Prescribing of SGLT2 inhibitors in secondary care: Progress and barriers
Samuel Birch-Machin, Catherine Russell, Jennifer Lees, Jack Fairweather, Emily McQuarrie, Patrick Mark, Keith Gillis
Queen Elizabeth University Hospital, Glasgow
Intro: Sodium/glucose cotransporter-2 inhibitors (SGLT2i) reduce risk of progressive kidney disease both in and out with the setting of diabetes. The aims of this study were to quantify the current uptake of canagliflozin within patients with type 2 diabetes in nephrology units within the west of Scotland and to identify barriers to prescribing.
Methods: A retrospective analysis of the Scottish Electronic Renal Patient Record (SERPR) was performed to patients to secondary care nephrology services within NHS Greater Glasgow and Clyde (GGC) and NHS Lanarkshire who were eligible for SGLT2i. Canagliflozin is licensed for treatment of diabetic kidney disease (DKD) in patients with type 2 diabetes, estimated glomerular filtration rate (eGFR) >30 ml/min/1.73 m2, urinary albumin:creatinine ratio (uACR) >30 mg/mmol. A questionnaire was produced to identify attitudes towards prescribing SGLT2i’s. The survey was composed of 5 questions on GoogleForms and Survey Monkey platforms. These were disseminated via email to prescribers in NHS GGC (nephrology only) and NHS Lanarkshire (nephrology and medical specialties).
Results: From the retrospective SERPR analysis, there were 74 patients in NHS Lanarkshire identified as eligible, of whom 8 (11%) had been prescribed canagliflozin. In NHS GGC, 148 patients were identified as eligible of whom 57 (38.5%) had been prescribed canagliflozin. There were 58 survey responses gathered in NHS Lanarkshire and 18 responses from NHS GGC. Within NHS Lanarkshire 35.5% of respondents were consultants, 19.0% were registrars, and 34.5% were foundation or core trainee doctors. Respondents in NHS Lanarkshire felt that the main responsibility for prescribing SGLT2i lay with diabetes (55.1%), then all specialties equally (39.7%), GP (20.7%) and cardiology (17.2%). Only 24.1% of respondents in NHS Lanarkshire had started a patient on an SGLT2i and 29.3% felt they had access to adequate information to commence a patient on SGLT2i. Within NHS GGC, 72.2% of respondents were consultants and 11.1% were registrars, 83.3% had prescribed SGTL2i and 94.4% of respondents felt as though they had adequate information to commence patients of SGLT2i treatment. Within NHS GGC 61.1% of respondents felt every specialty had equal responsibility to start patients on SGLT2i, followed by diabetes (33.3%), nephrology (33.3%) and GP (27.8%).
Conclusion: SGLT2i prescribing in patients with DKD remains low. A variety of factors contribute towards this, including inadequate provision of information to clinicians regarding commencing SGLT2i, concerns over serious side effects of SGLT2i (such as euglycemic DKA) and disagreement over whose responsibility it should be to commence these medications. Providing further education and readily accessible prescribing resources to clinicians, and particularly to training grade doctors, may help to increase uptake of SGLT2i.
Has lowering the initial dose of mycophenolate mofetil in transplant recipients over the age of 60 impacted on clinical outcomes?
Emma Cannon1, Trijntje Rennie1, Paul Phelan1
1Department of Renal Medicine, The Royal Infirmary of Edinburgh.
Background: Previous work looking at the Scottish transplant population highlighted that 77% of patients over the age of 60 failed to tolerate full dose (1 gram twice daily) of Mycophenolate Mofetil (MMF) following kidney transplantation.1 Since September 2018, patients over the age of 60 undergoing kidney transplantation in Scotland have been commenced on a lower dose of 500 milligrams (mg) twice daily of MMF. We aim to analyse the impact of this reduced immunosuppression regimen on the incidence of severe infection and acute rejection (AR) within the first year post transplantation.
Methods: Patients transplanted in The Royal Infirmary of Edinburgh between 01/09/2018 and 10/07/2020 were identified. Outcome data of patients over the age of 60 who were followed up in NHS Lothian were collected using the VitalData and TrakCare systems. All patients received standard immunosuppression at induction (basilixumab, MMF and tacrolimus). Serious infection was defined as any infection requiring hospitalisation or any opportunistic post-transplant infection necessitating immunosuppression reduction (BK, CMV and Pneumocystis Jirovecci infection). AR was defined as either biopsy proven rejection or empirically treated rejection. MMF intolerance was defined as requiring MMF dose reduction, cessation or change of antimetabolite. Statistical analysis was carried out on Microsoft Excel.
Results: During the follow up period, 206 kidney only transplants took place with 71 (34%) of recipients over the age of 60. Of the patients over 60, 23 (n = 15 male) were followed up in NHS Lothian. There were 3 deaths in the first year post transplant among these 23 patients (13%) (Infection n = 2, haemorrhage n = 1). The remaining 20 patients had functioning grafts at one year post transplant (mean eGFR 58.3 mL/min/1.73 m2). MMF Tolerance: Of the 22 patients commenced on the lower protocol dose of MMF, 8 (36%) failed to tolerate this, compared to 77% of patients on the prior protocol.1 One patient received a higher dose of 1 gram twice daily of MMF based on clinician preference. Reasons for MMF intolerance were gastrointestinal upset [n = 4 (18%)], leucopenia [n = 2 (9%)] and severe infection [n = 4 (18%)]. Some patients experienced more than one side effect. AR: Three episodes of biopsy proven acute cellular rejection affected 2 (8.7%) patients. One patient developed rejection whilst taking 500 mg twice daily of MMF. The other developed rejection when their MMF dose was reduced to 250 mg twice daily because of BK viraemia. There were no empirically treated episodes of rejection. Infection: Nine (39%) patients developed 24 severe infections within the first year post transplant. [BK viraemia - [n = 5 (22%)], CMV viraemia - [n = 2 (9%)] and 17 episodes of severe infection requiring hospitalisation affecting 5 patients (22%)]. In addition, there were 20 episodes of culture positive UTI (not requiring admission) affecting 8 (35%) recipients.
Discussion: Prior to the change in immunosuppression protocol 77% of transplant recipients over the age of 60 failed to tolerate 1 gram twice daily of MMF, 70% developed at least one serious infection and 11% experienced an episode of acute rejection during the first year post transplant1. These preliminary data from a limited number of patients suggest the reduction in the immunosuppression protocol in this age group is safe, with improved tolerance, an apparent very low AR rate as well as a lower infection rate. Mortality figures appear high. However, the three deaths reported were the only deaths in the larger cohort of 71 patients over 60. We plan to expand this work to examine outcomes of patients who are followed up across Scotland and to compare to younger cohorts to further assess the impact of this change in protocol.
≥60 on full-dose MPA vs 39% on reduced dose MPA
Reference
1.Rennie T.J.W., Petrie M., Metcalfe W., Walbaum D., Joss N., Barton E., Marson L., Clancy M.J., Henderson L., Traynor J.P., Geddes C.G. and Phelan P.J. (2020) The impact of age on patient tolerance of mycophenolate following kidney transplantation. Nephrology Vol. 25 Iss 7 July 2020 pp. 566–574 doi: https://doi.org/10.1111/nep.13718
Evaluating anticipatory care planning for patients who choose conservative kidney management
Dr C. Corson1, T. Sutherland1, Dr P. MacKenzie1
1University Hospital Crosshouse, NHS Ayrshire and Arran.
Objectives: At a busy teaching Hospital in Ayrshire, patients diagnosed with chronic kidney disease (CKD) who attend the renal advanced kidney care clinic (also referred to as the low clearance clinic) are provided education on different management options. This includes different types of renal replacement therapy and the option of conservative kidney management (CKM). Patients who are considering CKM are referred to the Renal Supportive Care Nurse for further education, advice and anticipatory care planning.
Our aim is to evaluate the demographics of patients choosing CKM and to study whether, by using renal anticipatory care plans (ACP), we are able to manage patients according to their wishes until end of life.
Methods: Using a database of patients who had chosen CKM, the demographics of the patients were analysed. Several categories were evaluated including gender, age, whether ACP was discussed, preferred place of care, place of death (when appropriate) and whether a ‘do not attempt resuscitation’ order was in place. The anticipatory care plans for patients who were deceased were then reviewed on the Scottish Electronic Renal Registry (SERPR) to compare their wishes, as pre-documented on ACP, with events at end of life.
Results: Overall 59 patients have chosen CKM, 25 identify as male and 34 female. Of these patients, 22 are alive and 37 are now deceased. Anticipatory care plans were completed in 18 patients, with 7 still in progress. 29 patients did not have an ACP, 3 patients declined and information was not able to be found for 2 patients therefore labelled as unknown. In the category of deceased patients the mean survival time from eGFR reaching <10 to death was 14.8 months. For the deceased patients, 10 out of the 11 patients that wanted to die at home did so, with one patient in the group dying in hospital.
Conclusion: This project provided the opportunity to learn more about patients choosing CKM and to evaluate whether patients who had anticipatory care planning were managed as per their wishes. So far, despite the limitation of small numbers, this project has found that the majority of the patients with ACP are dying in their preferred place of care. In the future, further study on a larger scale to evaluate if we are continuing to follow ACP in line with patient's wishes would be useful.
Improving the recognition, recording, management, and prevention of intradialytic hypotension in the Queen Elizabeth University Hospital outpatient haemodialysis unit
Kirsty Crowe1, Luis Loureiro Harrison1, Jamie Traynor1
1Glasgow Renal and Transplant Unit, Queen Elizabeth University Hospital, Glasgow
Background: Intradialytic hypotension (IDH) is a common haemodialysis (HD) complication which is associated with poor patient outcomes such as vascular access failure, end-organ damage, increased hospitalisation and increased mortality. We noted variability in the approach to management and documentation of episodes of IDH within the Queen Elizabeth University Hospital Renal Dialysis Unit (QEUH RDU). The existing unit protocol focussed on correcting hypovolaemia within the HD session without addressing other contributing factors to IDH.
Aims: This project aimed to improve the documentation of IDH episodes in the QEUH RDU and improve the adherence of IDH management to evidence-based guidelines, with the intention of reducing the incidence of episodes.
Method: We utilised quality improvement methodology with a number of plan-do-study-act (PDSA) cycles. Interventions included: introducing an event code to the electronic patient record to enable on-demand reporting of events and raise awareness to responsible clinicians; education through the renal unit departmental meeting; development of a revised IDH protocol in accordance with Renal Association guidelines; inclusion of IDH events in the QEUH RDU nursing safety huddles.
