tutorials would best guarantee coverage of the student curriculum. Our hypothesis was that the introduction of a structured programme such as this could lead to reduced dependence on senior staff for teaching, increased exposure of junior staff as educators, and increased coverage of the curriculum.
Methods
Curriculum outcomes were identified, and a series of tutorials developed for delivery by juniors within the department. Pre and post intervention questionnaires were given to students rotating through the department.
Results
70 responses were analysed (23 pre; 47 post intervention). Reliance on Consultant teaching dropped 29% and engagement of surgical, GP and foundation trainees in teaching increased by 29%, 43% and 9% respectively. Overall curriculum coverage increased by 12%.
Conclusion
A near-peer assisted tutorial programme is an effective way of increasing coverage of the medical curriculum with benefits for tutors and learners, whilst increasing junior engagement in teaching and reducing burden on Consultants.
Introduction
Near-peer assisted learning (NPAL) is a pedagogical approach which has grown in popularity within the field of medical education.1,2 Defined as teaching provided by one trainee - of one or more years senior - to another trainee 3 it benefits from not requiring utilisation of scarce expert instructors,4,5 and with advantages for both students and teachers. 6
Students profit in many ways. Studies in nursing education have shown improved outcomes in examination scores7,8 associated with NPAL. There are also psychological benefits, with students experiencing less distress attributed to fear of ridicule or lack of appreciation that can be associated with expert tutors.3,9 Reasons for this stem from the theory of “cognitive congruence” 10 where proximity of age leads to more recognisable language 11 and the ability to put a learner at their ease more readily. 12
Advantages to tutors may be even greater. 13 A number of studies show increases in teacher knowledge development in excess of learners14–17 and prepares junior trainees/senior medical students for a future role as a trainer and educator. 18 Indeed, in one study, 91% of participants in NPAL said being a tutor made them want to pursue teaching as part of their future career. 19 The positive effects are reinforced by repeat delivery of material to address uncertainties and improve understanding of concepts.20,21
Consideration of a NPAL approach to teaching students became relevant to our department when concern emerged around a lack of learning for both students and junior doctors in relation to the field of paediatric surgery: students because of the random nature of patient presentations and limited time spent in the department and junior doctors, because of the restrictions placed on them by a high administrative burden. In addition, the UK foundation curriculum includes “developing the clinical teacher”: as such, an opportunity to improve learning for both parties were identified.
We aimed to develop a NPAL programme that would improve core curriculum coverage for medical students, reduce dependence on senior staff for teaching whilst increasing junior staff exposure and, indirectly, tutor knowledge gain.
There is a scarcity of evidence in the literature focussed on how curriculum coverage and workload distribution can be affected by NPAL programmes and our study aims to address this.
Setting
The paediatric surgical department at the Royal Aberdeen Children’s Hospital, Scotland, is a tertiary referral centre. Staffing consists of four permanent Consultant paediatric surgeons and one specialty doctor, two core surgical trainees, one general practice trainee (GPST) and four foundation year one trainees. In addition, a clinical development fellow (CDF) may be attached to the unit – this is a non-training single year surgical post which allows twelve hours per week for development in an extra-clinical field, be it research, quality improvement or medical education.
The hospital is affiliated with the University of Aberdeen and is actively involved in teaching and training across the whole undergraduate curriculum. Students are first introduced to paediatric surgery in their third year, during a series of lectures, however their main exposure takes place in their fourth year when they spend a whole week on the unit. This forms part of their child health block along with medical paediatrics and neonatology. Students may also be offered a 6-week placement within the department in their final year as their mandatory surgical attachment. Traditionally the teaching program on the unit was Consultant led and delivered. It became apparent that delivery of undergraduate teaching was potentially inconsistent owing to the availability of Consultants due to clinical commitments, study leave and annual leave. In addition, the content of ward, clinic and theatre-based learning was very dependent upon the differing nature of presenting patients. Concurrently it was noted that junior doctors having passed through the department had an apparent lack of knowledge of core paediatric topics. The foundation curriculum includes ‘developing the clinical teacher’ however opportunities to develop requisite skills can be few and far between. A decision was made within the department to address both the issue of standardising undergraduate teaching and improving the knowledge of junior doctors through the implementation of a nee-peer teaching program.
Methods
The fourth-year undergraduate curriculum was reviewed and the learning outcomes that were associated with paediatric surgery were condensed into thirteen tutorials. Standardised learning materials were collated for each topic consisting of an annotated tutorial, clinical images and in some cases a power-point presentation. The existing student handbook was redesigned to include the new teaching program and outlined how it would be delivered.