Outcome measures included a comparison of IDH events coded in the electronic patient record and paper HD records, number of admissions related to IDH events and the proportion of events where ultrafiltration was modified or intravenous fluid was administered. Process measures included number of patient medications, patients’ serum haemoglobin and albumin, and UF rates and targets for the relevant sessions. Regular dialogue with nursing staff was undertaken to identify the unintended impact of interventions and to inform further PDSA cycles.
Results: Electronic coding of IDH events poorly reflected paper documentation throughout the project despite the PDSA cycles. The greatest improvement was seen after the introduction of IDH event reporting in the QEUH RDU nursing safety brief, but this did not lead to sustained improvement.
The majority of IDH events were associated with appropriate nursing intervention, in line with the IDH protocol. Immediate changes in ultrafiltration occurred in 61.67% of all events and infusion of IV fluids occurred in 50.56% of all events. All cases coded on the electronic record resulted in the infusion of IV fluid, which may reflect a tendency to code the more severe end of the spectrum of IDH events i.e. those requiring fluid resuscitation. Concerningly the proportion of events where the UF rate exceeded the recommended 10 ml/kg/hour increased throughout the project despite the use of the revised protocol.
There was no sustained change in the incidence of IDH events, although the QEUH RDU incidence rate falls at the lower range quoted in wider literature.
Discussion: The documentation of IDH events on the electronic record reflects poorly on the true incidence of events in the QEUH RDU, and there has not been sustained improvement of this despite the interventions instituted. This results in a barrier to effective and efficient audit of IDH incidence. Given the overlap between electronic patient record coding and administration of IV fluid, a systematic intervention which prompts electronic event coding after delivering IV fluids may further improve documentation, along with the continued promotion of IDH as a safety issue amongst nursing and medical staff. The majority of IDH events led to appropriate nurse-led intervention, however there is scope to pursue better adherence to the protocol; the UF rate is a readily modifiable factor that can be leveraged to help prevent IDH events. Further iterations of the protocol will emphasise preventative measures which may have an impact on reducing the incidence of events.
The impact of fluconazole on tacrolimus levels in simultaneous pancreas-kidney transplantation
Bruce Dickson1, Trijntje Rennie1, Emma Cannon1, and Paul Phelan1
1Department of Renal Medicine, The Royal Infirmary of Edinburgh
Background: Simultaneous pancreas-kidney transplant (SPK) patients receive fluconazole as standard antifungal prophylaxis for the first week post-operatively or until clear donor duodenum swabs are demonstrated. Fluconazole inhibits CYP450 enzymes, which metabolise tacrolimus, and can result in increased tacrolimus exposure when co-administered. Despite this, the initial tacrolimus dosing regimen (0.05 mg/kg twice daily) is not altered for SPK transplantation. We wanted to investigate the impact of fluconazole on early tacrolimus levels in SPK patients compared to kidney only and simultaneous islet-kidney (SIK) patients.
Methods: All patients who underwent SPK and SIK transplantation, and all single kidney transplant recipients under 60 years old, from August 2018 - March 2021 were included. Patients over 60 years old were excluded as they receive different immunosuppression and are not comparable to the SPK/SIK population. Initial tacrolimus results were recorded, alongside the mean of the first three drug levels. Statistical analysis was carried out using Microsoft Excel. We used unpaired T test and considered a p-value of <0.05 to be statistically significant.
Results: 257 patients were included (see Table for demographics). SPK patients had a higher mean initial tacrolimus level (12.5ng/mL) compared to live (9.3ng/mL, p = 0.007), deceased donor (8.8ng/mL, p = 0.003) and SIK (8.6ng/ml, p = 0.051) recipients. Tacrolimus levels remain higher over the first three measurements in SPK recipients (11.2ng/mL) compared to live (7.9ng/mL, p = 0.00003) and deceased donor recipients (8.4ng/mL p = 0.0002) but not when compared to SIK (8.6ng/mL, p = 0.059), although note should be made of very small numbers in the SIK group. The number of initial tacrolimus levels ≥ 15ng/mL was higher in SPK patients (12, 28%), compared to SIK (0, 0%), live donor (8, 10%) and deceased donor kidney recipients (15, 12%). The number of initial tacrolimus levels ≤ 5ng/mL was lower in SPK recipients (3, 7%), compared to SIK (1, 14%), live donor (18, 22%) and deceased donor kidney (27, 21%).
Discussion: SPK recipients have higher levels of tacrolimus in the immediate post-operative period. This is likely to be related to concurrent fluconazole prophylaxis. Whilst high early tacrolimus levels may be deleterious, there may also be a benefit in higher initial levels post-operatively. The clinical significance of the differences we have demonstrated is unclear and further work is needed to examine allograft outcomes before any change in practice is planned.
Patient demographics and results.
SPK
SIK
Kidney Alone
Live Donor
Deceased Donor
N
43
7
81
126
Male (N, %)
56
71
54
56
Age at Tx (years), (mean ± SD)
42
50
42
45
Initial Tacrolimus Level (mean ± SD)
12.5 ± 7.5
8.6 ± 5.0
9.3 ± 4.8
8.8 ± 5.0
Initial 3 Tacrolimus Levels (mean ± SD)
11.2 ± 4.5
8.8 ± 3.3
7.9 ± 3.2
8.4 ± 3.3
Initial tacrolimus levels ≤ 5 (N, %)
3 (7%)
1 (14%)
18 (22%)
27 (21%)
Initial tacrolimus levels ≥15 (N, %)
12 (28%)
0 (0%)
8 (10%)
15 (12%)
Outcomes from a dedicated Tolvaptan clinic for patients with Autosomal Dominant Polycystic Kidney Disease (ADPKD)
1Glasgow Renal and Transplant Unit, Queen Elizabeth University Hospital, Glasgow
Introduction: Tolvaptan was approved for use in patients with ADPKD by the Scottish Medicines Consortium in January 2016, following the results of the TEMPO 3:4 trial, which showed that Tolvaptan reduced the rate of decline in kidney function- and increase in total kidney volume- compared to placebo.1 In July 2017, a dedicated Tolvaptan clinic was set up for patients with ADPKD from NHS Greater Glasgow and Clyde and NHS Forth Valley. Eligible patients are referred from their local general nephrology clinic, and counselled on treatment with Tolvaptan by a dedicated team comprised of consultant nephrologists, advanced nurse practitioners and renal pharmacists. Those who choose to proceed with treatment are reviewed monthly in the ADPKD clinic for the first 18 months of treatment before returning to three monthly follow up at their local nephrology clinic. We aimed to analyse the outcomes of patients referred to the ADPKD clinic since July 2017.
Method: All patients referred to the Glasgow ADPKD clinic between July 2017 and January 2021 were identified. Prospectively recorded data was collected from SERPR and Clinical Portal and analysed retrospectively. In those who did not commence treatment with Tolvaptan, the documented reason was recorded. In those who commenced Tolvaptan, further data were gathered including duration of treatment, dose achieved, side effects reported, any LFT derangement, and serum creatinine measurements over time. An assessment of whether patients met the Renal Association criteria for eligibility for treatment with Tolvaptan was also made.
Results: 78 patients who attended the ADPKD clinic were identified. 60 patients commenced treatment with Tolvaptan. Of those who did not start treatment, the most common reason recorded was anticipated side effects and consequent impact upon quality of life (7/18 patients). 25 of the 60 patients who started Tolvaptan stopped the drug during this period, after a median length of treatment of 11 months (IQR 2–18 months). The most common reason for stopping Tolvaptan was also side effects −23% of our patients stopped for this reason compared to 8% in the trial. The median length of treatment in those patients still on Tolvaptan was 21 months (IQR 14–34.5 months). 29 patients had a break in treatment due to the COVID-19 pandemic. 7 patients (11.7%) had treatment suspended due to deranged LFTs, and 2 (3.3%) of those patients did not resume Tolvaptan, compared to 1.2% of patients in the trial. In retrospect, 4 of the 60 patients commenced on treatment may not have met the criteria for eligibility for treatment with Tolvaptan suggested by the Renal Association.
Discussion: Tolvaptan appears to be well-tolerated in the majority of patients. As expected, a significant minority of patients do not tolerate Tolvaptan due to expected side effects. A higher proportion of our patients stopped Tolvaptan due to aquaresis side effects that in TEMPO, but this is not unexpected, and the vast majority of patients in our clinic elected to resume Tolvaptan after an enforced break due to the COVID-19 pandemic. Fewer patients in our clinic were maintained on less than full dose Tolvaptan when compared with the trial. A higher percentage of our patients had Tolvaptan discontinued due to deranged LFTs than in the trial, although this was only 2 patients. The impact of Tolvaptan on CKD progression outwith the trial setting will become clearer over time.
Reference
1.Torres V, Chapman A, Devuyst O, et al. Tolvaptan in Patients with Autosomal Dominant Polycystic Kidney Disease. N. Engl. J. Med 2012; 367(25): 2407–2418.
Have CORAL and ASTRAL Blocked Renal Stenting?
Edgar B, Pearson R, Kasthuri R, Gillis K, Brady A, Hussey K ,Roditi G, Delles C, Kingsmore
Background: The CORAL and ASTRAL trials found no benefit to renal artery stenting in addition to medical therapy in the groups studied. This has led to a perception that endovascular intervention overall offers limited benefit whilst conferring substantial risk.
Aim: To report the outcomes of a consecutive group of patients undergoing renal artery stenting, and determine whether greater benefit may be achieved in higher risk patient groups not included in trials.
Methods: Retrospective case note review of all patients undergoing percutaneous angioplasty and/or stenting of the renal artery between 2008 and 2021 (n = 94, 50 M 44F, mean age 60). Preoperative systolic blood pressure (sBP) and number of antihypertensive medications compared with that at time of discharge and at 6 months and/or 1 year. Major Renal and/or Cardiovascular Events recorded from time of intervention to end of follow up. Mean follow up 61 months.
Patients were compared against exclusion criteria from the CORAL trial, and against criteria from recent literature determining patients with high-risk RAS. Those presenting with Flash Pulmonary Oedema, sBP ≥ 200 despite ≥ 4 antihypertensives and/or AKI necessitating RRT were included in the High-Risk group.
Patients were grouped and results analysed separately according to indication, risk group and CORAL exclusion.
Results: Indications for intervention included Hypertension (n = 48), Acute and/or Chronic Renal Impairment (n = 27), Pulmonary Oedema (n = 40) and Transplant Renal Artery Stenosis (n = 20).
The average reduction in sBP and reduction in antihypertensives at time of discharge was higher in the High-Risk group than the Low-Risk group (44.1 mmHg vs 27.5 mmHg; 1.66 stopped vs 0.84 stopped). The same was true for reduction in the serum creatinine level at discharge and 6-month follow up (108 µmol/l vs 64 µmol/l; 135.6 µmol/l vs 76 µmol/l).
In those who would have been excluded from CORAL, an average reduction in sBP of 26.7 mmHg and of 1.3 in antihypertensive medications was observed. The average reduction in serum creatinine level was 172.3 µmol/l at discharge and 206.5 µmol/l at 6 months in this group.
When hypertension was the indication, there was an average reduction of 51.24 mmHg (25%) in sBP at discharge and 39.8 mmHg (19.5%) at 1 year.
In those with renal dysfunction as an indication, this was chronic in 63% and acute in 37%. Those with acute dysfunction had a larger reduction in serum creatinine both at discharge (294 µmol/l vs 125 µmol/l) and at 1 year (413 µmol/l vs 153.5 µmol/l) as well as a greater reduction in sBP (59 mmHg vs 32 mmHg) and more antihypertensives stopped (2.3 vs 1.3). 10 patients (6 chronic vs 4 acute kidney injury) who had commenced Haemodialysis regained function following intervention and ½ have not required further dialysis within the follow up period. The other ½ managed an average of 10.4 months of dialysis-free time.
Procedure-related major renal events, major cardiovascular events and mortality were similar between high and low-risk groups.
Conclusion: Limitations in previous trial design may have led to an underestimation of the clinical benefit that can be achieved by endovascular renal artery intervention in selected patient cohorts.
Tolvaptan use in Ayrshire and Arran: A population-based Study
Graham C1, Dunleavy A1, Singh P1, Imtiaz T1, Porch K1
Background: Tolvaptan was approved by the Scottish Medicines Consortium (SMC) in 2015 for adults with Autosomal Dominant Polycystic Kidney Disease (ADPKD) with eGFR > 30 ml/min and evidence of rapidly progressive disease. Within NHS Ayrshire and Arran we have established a dedicated Tolvaptan clinic to offer this treatment to suitable patients. Eligible patients were identified either by establishing evidence of declining renal function (decline in eGFR ≥5 ml/min in 1 year or 2.5 ml/min per year over 5 years) or risk of rapid progression based on calculation of MRI guided total kidney volume adjusted to the patients’ height and Mayo classification. Due to the relatively small numbers of eligible patients we have been able to closely monitor uptake, side effects and early indications of effectiveness in slowing the progression of chronic kidney disease (CKD).
Aim: To assess the tolerability and effectiveness of Tolvaptan in slowing the progression of CKD in patients with Autosomal Dominant Polycystic Kidney disease in NHS Ayrshire and Arran.
Method: Information was gathered for all patients who were eligible for Tolvaptan therapy. This included baseline eGFR, pre-treatment rate of decline in eGFR and Mayo classification, where available. We recorded the reasons for some patients declining, and/or stopping treatment. For those remaining on treatment we compared decline in kidney function using MDRD GFR over a 2 year pre and 2 year post drug initiation time-frame. Assays were performed by biochemistry departments across NHS Ayrshire and Arran hospital sites. Over this time-frame patients were also monitored regularly for adverse effects by clinical assessment and measurement of routine biochemical markers.
Results: 36 individuals were deemed suitable for treatment with Tolvaptan. Of the 36, 6 opted not to commence therapy. 2 patients were removed due intolerable side effects developing within the first month of treatment. This left 28 patients, all of whom were on tolvaptan for at least 6 months. 14 discontinued treatment for a variety of reasons including the drug being incompatible with personal circumstances and lifestyle, and adverse effects. The adverse effects resulting in treatment cessation were insomnia, bloating and persistently deranged liver function on biochemical assessment. A further 6 of the initial 28 patients showed evidence of mildly deranged liver function, which was managed by either dose reduction or temporarily withholding tolvaptan. One patient developed malignant melanoma so stopped tolvaptan. Of the remaining 14 patients there was evidence of a clear slowing of decline in renal function after commencing treatment, at various time points measured. Mean decline in MDRD GFR over a 2-year time period before commencing treatment was 11.086 ml/min/1.73 m2(±4.988) compared to 2.975 ml/min/1.73 m2(±4.094) in the 2 years after commencing treatment.
Conclusion: Our study demonstrates that Tolvaptan is effective in slowing the rate of decline in renal function in patients with ADPKD but it is a medication that is limited by its side effects and significant lifestyle implications.
Low dose versus standard dose Rituximab for induction and maintenance treatment of ANCA-associated vasculitis in elderly: A single centre experience
1Renal Unit, Aberdeen Royal Infirmary, Aberdeen, UK
2Vasculitis and Lupus Clinic, Aberdeen Royal Infirmary, Aberdeen, UK
Background and Aims: Cyclophosphamide/glucocorticoids followed by azathioprine have been the standard therapy for remission induction and maintenance treatment of ANCA-associated vasculitis (AAV) for decades. Successful randomised controlled trials using Rituximab supported the use of this agent as first line therapy for both remission induction and maintenance. Elderly patients were under-represented in these trials. Advanced age is known to be associated with increased mortality in AAV. It is unclear whether low dose Rituximab is comparable to standard dosing in achieving and maintaining remission in elderly patients. We report our single centre experience of using low dose Rituximab (LDR) and standard-dose Rituximab (SDR) for both remission induction and maintenance in elderly patients.
Method: We compared the outcome of three treatment strategies in the elderly patients who presented with AAV to our Vasculitis clinic from 1st of July 2007 to 13th of June 2019. These strategies included LDR, SDR and Cyclophosphamide/Azathioprine (Cyc/A). All patients received oral glucocorticoids during remission induction and maintenance. LDR patients received two doses of 500 mg Rituximab fortnightly as remission induction followed by six monthly 500 mg doses for 2 years as maintenance. SDR patients received 2 doses of 1g Rituximab fortnightly followed by six monthly 1g doses for 2 years. Cyc/A patients received 1.5 mg/kg oral Cyclophosphamide for 3 months followed by 18 months of Azathioprine.
Results: Among 60 AAV patients, 17 received LDR regimen, 14 received SDR regimen and 29 were treated with Cyc/A. 51% of patients were males and mean age was 79.6 + /- 4 (LDR), 72.4 + /- 7.2 (SDR), and 71.1 + /- 5 (Cyc/A), p = 0.001. There were no significant differences in pre-treatment serum creatinine, BVAS scores or CRP between groups. None of the patients in the LDR or SDR groups were dialysis dependent at 1 year. Serum creatinine at 24 months from diagnosis was 150 ( + /-30) µmol/L for LDR and 139 ( + /-32) µmol/L for SDR, p = 0.75. At 24 months, patient survival was 76% (LDR), 92% (SDR), and 68% (Cyc/A), p = 0.07. Lower respiratory tract infection was the commonest cause of death. The mean glucocorticoid dose at 3 months of remission induction was significantly lower in the LDR (7.6 + /- 1.7) mg/day and SDR (8.6 + /- 3.1) mg/day compared with Cyc/A (12.5 + /- 3.6) mg/day, p = 0.001. The number of patients requiring hospital admission due to infections were 5/17 (30%) in LDR, 5/14(36%) in SDR and 17/29 (58%) in Cyc/A, p = 0.9, during the 24 months period.
Conclusion: In this single centre observational study, we found that low dose Rituximab used for both remission induction and maintenance in AAV was associated with similar patient outcomes compared to standard dose. The use of low dose Rituximab did not improve the rate of infections despite reduced steroid exposure.
Can cardiopulmonary exercise test results predict the length of critical care stay in patients undergoing simultaneous kidney pancreas transplant?
Lucija Ana Kovacic1, Dr Mortimer Kelleher1, Dr Helen Usher1, Mr Shaun Baxter1, Mr Aaron Hui1, Mr Andrew Sutherland1, Ms. Hillary Guthrie1, DrEuan Thomson1
1Royal Infirmary of Edinburgh, NHS Lothian
Introduction: Cardiopulmonary exercise testing (CPEX) has been able to accurately predict patient mortality, graft outcomes and length of hospital stay in some solid organ transplants (such as liver and kidney), however, no study has so far been published that has examined the ability of CPEX to predict non-cardiac outcomes in patients undergoing simultaneous kidney pancreas (SKP) transplant. We aimed to determine the ability of CPEX to predict outcomes in SKP transplant patients.
Methods: A single centre retrospective analysis of patients that underwent SKP transplant at Edinburgh Transplant Centre between 2011 and 2020 was carried out. Patients were included if they had performed at least one CPEX prior to surgery and if their complete results were available. Five CPEX variables were included in the study (peak oxygen consumption (VO2peak), anaerobic threshold (AT), peak workload (Wpeak), oxygen pulse (VO2/HR), ventilatory equivalent for carbon dioxide (VE/VCO2). The primary outcome was the length of postoperative critical care unit stay. Additional data was collected for length of critical care and hospital stay, mortality and graft outcomes.
Main results: 156 patients underwent SKP transplant at Edinburgh Transplant Centre in the 9-year period. 8 patients were excluded from the final analysis: 4 patients as they did not perform a CPEX and 4 as they had incomplete data available. Mean length of stay in critical care was 9.59 days (SD: 7.47 days). Univariate analysis found no significant association between CPEX and length of critical care stay (VO2peak: r2 = 0.0080, p = 0.281; AT: r2 = 0.0035, p = 0.511; Wpeak: r2 = 0.0034, p = 0.486; VO2/HR: r2 = 0.0229, p = 0.067; VE/VCO2: r2<0.0001, p = 0.982). To correct for cofounders, stepwise linear regression with backward elimination was performed. It identified five other recipient characteristics that had a significant influence on the length of critical care stay (age: p = 0.028, BMI: p = 0.049, pre-transplant CVA and blindness: p = 0.0093 and p = 0.036, length of pre-transplant dialysis: p = 0.007). Average length of hospitalisation was 19.27 days (SD: 11.67 days). When comparing CPEX results for other secondary outcomes (mortality, rejection episodes and insulin independence), there was no significant between-group difference in CPEX variables.
Conclusion: In our population, CPEX had limited ability at predicting the length of critical care and hospital stay, and did not predict mortality or graft outcomes post-transplant in our study cohort. A possible explanation for this is exclusion of patients with poor CPEX result from being listed for SKP transplant which reduces the sensitivity of CPEX to predict length of critical care stay. Future studies are needed to further evaluate this relationship.