At the end of the week, students sit a formative assessment consisting of multiple-choice questions covering all the core topics. They are also invited to complete a feedback form to determine: the grade(s) of doctor responsible for delivering their teaching; which topics were covered and in what format they were delivered; and a free-text box where they can suggest ways to improve the program.
Results
A pre-intervention group – covering the period February to August 2017 - and a post-intervention group – covering the period May to July 2018 - were analysed. The second data set collected (May to July 2018) followed full implementation of the neer-peer tutorial program. Data was entered into a spreadsheet and Fisher exact test performed to look for significance, defined as 2 tailed p value less than 0.05.
Overall there were 70 feedback forms returned: 23 in the pre-intervention group and 47 in the post-intervention group. All forms were included in the study – 2 forms in the post intervention group had incomplete data pertaining to grade of tutor, and so were excluded for this analysis but included in the curriculum coverage figures.
Regarding grade of tutor, the results suggest a move towards NPAL, with the proportion of students who attributed teaching to consultants dropping from 100 to 71% and staff grade from 39 to 13%. Conversely, the teaching attributed to surgical trainees rose from 22 to 51%; CDF 9 to 93%; GPST 4 to 43%; and senior students 0 to 17% (Table 1). There was an increase in FY1 delivered teaching from 48 to 56%.
Summary of data comparing major tutor grades identified by students during placement.

P values removed.
With respect to the curriculum coverage, there was overall a significant increase in curriculum coverage from 78 to 90%. Looking at individual topics, there was an improvement in coverage of the acute scrotum – from 52 to 96% – and pyloric stenosis – from 65 to 91%. The full results are expressed below (Figure 1).
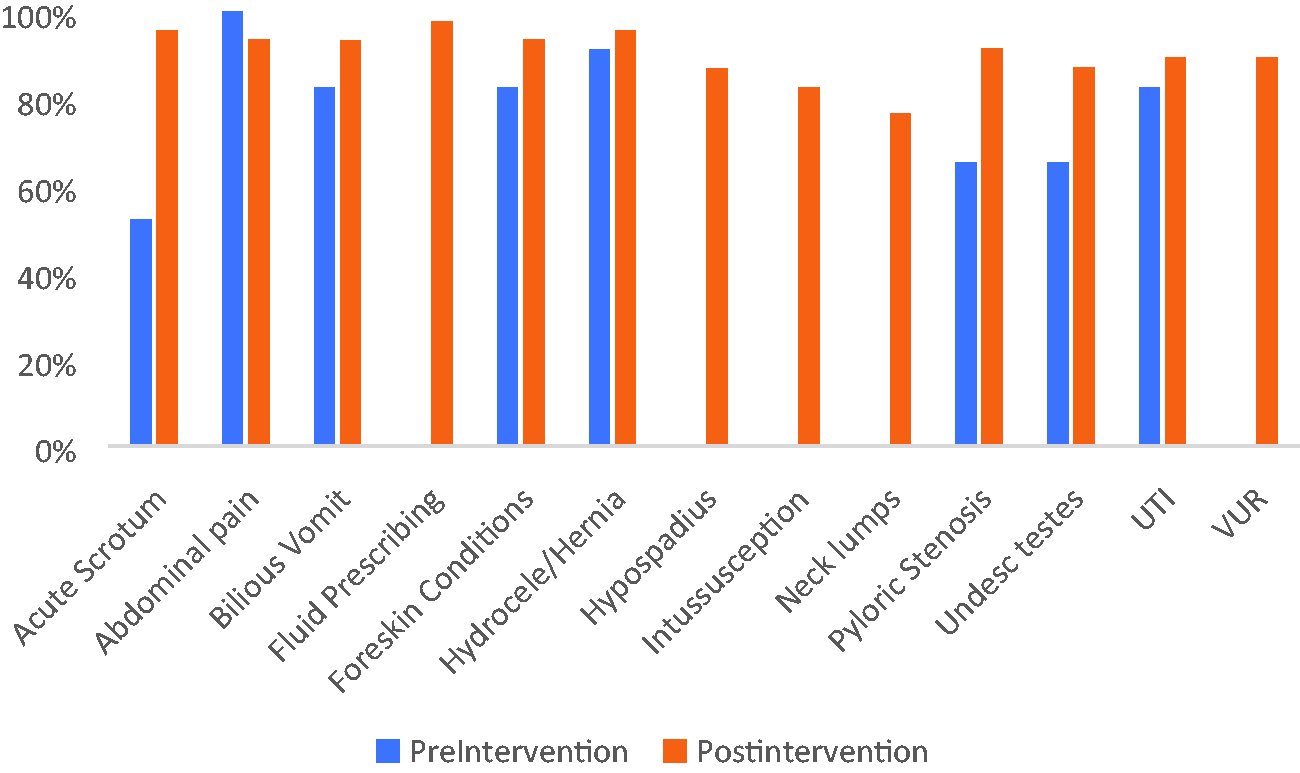
Graph representation of curriculum coverage.