Analgesic use and associated adverse events in patients with chronic kidney disease: a systematic review and meta-analysis
1Division of Population Health and Genomics, University of Dundee, Dundee
2Renal Unit, Ninewells Hospital, Dundee
Background: Pain is one of the commonest symptoms experienced by patients with chronic kidney disease (CKD), with an estimated prevalence of 60%. At an individual level, overall quality of life is profoundly affected by pain and CKD, whilst also representing a significant economic burden for healthcare systems globally. Treating pain in the context of CKD is challenging due to altered pharmacokinetics and pharmacodynamics, with an increased risk of toxicity and drug adverse events (AE) in this population. The aims of this systematic review and meta-analysis were to assess the prevalence of analgesic use and establish the risk of analgesics-related AE, in patients with CKD.
Methods: The protocol of this systematic review was prospectively registered on PROSPERO. PRISMA guidelines were followed. Medline, Embase, CINAHL and CENTRAL were searched until January 2021. Screening, and risk of bias assessment were performed by two independent reviewers. Random-effect meta-analyses and meta-regression were conducted to pool and summarise prevalence data as well as measures of association between analgesic use and AE.
Results: Sixty-two studies relevant to the prevalence of analgesic use and thirty-three to analgesic-related AE were included, combining data on 2.3 and 3 million individuals respectively. Meta-analyses showed that 41% (35 to 48) of the CKD population regularly use analgesia. The annual period prevalence was estimated at 51% (43 to 58) for opioids and 21% (10 to 37) for NSAIDs. Twenty percent and seven percent of patients with CKD are on chronic opioid or NSAID therapy respectively. Chronic analgesic use was most common among the dialysis subgroup, with prevalence of 23% for opioid and 17% for NSAIDs. Opioid use was associated with a significantly increased risk of death (HR = 1.61, 1.12 to 2.31, n = 7 studies, I2 = 91%), hospitalisation (RR = 1.38, 1.32 to 1.45, n = 2, I2 = 0%, for high doses) and fractures (RR = 1.51, 1.16 to 1.96, n = 3, I2 = 54%). The association between opioid consumption and mortality followed a dose-dependent relationship with a pooled HR ranging from 1.12 (0.87 to 1.45) when considering the lowest doses to 1.89 (0.90 to 3.94) when considering the highest doses. Evidence was in favour of a lack of association between NSAIDs consumption and CKD progression (RR = 0.94, 0.78 to 1.14, n = 3 studies, I2 = 0%). Although individual studies systematically reported a positive association, random-effect meta-analysis failed to identify any significant relationship between NSAIDs use and CV events (RR = 1.28, 0.72 to 2.28, I2 = 80%) or risk of GI bleeding (RR = 1.86, 0.35 to 9.97, I2 = 97%). This was potentially due to the low number of studies included (n = 3). Five studies consistently reported common and sometimes severe symptoms of neurological impairment such as comatose, lethargy, drowsiness, among patients undergoing dialysis prescribed gabapentinoids.
Conclusion: High levels of analgesic consumption and related serious adverse outcomes were found in patients with CKD. High-quality randomised controlled trials investigating the safety as well as the efficacy of analgesics among patients with a reduced eGFR are required in order to increase the level of evidence.
Outcomes of COVID-19 in patients with CKD: A Scottish observational study
Emilie Lambourg2, Moneeza Siddiqui1, James Chalmers3, Samira Bell1,2
1Renal Unit, Ninewells Hospital, Dundee,
2Population Health Sciences Division, University of Dundee, Dundee
3Molecular and Clinical Medicine, University of Dundee, Dundee
Background: Many studies have reported a poor prognosis from COVID-19 infection among patients with reduced eGFR. These findings may be partly explained by the high burden of comorbidities affecting patients with CKD but the impact of CKD itself is unclear.
The aim of this study was to evaluate and quantify the effect of CKD on COVID-19-related deaths, hospitalisations and cardiovascular (CV) events in a Scottish population, using a propensity-score-based method to eliminate confounding factors.
Methods: All adult patients in Tayside and Fife, Scotland, UK with a COVID-19 positive PCR test between 03/2020 and 02/2021 were included in the cohort and further divided into two groups (CKD and non-CKD). Patients were included in the CKD group if their most proximal eGFR was <60 mL/min/1.73 m2 and they had another eGFR measurement<60 at least 90 days before. A Covariate Balancing Propensity Score (CBPS) algorithm was implemented to account for systematic differences in their baseline characteristics. Doubly robust Cox and logistic regression enabled to estimate the effect of CKD on COVID-19 outcomes.
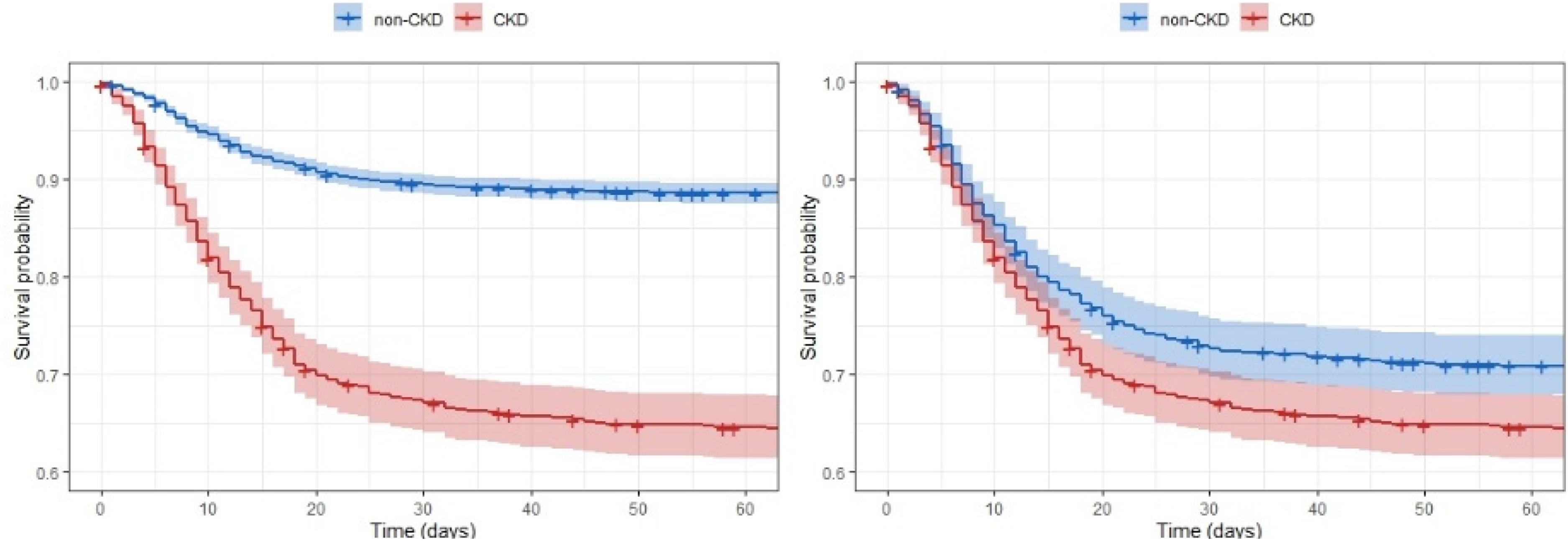
Results: The cohort included 4556 patients (858 with CKD and 3698 without CKD). Patients with CKD were older (84 versus 59 years old, p < 0.001) and had a higher burden of comorbidities. After implementation of the CBPS algorithm, the characteristics of the two groups were similar. Patients with CKD experienced worse outcomes than those without CKD (mortality: 37% versus 12%, hospitalisation: 38% versus 23%, CV events: 12% versus 3%, p < 0.001). Although reduced after CBPS adjustment, those differences remained significant for COVID-19-related deaths and CV events but not for the risk of hospitalisation or the length of stay. The cause specific hazard ratio for COVID-19-related deaths was 3.67 (95% CI 3.17 to 4.24 - logrank test p < 0.001) before CBPS and 1.28 (95% CI 1.07 to 1.52 – p < 0.001) after CBPS adjustment (Figure 1). For all outcomes, the risk magnitude progressively increased as lower eGFR values were reached. Indeed, after CBPS adjustment, having CKD G3A was not associated with a higher risk of COVID-19-related outcomes. However, CKD G4/5 or being on dialysis was associated with an approximately twice higher risk of death and CV event, compared with having a normal renal function (Figure 2 for risk of death).
Unweighted (left) and CBPS weighted (right) survival curves for COVID-19-related deaths (cause specific HR) of patients with (red) and without (blue) CKD.
CBPS adjusted cause specific HR for risk of COVID-19 death across the eGFR spectrum.
Conclusion: Patients with CKD experience worse outcomes following a COVID-19 infection, compared to those with a preserved renal function. A large part of this increase in risk for poor outcomes is related to the greater burden of comorbidities affecting patients with CKD, but our analyses suggest that CKD is also an independent risk factor. The effect of CKD on COVID-19 severity was particularly marked in more advanced CKD stages. Patients with CKD are at increased vulnerability to COVID-19 and should be prioritised for preventive measures such as vaccination.
The risk of site-specific cancer incidence and cancer death in people with CKD: a 5-year landmark analysis
Jennifer S Lees1, Michael K Sullivan1, Frederick Ho1, Solange Parra-Soto1,2, Carlos Celis-Morales1,2, Paul Welsh1, Bhautesh D Jani1, Naveed Sattar1, Ninian N Lang1, Jill P Pell2, Angela C Webster3, Patrick B Mark1
1Institute of Cardiovascular and Medical Sciences, University of Glasgow, Glasgow, UK
2Glasgow Institute of Health and Wellbeing, University of Glasgow, Glasgow, UK
3Sydney School of Public Health, University of Sydney, Sydney, Australia
Background: Cancer incidence and death is observed to be higher in people with chronic kidney disease (CKD), even after adjustment for known risk factors for cancer, and more strongly associated with estimated glomerular filtration rate calculated from cystatin C (eGFRcys) compared with serum creatinine. It has been postulated that the observed association between eGFRcys and cancer outcomes is related to reverse causality. We sought to assess the association between eGFRcys and future risk of cancer incidence and cancer death using methods designed to attenuate the impact of reverse causality.
Methods: Data were from the prospective research cohort UK Biobank, excluding participants with missing biochemistry at baseline, a diagnosis of cancer within 5 years of enrolment (5-year landmark analysis) or a diagnosis of multiple myeloma or renal tract cancer at any time during follow-up (because these cancers and/or their treatments directly cause CKD). eGFRcys was calculated from serum cystatin C using the CKD-EPI equation. eGFRcys >90 ml/min/1.73 m2 was considered the reference. Missing data were multiply imputed by chained equations, using the average of 5 separately imputed datasets. Cox proportional hazards models were constructed to assess the risk of cancer incidence and cancer death, censoring for competing risk of non-cancer death, and adjusted for known risk factors for cancer development, including age and albuminuria. Cox models were sex-disaggregated to explore differential impact of CKD in men and women on cancer outcome.
Results: Of 431,234 participants in UK Biobank with available biochemistry at baseline, 398,803 participants (188,974 men; 209,829 women) met eligibility criteria and were included in the analysis. Beyond 5 years following enrolment, there were 11,990 incident cancer and 3288 cancer deaths in men and 10,899 incident cancers and 2597 cancer deaths in women over a median follow-up period of 11.3 (IQR 10.6–12.0) years. Each 10 ml/min/1.73 m2 reduction in eGFRcys was associated with increased risk of incident lung (men: HR 1.11 (1.06–1.15, p < 0.001); women: HR 1.08 (1.03–1.13, p = 0.001)), abdominal solid organ (men: 1.07 (1.02–1.13, p = 0.005); women: 1.08 (1.01–1.16, p = 0.019)) and haematological (men: 1.11 (1.06–1.16, p < 0.001); women: 1.09 (1.03–1.15, p = 0.003)) cancers. The excess risk of cancer death with each 10 ml/min/1.73 m2 reduction in eGFRcys was most pronounced for haematological (excluding myeloma) malignancies (men: 1.21 (1.11–1.31, p < 0.001); women: HR 1.20 (1.07–1.34, p = 0.001)), but present also for lung (men: 1.10 (1.04–1.16, p = 0.001); women: 1.12 (1.05–1.19, p < 0.001)), digestive (men: HR 1.09 (1.04–1.15, p = 0.001); women: HR 1.10 (1.02–1.18, p = 0.010)) and abdominal solid organ cancers for men only (men: HR 1.11 (1.05–1.18, p < 0.001); women: HR 1.05 (0.97–1.13, p = 0.236)). There was no association between eGFRcys and risk of male or female reproductive tract cancers or melanoma.
Conclusions: Using a 5-year landmark analysis and excluding participants with cancers known to be associated with CKD development, declining eGFRcys is associated with a rising risk of site-specific cancer incidence and death. The reasons for worse cancer outcomes in CKD are unexplained, but may include more invasive stage at presentation, more rapid disease progression, and/or a differential approach or response to cancer treatments. Specific investigation is warranted to identify the mechanisms involved, in order to improve cancer outcomes in people with CKD.
Transplant nephrectomy in the West of Scotland - descriptive analysis of 16 years of data
Luis Loureiro Harrison1, Jamie Traynor1
1Glasgow Renal and Transplant Unit, Queen Elizabeth University Hospital, Glasgow
Introduction: Current common clinical practice is to leave a renal graft in situ once the transplant fails, unless an indication for transplant nephrectomy develops. This procedure can be performed for uncontrolled rejection, which is clinically termed graft intolerance syndrome (GIS), as well as infection, infarction, malignancy, and to create space for re-transplantation.
Aims: In this study we aimed to 1) identify the incidence of transplant nephrectomy and the indications for it 2) identify the 30-day mortality rate for the procedure 3) analyse potential differences between patients who undergo nephrectomy for different indications at the point of transplant failure, which could potentially lead to further work on predicting the need for transplant nephrectomy.
Methods: We queried the Strathclyde Electronic Renal Patient Record (SERPR) which includes patients receiving transplantation and follow up across the West of Scotland. We identified patients with renal transplant failure between 1st January 2004 and 31st December 2019. Data on subsequent nephrectomy were collected up to 8th July 2021. We identified those who underwent transplant nephrectomy of their first transplant, and excluded those younger than age 18 at nephrectomy, and those whose transplant failure occurred outside the remit of our database. We reviewed clinical entries to determine the indication for the procedure. We collected data on the timing of the procedure, mortality, and a selection of inflammatory markers including neutrophil count, neutrophil:lymphocyte ratio, albumin, and CRP, as well as markers of excretory function and proteinuria at failure, including eGFR (CKD-EPI), eGFR slope for the 12 months before failure, and urine protein:creatinine ratio (uPCR). Data on degree of mismatch was not available for a sufficient number of patients to make analysis of this parameter meaningful.
Results: We identified 556 patients with transplant failure, of which 473 patients experienced failure of a first renal transplant. 452 patients remained after exclusions applied. A total of 124 patients underwent transplant nephrectomy by follow-up, and 328 did not undergo transplant nephrectomy by follow-up or death, meaning 27.4% of failing first renal transplants led to a transplant nephrectomy. 48 patients underwent nephrectomy for GIS, with infection (n = 17) and infarction (n = 16) being the next commonest indications. 43 of 48 nephrectomies for GIS were performed within one year of transplant failure, compared to 70 of 76 for other indications. GIS represented a minority of nephrectomies performed acutely (within 30 days of transplantation), with vascular complications such as infarction (n = 13), vein thrombosis (n = 9) and bleeding (n = 5) being more common. 30-day mortality overall was 3.23%, with nephrectomies performed for GIS having a slightly higher mortality than other indications (4.17% versus 2.63%).
Compared to those who did not undergo nephrectomy, patients who underwent nephrectomy for GIS were younger (median 38.68 years versus 48.46, p < 0.001), had shorter-lasting grafts (median 4.05 years versus 9.95, p < 0.001), and had shorter renal replacement therapy careers (median 7.55 years versus 12.49, p < 0.001), as well as lower eGFRs at failure (6.5 versus 7.4, p = 0.0093) and steeper eGFR slopes (-0.056 versus −0.033, p = 0.0022). Compared to those who did not undergo nephrectomy, patients undergoing nephrectomy for non-GIS indications were older (median 52.12 versus 48.25 years old, p = 0.025), had markedly shorter graft survival (median 0.41 versus 9.95 years, p = <0.001), shorter RRT careers (median 4.29 versus 12.49 years, p < 0.001). There were also differences in neutrophil count (median7.51 versus 5.53, p < 0.001), neutrophil:lymphocyte ratio (median 8.24 versus 6.00, p = 0.0010), albumin (median 28.00 versus 33.00, p < 0.001), CRP (median 42.00 versus 11.0, p < 0.001) and eGFR (median 8.00 versus 7.40, p = 0.042).
Conclusion: GIS was the commonest indication for transplant nephrectomy in our patient group. The vast majority of nephrectomies performed within a month of transplantation were for vascular complications in the post-operative period. Mortality for the procedure was low, albeit slightly higher for GIS. Even at the point of transplant failure, which can predate nephrectomy by several months, those undergoing subsequent nephrectomy for non-GIS indications had evidence of inflammatory response compared to those who did not undergo nephrectomy.
Predicting outcomes in kidney biopsy proven ANCA-Associated Vasculitis: the complete Scottish experience
Dr Dominic P. McGovern1,2, Dr Jennifer S. Lees1,2, Dr Jamie Smith3, Dr Dana Kidder3, Dr Bruce Mackinnon4, Dr Colin C. Geddes1,2, Dr Emily P. McQuarrie1,2, Dr Kate I. Stevens1,2
1Glasgow Renal & Transplant Unit
2University of Glasgow
3University of Aberdeen
4Department of Nephrology & Hypertension, John Hunter Hospital, New South Wales, Australia
Background and Aims: Predicting outcomes in ANCA-associated vasculitis (AAV) remains challenging for clinicians. We aimed to establish if a clinicopathologic renal risk score (RRS) could accurately predict outcomes in a national cohort of patients with AAV proven on kidney biopsy(1).
Method: The Scottish Renal Biopsy Registry is a complete national dataset of all renal biopsies performed in Scotland. We included all first kidney biopsies with evidence of AAV that were performed between 2014 and 2017. Patients with dual PR3/MPO positivity were excluded. Demographic and histological data and outcomes of interest (including relapse, end-stage kidney disease and death) were recorded. The RRS is a combination of individual scores attributed to the % of normal glomeruli, % of tubular atrophy/interstitial fibrosis and eGFR (CKD-EPI) at time of biopsy. Depending on this summative score, patients are then defined as low, medium or high risk. Survival analyses were conducted using Cox proportional hazard models for survival to ESKD, relapse and death, stratified by risk category. Statistical analyses were conducted using R software.
Results: We identified 241 eligible patients for inclusion in the study: 38 (15.8%) relapsed, 35 (14.5%) progressed to ESKD and 54 (22.4%) died. The patients were stratified into low (n = 123 (50%)), medium (n = 112 (46%)) and high (n = 11 (5%)) risk groups respectively. Mean age at biopsy was 66.7 ± 12.2 years and 48% (n = 112) were female; this was similar across the risk groups. Within the high-risk group, we noted a lower mean eGFR (high 8.6 ± 6.1 versus low risk 45.7 ± 26.0 ml/min/1.73 m2, p < 0.001) and higher level of proteinuria (high 405 (IQR 170–767) versus low risk 81 (IQR 41–155) mg/mmol, p < 0.001). Ninety-one (38%) were PR3 positive and these patients were over-represented in the high risk compared with the low risk category (70% versus 43% respectively; p = 0.006). Pulmonary haemorrhage was also observed more frequently in high risk patients (7% low risk, 6% medium risk and 20% high risk (p = 0.294)). High risk patients were more likely to receive plasma exchange (80% versus 9%; p < 0.001) and/or haemodialysis (70% versus 2%; p < 0.001) compared with low risk patients. The risk of relapse was most significant for those in the low risk group (low risk: 21.3%; medium risk 11.0%; high risk 0.0%; p = 0.038). On Cox proportional hazards analysis, adjusted for age, sex, PR3/MPO status, proteinuria, steroid treatment, cyclophosphamide or plasma exchange, initial renal replacement therapy (HR 4.6 (95% CI 1.4–14.7); p = 0.011) and RRS (medium risk: HR 9.3 (95% 2.1–42.1); p = 0.004; high risk: HR 29.9 (95% CI 3.7–239.7); p = 0.001) were associated with higher risk of ESKD. If eGFR is also adjusted for, the RRS continues to be associated with an increased risk of ESKD (high risk: HR 14.9 (95% CI 1.74–128.84); p = 0.014). Also, a higher RRS was associated with a trend towards increased risk of death (HR 1.14 (95% CI 0.99–1.31); p = 0.073).