There was a general increase in most of the other curriculum outcomes. On the other hand, coverage of the acute abdomen topic had a slight fall.
Discussion
Multiple, short and intensive, ward-based placements form the mainstay of the current fourth year medical school program designed to place theoretical learning into context. Whilst the curriculum consists of clear learning outcomes it is up to each department to decide which ones are relevant to their specialty and how best to deliver any teaching. Traditionally, education has been a direct responsibility of the available Consultant team. However, as previously highlighted, this ad-hoc delivery can potentially lead to issues with curriculum coverage. The reduction of junior doctors’ hours and change of working patterns has resulted in foundation year doctors spending a lot of time completing the paperwork associated with clerking and discharging patients. They are often unaware of the pathophysiology of the conditions that they are seeing as this is not required in their day-to-day functioning. Furthermore, there is a strong emphasis on “developing the clinical educator” in postgraduate curricula however it is an area that can sometimes be neglected in favour of clinical tasks.
The idea of our teaching program was to ensure that all students rotating through the department received equal educational opportunities. Teaching materials were provided not only to standardise tutorials but also to ensure that less confident tutors felt empowered to deliver the subject matter. Information was made available in a variety of formats in order to allow some fluidity in delivery.
The results above are encouraging. We showed a reduction in the reliance on Consultant led ward-based teaching and an uptake in junior teaching. It is noticeable that the presence of a CDF, who during the study period had an interest in education and was noted as responsible for teaching delivery by almost all the students while attached to the unit, may have contributed to the high coverage of the curriculum. However, following the CDFs departure, other grades appeared to increase their relative contributions.
The coverage of the curriculum during students’ placement seemed to improve as a result of the NPAL tutorial programme. Unfortunately, there were only eight out of the thirteen outcomes in the pre-intervention group measured, as prior to liaison with the university to identify those outcomes deemed important to cover, only those areas most often taught were analysed. However, given that those areas were likely to see limited coverage prior to implementation of the NPAL tutorials, it could be assumed that these too saw a significant improvement in their concordance.
Although we saw a significant increase in the tutoring by all other junior grades, it was disappointing to not achieve a higher increase in foundation doctor participation, given that this was the grade deemed to have most to gain from the programme. Barriers to this seem to be low confidence regarding their ability to teach unfamiliar content, difficulty balancing workload, and potential lack of engagement from students, who are sometimes unwilling to wait for foundation doctors to become free before seeking alternative educational opportunities. Future avenues to improve this could include portfolio incentivisation with certificate recognition, induction coverage of the topics to improve confidence, and pre-arranged tutorial times when senior colleagues can be around to help with the workload. There certainly seems to be paucity of study on this subject, which is particularly concerning given the attention the foundation curriculum gives to developing the clinical teacher. Some deaneries have developed educational consortia, such as the South East Faculty of Clinical Education 22 in Scotland, to provide workshops and development programmes supporting acquisition of teaching skills in junior doctors. Such a system may be an invaluable addition in the North East of Scotland for breaking down these barriers to foundation doctors taking part in teaching activities.
The impact of educational intervention is most popularly related to the Kirkpatrick framework for training evaluation. This divides training outcomes into four levels: level one is termed “reaction”, or the learners response to an intervention; level two is “learning”, where there is evidence of retention of knowledge; level three is “behaviour”, where there is evidence of impact on the practical application of knowledge gained; and level four is results, or improvement within the organisation itself. 23 The intervention described in this paper only achieves a Kirkpatrick level one outcome. Further study could utilise the end-of-week assessment to evidence a higher impact level but unfortunately test scores for the pre-intervention group were not available during this study period.
There were other limitations to this study. The heterogeneity of the data between the two groups makes direct comparison difficult. In addition, changes within the department particularly in terms of staff who may have more time, or more interest in teaching, may confound the results. Furthermore, the small sample size particularly in the preintervention group could lead to type 1 errors.
Conclusion
We present a novel example of a quality improvement project, centred around a formalised near-peer assisted learning programme, which succeeds in increasing curriculum coverage for students and exposure of junior staff to teaching, with an aim of improving knowledge acquisition for both groups. Further improvements would relate to increasing foundation doctor engagement and additional data collection looking at assessing the knowledge gain in both students and staff consequent to their involvement with the programme.
Footnotes
Acknowledgements
The authors would like to thank supporting consultants and junior medical staff working within the department of paediatric surgery during the study period, particularly those who delivered tutorials. Thanks also to administration staff of the University of Aberdeen for organising student placements and supporting our work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.