Conclusion: This simple RRS, proposed first in 2018, which is calculated using routinely collected clinical and pathological data, is helpful in predicting progression to ESKD in those with AAV proven at kidney biopsy. It is also of interest that relapse was more frequent in the patients of the low risk category. This could be explained by reduced irreversible damage in this group, or perhaps immunosuppression was tailored more rapidly for those with less severe disease at presentation. A unique strength of our findings is that they are based on a complete national dataset, thus reducing susceptibility to bias from variations in regional diagnostic and therapeutic practices.
Reference
1.Brix SR, et al. Development and validation of a renal risk score in ANCA-associated glomerulonephritis. Kidney Int. 2018 Dec; 94(6): 1177–1188. doi: 10.1016/j.kint.2018.07.020
The association of deprivation with outcomes in kidney biopsy proven ANCA-associated vasculitis in a complete national cohort
Dominic P. McGovern1,2, Jennifer S. Lees1,2, Bruce Mackinnon3, Colin C. Geddes1,2, Emily P. McQuarrie1,2, Kate I. Stevens1,2
1Glasgow Renal & Transplant Unit
2University of Glasgow
3Department of Nephrology & Hypertension, John Hunter Hospital, New South Wales, Australia
Introduction: Deprivation is associated with poorer patient outcomes and has specifically been associated with a two-fold increase in mortality in cases of primary glomerulonephritis (1). However, the impact of deprivation on outcomes in ANCA associated vasculitis (AAV) has not yet been fully described. We aimed to establish if socioeconomic deprivation is associated with disease severity at presentation and if it has an impact on clinical outcomes in AAV in a complete national cohort.
Methods: The Scottish Renal Biopsy Registry is a complete national dataset of all kidney biopsies performed across Scotland. Patient demographics, laboratory parameters including histopathology, treatment modalities and outcomes are recorded retrospectively. We included patients with AAV proven on first kidney biopsies that were performed between 2014 and 2017 inclusive. We used the quintiles of the validated Scottish Index of Multiple Deprivation (SIMD) as a measure of relative socioeconomic deprivation for each patient. A previously validated renal risk score (RRS) – which combines weighted scores for presentation eGFR (CKD-EPI) and histopathological data from biopsy – was calculated and patients were defined as high, medium or low risk depending on their score (2). Cox proportional hazard models were created for survival to ESKD, relapse and death and were stratified by deprivation quintile. Statistical analyses were conducted using R software.
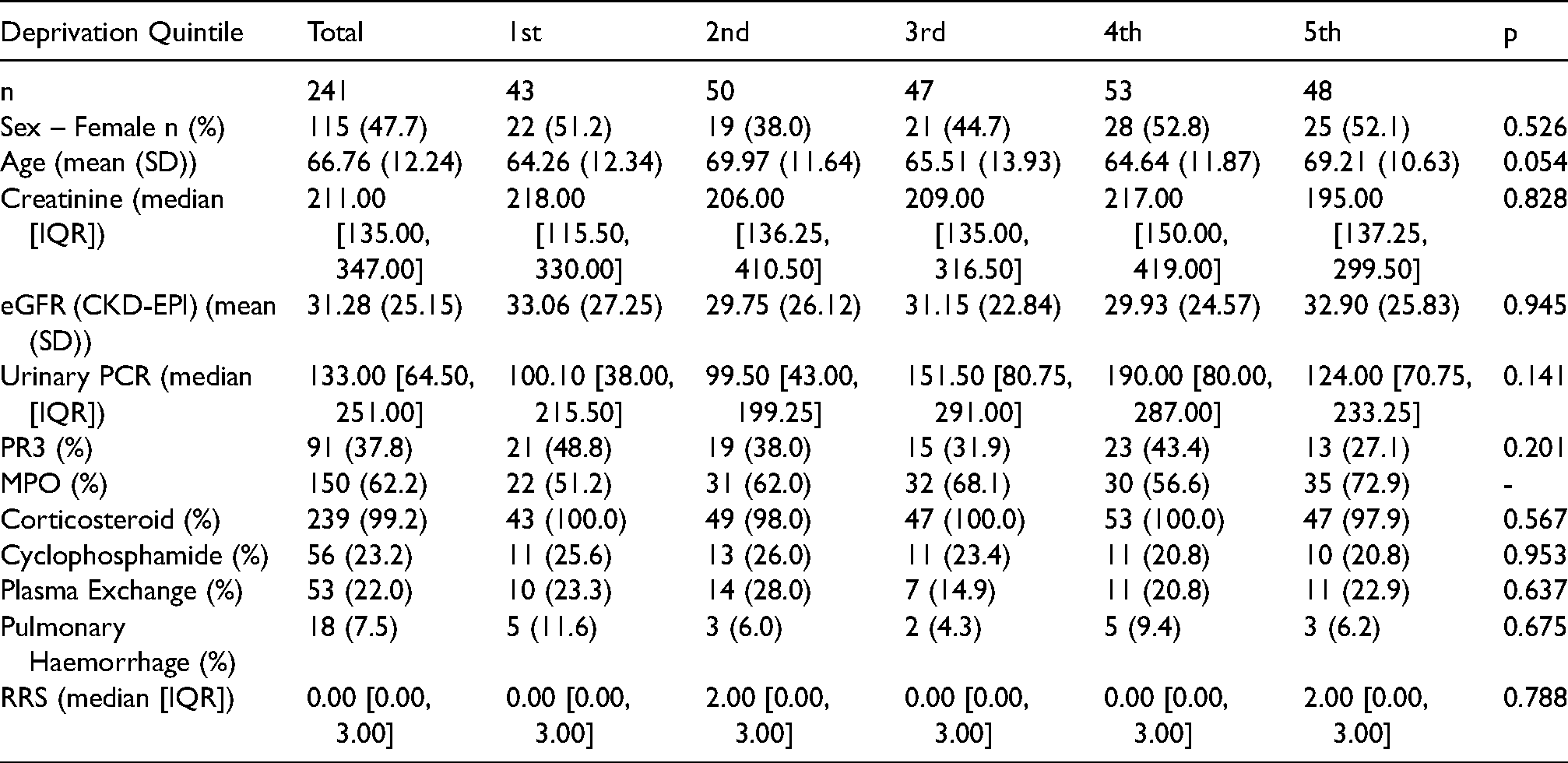
Results: In total, 241 patients met our inclusion criteria. There were 115 (48%) female patients and mean age at biopsy was 66.7 ± 12.2 years. For renal risk score, 50.6% (n = 122), 45.2% (n = 109) and 4.1% (n = 10) were classed as low, medium and high risk respectively. Baseline demographic data by deprivation quintile are displayed in Table 1. We noted a trend of those in the least deprived quintile being older (least deprived 69.2 ± 10.3 versus most deprived 64.3 ± 12.3 years; p = 0.054). Otherwise, no significant difference between deprivation quintiles was observed for baseline demographics, initial investigation results, immunosuppression modalities or the presence of pulmonary haemorrhage. After adjustment for age, sex, PR3/MPO status, eGFR, proteinuria, renal risk score, requirement for kidney replacement therapy initially, treatment with steroid, cyclophosphamide and plasma exchange, relative socioeconomic deprivation was not associated with relapse or ESKD but was associated with an increased risk of death (HR 3.44 (1.02–11.57, p = 0.046) in most deprived compared to least deprived SIMD quintiles).
Conclusion: The health inequalities that exist in Scottish society due to significantly varying levels of deprivation are well recognised. In spite of this, we did not demonstrate an association with deprivation and worse kidney outcomes in AAV, but higher levels of relative socioeconomic deprivation are associated with an increased risk of death in this patient cohort. Regardless of deprivation quintile, patients with AAV, who undergo kidney biopsy, appear to be identified, referred and treated to the same standard and renal outcomes are similar regardless of the level of deprivation. The main strength of this study is that it is based on a national cohort and is therefore less susceptible to regional variations in diagnostic and therapeutic approach.
References
1. McQuarrie, Emily P., et al. "Multiple socioeconomic deprivation and impact on survival in patients with primary glomerulonephritis." Clin. Kidney J 10.1 (2017): 49–54.
2. Brix, Silke R., et al. "Development and validation of a renal risk score in ANCA-associated glomerulonephritis." Kidney international 94.6 (2018): 1177–1188
Baseline Demographic Data by Deprivation Quintile
Deprivation Quintile
Total
1st
2nd
3rd
4th
5th
p
n
241
43
50
47
53
48
Sex – Female n (%)
115 (47.7)
22 (51.2)
19 (38.0)
21 (44.7)
28 (52.8)
25 (52.1)
0.526
Age (mean (SD))
66.76 (12.24)
64.26 (12.34)
69.97 (11.64)
65.51 (13.93)
64.64 (11.87)
69.21 (10.63)
0.054
Creatinine (median [IQR])
211.00 [135.00, 347.00]
218.00 [115.50, 330.00]
206.00 [136.25, 410.50]
209.00 [135.00, 316.50]
217.00 [150.00, 419.00]
195.00 [137.25, 299.50]
0.828
eGFR (CKD-EPI) (mean (SD))
31.28 (25.15)
33.06 (27.25)
29.75 (26.12)
31.15 (22.84)
29.93 (24.57)
32.90 (25.83)
0.945
Urinary PCR (median [IQR])
133.00 [64.50, 251.00]
100.10 [38.00, 215.50]
99.50 [43.00, 199.25]
151.50 [80.75, 291.00]
190.00 [80.00, 287.00]
124.00 [70.75, 233.25]
0.141
PR3 (%)
91 (37.8)
21 (48.8)
19 (38.0)
15 (31.9)
23 (43.4)
13 (27.1)
0.201
MPO (%)
150 (62.2)
22 (51.2)
31 (62.0)
32 (68.1)
30 (56.6)
35 (72.9)
-
Corticosteroid (%)
239 (99.2)
43 (100.0)
49 (98.0)
47 (100.0)
53 (100.0)
47 (97.9)
0.567
Cyclophosphamide (%)
56 (23.2)
11 (25.6)
13 (26.0)
11 (23.4)
11 (20.8)
10 (20.8)
0.953
Plasma Exchange (%)
53 (22.0)
10 (23.3)
14 (28.0)
7 (14.9)
11 (20.8)
11 (22.9)
0.637
Pulmonary Haemorrhage (%)
18 (7.5)
5 (11.6)
3 (6.0)
2 (4.3)
5 (9.4)
3 (6.2)
0.675
RRS (median [IQR])
0.00 [0.00, 3.00]
0.00 [0.00, 3.00]
2.00 [0.00, 3.00]
0.00 [0.00, 3.00]
0.00 [0.00, 3.00]
2.00 [0.00, 3.00]
0.788
Kidney replacement therapy choices – a challenge for patients and professionals
K. Neilly1, T. Harkness1, A.Almond1, M.Kelly1, N.Rathnamalala1, T. Muniraju1
1Renal Unit, Mountainhall Treatment Centre, Bankend Road, Dumfries, DG1 4AP
Background: Decision making around kidney replacement therapy (KRT) is complex and sensitive. Those nearing end stage kidney disease should be offered information about all treatment modalities available to them and should be able to make informed decisions with their families and carers.[1]
Aims: To assess the challenges faced by patients and their clinicians in making KRT decisions.
Methods: Patients with eGFR 20 or below were referred to the kidney care planning (KCP) pathway for KRT counselling in Dumfries and Galloway. Patients received counselling on KRT and conservative care by the same KCP nurse. This counselling took place at the patient's home with their family member(s) if available. The same literature was given to all patients. Data was collected prospectively with initial choice of KRT as indicated by the patient, patient's family if available and KCP nurse. Other demographics were recorded including age, co-morbidities, primary kidney diagnosis, rate of decline in kidney function, distance from HD unit as well as their Frailty Assessment for Care-Planning Tool Score[2] and distance from nearest relative if living alone. This data was then sent anonymously to four doctors, three nurses and one dietitian who indicated their KRT recommendation.
Results: During the study period of August 2018 to May 2021, 50 patient's data was collected. Decision making was proven to be complex. Within the doctor group agreement on KRT modality was the same in 7 of the 50 patients. In the other healthcare professional group (nurses and dietitian) the recommended modality was the same in 5 out of 50. One patient had the same KRT recommendation indicated by all healthcare professionals. Greatest agreement was seen between the KCP counsellor and the patient and family. Of the 50 initial patients 44 were followed up to 12 months with 4 patients dying within the initial 12 months.
Conclusions: KRT choices are complex with various factors influencing the decision making process. While some qualitative studies have examined factors influencing patient decisions, factors that affect health care professionals and their interactions with the patient decision making process is largely unexplored.[3,4] In our study, it appears that decision making is influenced by some of the data provided, in particular the frailty score, age and co-morbidities. Clinician's recommendations are also subject to their own biases in KRT preference. Greatest agreement in KRT modality was seen between the KCP nurse and patients and family. This nurse was the only healthcare professional to meet with the patient and family highlighting the influence of face-to-face interaction. It is clear we need more evidence and decision making tools to guide both patients and professionals with KRT choices.
References
1.NICE. Renal replacement therapy and conservative management. NICE guidelines 2018
2.Accreditation Canada. Frailty Assessment for Care Planning Tool (FACT). 2014.
3.Morton RL, Tong A, Howard K, et al. The views of patients and carers in treatment decision making for chronic kidney disease: Systematic review and thematic synthesis of qualitative studies. BMJ 340: c112, 2010. PMID: 20085970
4.Murray MA, Brunier G, Chung JO, et al. A systematic review of factors influencing decision-making in adults living with chronic kidney disease. Patient. Educ. Couns. 2009 Aug; 76(2): 149–58. doi: 10.1016/j.pec.2008.12.010. PMID: 19324509.
A Misplaced HeRO (Haemodialysis Reliable Outflow Graft)
Ahmed Fouad Omar1,Shilen Shanghavi2, Konstantinos Koutroutsos2
1Aberdeen Royal infirmary, NHS Grampian, Scotland
2Royal Sussex country hospital, University hospitals of Sussex ,Brighton
Abstract: A multitude of medical implants exist, especially within the field of vascular access. This report features a case in which a 38-year-old gentleman with end stage renal disease presented to the renal unit. On examination, an audible sound was heard over the tricuspid valve and further investigations revealed that his haemodialysis reliable outflow (HeRO) graft had broken; a segment greater than 20cm in length migrated into his heart. This is the first report of such an occurrence without an obvious precipitant, and emphasises the importance of both a thorough examination in all presentations and being aware of foreign bodies that are implanted into patients.
Case presentation: A 38 year-old gentleman with a history of end stage renal disease in childhood due to posterior urethral valves and cystic dysplastic kidneys, for which he was on his third renal transplant, presented to the renal unit with kidney allograft dysfunction. Physical examination revealed a soft abdomen with no pain over the transplant and clear lung fields, but a high-pitched sound was heard over the tricuspid valve with no clear explanation. The chest x-ray revealed a foreign body, thought to be in the retro-cardiac region. A transthoracic echocardiogram showed a long tubular structure entering the right atrium, going into the right ventricle through the tricuspid valve and looping back around the apex, back into the right atrium. There was also evidence of mild to moderate tricuspid regurgitation caused by tube entering and leaving the tricuspid valve.
With these findings, a review of previous imaging and the patient's history revealed that part of a haemodialysis reliable outflow (HeRO) graft, placed 4 years earlier, had detached and migrated into the heart. The cardiology team performed a successful trans-femoral retrieval of the graft, which measured over 20cm in length.
Acute kidney injury associated with checkpoint inhibitors – clinical features and outcomes of cases referred into the Glasgow Renal Unit.
Dr Eleanor Parkhill1, Dr Jennifer Lees1, Dr Keith Gillis1, Dr Mark Findlay1
1Glasgow Renal & Transplant Unit
Background: Checkpoint inhibitors (CPI) are novel immunotherapy agents used to treat solid and haematological malignancies. Since clinical adoption, the clinicopathological features of CPI nephrotoxicity has been demonstrated in several case series. The Glasgow experience of CPI associated nephrotoxicity is described here.
Methods: A retrospective analysis was conducted of all patient records that referenced checkpoint inhibitors. All cases of acute kidney injury (AKI) deemed to be associated with CPIs by either the oncologists or nephrologists involved in their care were included. Detail on demographics, comorbidities, CPI choice, dose and duration, concomitant medications, biochemistry, treatment, and outcomes were extracted manually.
Results: Twenty-six cases of AKI associated with CPI were identified. The first referral was received in July 2017. Mean age at referral was 67.9 years (SD 8.7), and 69% (18) were male. Comorbid hypertension was present in 58% (15), and 73% (19) were on a proton pump inhibitor. Median baseline creatinine was 96 µmol/L (IQR 79–103), with median change at presentation 127 µmol/L (IQR 99–199). At presentation 42% (11) had low bicarbonate, and 46% (12) had new proteinuria of > 50 mg/mmol. Most cases were referred on admission or on development of AKI (17), with delayed referrals often prompted by an incomplete or failed recovery (4), and once on considering rechallenging. Three cases underwent renal biopsy – showing acute interstitial nephritis (2) or chronic interstitial nephritis (1). Most clinical diagnoses were of immune related nephritis (18), with 2 cases of immune related tubular acidosis. In 85% (22) of cases, the CPI was stopped and in 92% (24) high dose steroids were commenced. Eleven individuals required steroid course of > 6 weeks. Median time to maximum renal recovery was 55 days (IQR 36–115), and 81% (21) made a complete renal recovery. Fourteen patients (54%) had died at the time of data collection, median time to death was 324 days (IQR 36–465), and 38% had died within a year from maximal creatinine. In cases where CPI was stopped, median survival was 426 days (IQR 270–592), compared to 743 days (IQR 599–984) when CPI was not stopped (W = 72, P = 0.048).
Conclusions: Since 2017 there were 26 cases of CPI associated nephrotoxicity referred to the local nephrology unit. Presentation was commonly an interstitial nephritis, often with an associated acidosis or proteinuria. Majority of patients were clinically diagnosed and treated empirically, and had a good renal response to steroids. Survival was significantly shorter when CPI was not stopped, though numbers where CPI was not stopped in this case series were small.
SGLT2 inhibitor use in secondary care nephrology: Clinical demand and patient distribution
Catherine Russell1, Samuel Birch-Machin1, Jennifer Lees1, Elaine Spalding1, Jack Fairweather1, Emily McQuarrie1, Patrick Mark1, Keith Gillis1
1Queen Elizabeth University Hospital, Glasgow
Introduction: Sodium glucose linked transporter 2 inhibitors (SGLT2i) reduce progression of chronic kidney disease (CKD) both in people with and without diabetes. The distribution of patients who may benefit from this indication across secondary care remains uncertain. We aimed to define how many patients across secondary care nephrology may benefit from SGLT2i.
Methods: We performed a cross sectional study of electronic patient records in secondary care nephrology centres (NHS Greater Glasgow and Clyde, Lanarkshire and Ayrshire and Arran) to assess eligibility for SGLT2i prescription according to clinical trial criteria for kidney outcomes. In the CREDENCE trial of canagliflozin, participants had type 2 diabetes, eGFR >30 ml/min/1.73 m2 and uACR >30 mg/mmol (uPCR >70 mg/mmol); exclusion criteria included prior ketoacidosis. Participants in the DAPA-CKD trial of dapagliflozin had eGFR >15 ml/min/1.73 m2 and uACR >20 mg/mmol (uPCR >50 mg/mmol); exclusion criteria included lupus, vasculitis, and polycystic kidney disease. Additionally, age criteria were set at 18–81 for canagliflozin and 18–86 years for dapagliflozin, according to the age range involved in the relevant clinical trials. Trials of SGLT2i recruited patients on standard of care including angiotensin converting enzyme inhibitors (ACE) or angiotensin receptor blockers (ARB).
Results: Patients were excluded by criteria detailed in table 1. Of 2767 patients with type 2 diabetes, eGFR was 33 ± 24 ml/min/1.73 m2 and age 82 ± 14 years. 1048 (38%) of these were deemed appropriate for SGLT2i after applying licensing criteria. After excluding patients out with the age range, and including only those on ACE or ARB, 272 remained eligible (10%).
In 11889 patients without diabetes, eGFR was 58 ± 33 ml/min/1.73 m2 and age 67 ± 23 years. 6780 patients (57%) were deemed suitable for SGLT2i. After excluding patients out with the age range, and including only those on ACE or ARB, 1245 remained eligible (10%).
Conclusions: The number of patients who may be treated for diabetic kidney disease is dwarfed by those who may be treated for non-diabetic CKD. Although age and co-prescription of ACE or ARB are not absolute contraindications to SGLT2i prescription, these factors may alter clinical decision making and may reduce overall prescribing of therapy.
Canagliflozin
Dapagliflozin
Total
2767
Total
11889
eGFR > 30 ml/min uACR >30 mg/mmol
1058
eGFR> 25 ml/min uACR >30 mg/mmol
7331
No history DKA
1048
No history of lupus, vasculitis, PKD
6780
Age 18–81 years
562
Age 18–86 years
5252
On ACE/ARB
272
On ACE/ARB
1245
How many children and when – a women's reproductive history and her risk of chronic kidney disease in UK Biobank
E Rutherford1, K Stevens,M Sullivan1, P Welsh,S Nelson1, PB Mark1, JS Lees1
1Queen Elizabeth University Hospital, Glasgow
Introduction: Even in pregnancies free from complications, the kidneys undergo profound structural and functional changes. It is well established that a woman's reproductive history alters her future risk of cardiovascular disease. A woman's reproductive history may also influence her future risk of kidney disease, however evidence for this is sparse. We assessed the relationship between several reproductive factors and future chronic kidney disease (CKD) in the UK Biobank.
Methods: Between 2007 and 2010,the UK Biobank recruited over 500,000 participants aged 37–73. Participants gave a detailed reproductive history and had extensive phenotyping and sampling of baseline biochemical measures including kidney functionand albuminuruia. After adjustment for age, Townsend Deprivation Score, BMI, smoking, systolic blood pressure and presence of diabetesCox regression models yielded adjusted hazard ratios for the presence or absence of CKD at entry to UK Biobank for: number of births and age at first birth. Presence of CKD was defined using cystatin c as an estimated glomerular filtration rate of <90 ml/min/1.73 m2 and/or urinary albumin creatinine ratio >3.
Results: We included 254,032 women with available biochemistry and reproductive history at UK Biobank entry. 54,685 (21.5%) women had CKD1–5. Women with CKD were older than those without CKD, had a greater BMI and had a higher blood pressure.Women with CKD had a higher mean number of live births (1.9 ± 1.2 v 1.7 ± 1.2, p < 0.001) and were younger at first live birth (24.5 ± 4.6 v 26.0 ± 4.9 years p < 0.001).On Cox regression, adjusted hazards ratios showed that compared with 0 births, 2 or 3 live births was associated with lower risk of CKD1–5 (1 birth: HR 0.99 (0.95–1.02, p = 0.469, 2 births:HR 0.86 (0.81–0.92, p < 0.001,3 births: 0.88 HR 0.82–0.92, p < 0.001) (Figure 1). Later age at first birth was associated with a reduced HR of CKD: HR 0.99 (0.98–0.99, p < 0.001).
Conclusions: In UK Biobank, compared to women with no births, women who had 2–3 birthshad a reduced risk of CKD.Women who had a later age at their first birth had a reduced risk of CKD. The mechanisms underlying these associationsrequires further exploration.
Is having children bad for your cardiovascular health? Kidney function and risk of incident cardiovascular disease in parents– a UK Biobank Study
E Rutherford1, KI Stevens1, MK Sullivan1, P Welsh1, S Nelson1, PB Mark1, JS Lees1
1Queen Elizabeth University Hospital, Glasgow
Introduction: Multiple studies have shown that the number of children someone has appears to influence their future risk of cardiovascular disease (CVD), including myocardial infarction (MI) and stroke. These studies do not take into account markers of kidney function which strongly influence an individual's CVD risk. We explored whether the number of children a person has influences their future risk of stroke, MI or end stage kidney disease (ESKD)and whether this might be mediated by kidney function in UK Biobank.
Methods: Between 2007 and 2010, the UK Biobank recruited over 500,000 participants aged 37–73. Participants gave a detailed reproductive history and had extensive phenotyping and sampling of baseline biochemical measures including kidney function. Cox proportional hazards models tested associations between number of children and future risk of MI, stroke or ESKD. Models were adjusted for age, Townsend deprivation index, BMI, smoking, systolic blood pressure,presence of diabetesand use of antihypertensives, cholesterol-lowering medications and insulin. Survival was censored for the competing risk of all-cause mortality.We sought evidence ofa multiplicative interaction between sex and number of children.Results are presented before and after adjustment for baseline kidney function (estimated glomerular filtration ratecalculated using cystatin C (eGFRcys) and albuminuria).
Results: We included 244,556 women and 195,170 men without a prior diagnosis of CVD, at UK Biobank entry. Mean age at recruitment was 56.2 ± 8.0 years in women; 56.3 ± 8.2 years in men. Women had given birth to median 2 (IQR 1–2) children; men fathered median 2 (IQR 1–2) children. Median eGFRcys at study entry was91 (IQR 78–104) for women and 89 (IQR 78–101) for men. Over a median follow-up of 11.5 years, 11,136 (4.6%) women and 14,392 (7.4%) men died, 1883 (0.8%) women and 2433(1.2%) men had a stroke (ischaemic or haemorrhagic), 2027 (0.8%) women and 4764 (2.4%) men had a non-fatal MI and165 (0.1%) women, and 269 (0.1%) men reached ESKD. Compared to having zero births, having 4 or more children was associated with an increased future risk ofMI (HR 1.27 (1.14–1.41, p < 0.001) and stroke (HR 1.23 (1.08–1.40, p = 0.002), even after adjustment for eGFRcys and albuminuria (Figure). The association between number of children and MI was stronger in women (p-for interaction <0.001) but not stroke (p for interaction p = 0.627). The number of children was not associated with risk of ESKD before or after adjustment for kidney function markers in either women or men.
Conclusions: There is an increased risk of MI and stroke associated with having increasing numbers of children, even after adjustment for markers of kidney function. Consideration should be given to whether lifestyle factors, including dietary habits and physical activity, may explain this observed association. Further scrutiny in this area may identify modifiable risk factors to attenuate CVD risk in parents.
Total renal chronicity score predicts renal survival in ANCA-associated glomerulonephritis
Ahmed Saleh1, James R Smith1, David P Kaipen2, Moira Davie3, Kathryn I Stevens4, Bruce MacKinnon5, Shona Methven1, Dana Kidder1
1Nephrology Department, Aberdeen Royal Infirmary, United Kingdom
2Pathology Department, Queen Elizabeth University Hospital, United Kingdom
3Pathology department, Aberdeen Royal Infirmary, United Kingdom
4Nephrology Department, Queen Elizabeth University Hospital, United Kingdom
5Nephrology Department, John Hunter Hospital, Australia
Introduction: Evaluating the severity of ANCA-associated glomerulonephritis (AAGN), using histological scoring or a combination of histological scoring plus demographic and laboratory markers, has been shown in several landmark studies to predict the risk of end-stage kidney disease (ESKD). In this study we hypothesised that quantifying total chronicity in AAGN using the scoring system proposed by Sethi et al., can predict renal survival in the Scottish population. The second aim of our study was to compare the total chronicity score to the renal risk score in predicting 1,2 and 3 year outcome.
Methods: We utilised data from the Scottish Renal Biopsy Registry to identify patients with AAGN from two geographically distinct tertiary referral renal units (Aberdeen Royal Infirmary)and Glasgow Renal and Transplant Unit) serving a combined population of >2 million people in Scotland. All patients met the criteria for the Chapel Hill Consensus Conference definition of ANCA-associated vasculitis (AAV). Consecutive AAV patients who had a renal biopsy at diagnosis in these two units between 24/1/2013 and 17/5/2017 were included. Biopsy reports were reviewed and scored by two different pathologists (DKP, MD) and two nephrologists (JRS and DK). Both pathologists were blinded to clinical data and scored the biopsies independently. We measured the performance of individual components of the chronicity score and total score, to predict renal survival at 1,2 and 3 years. We compared the performance of the chronicity score to the recently published renal risk score.
Results: A total of 102 patients were included. More than half of the patients were positive for PR3-ANCA. The median (IQR) eGFR at diagnosis was 20 mL/min/1.73 m2 (10.5–37.7). Nineteen patients (18.6%) required dialysis at presentation. Cyclophosphamide was used for remission induction in 92 (90%) patients. Azathioprine was used for remission maintenance in 76 (74.5%) patients. Glomerulosclerosis score alone demonstrated the best performance in terms of predicting ESKD across all time points (AUC = 0.80 at 1,2 and 3 years), whereas degree of arteriosclerosis performed poorly (AUC = 0.44, at 1 ,2 and 3 years) . The total chronicity score AUC was 0.8 in year 1 and 2 and dropped slightly to 0.77 at year 3 follow-up. Comparison of the total chronicity score to the recently published and validated renal risk score showed closely comparable discriminative abilities. For example, patients in the severe chronicity grade had high renal risk scores of >10.
Conclusion: This study confirms that the total chronicity score in AAGN can predict renal survival. We found that glomerular and tubulointerstitial components of the score have more predictive power compared to arteriosclerosis. The score provides an additional useful tool for clinicians to guide clinical decision making for patients with severe chronicity grades who might not benefit from immunosuppression.
Changes in body mass parameters in a paediatric renal transplant population in different stages of social lockdown during the coronavirus pandemic
Peter Schulga, I Ramage, D King, B Reynolds
Renal Unit, Queen Elizabeth University Hospital, Glasgow
Background: Renal transplant patients are at greater risk of cardiovascular disease than the general population. Excess weight is a significant risk factor for all patients, with weight gain post-transplant a particular concern.
Methods: This retrospective observational study of children attending the renal transplant clinic monitored changes in weight and body mass index over the first 12 months of the SARS-Cov-2 pandemic, during which multiple restrictions on socialising and school attendance occurred.
Results: 46 post-kidney transplant patients at least 6 months post-transplant were included. 26 patients gained weight, 11 patients had stable weight and 9 lost weight. The mean weight z-score across the patient cohort increased from −0.053 at start of lockdown 1, to 0.132 4 months post-lockdown 1, increasing further to 0.196 after lockdown 2. Mean BMI z-score increased from 0.633 at onset of lockdown to 0.788 at end of lockdown 1.
Conclusion: The majority of paediatric post-kidney transplant patients demonstrated increases in weight and BMI z-score over the periods of lockdown. The potential consequences of the pandemic and societal responses continue to emerge.
Moving more is associated with reduced risk of chronic kidney disease: a UK Biobank study
K.I. Stevens1,2, C. Delles2, P.B. Mark1,2, P.C. Thomson1,2, J.M.R. Gill2, S.R. Gray2, E. Rutherford1,2, J.S. Lees1,2
1Glasgow Renal and Transplant Unit, Queen Elizabeth University Hospital, Glasgow
2ICAMS, BHF Cardiovascular Research Centre, University of Glasgow
Introduction: The increasing prevalence of chronic kidney disease (CKD) is a public health concern. Physical activity (PA) is widely recommended for both primary and secondary prevention of many chronic conditions. It is not clear whether achieving UK Government targets for PA reduces the risk of developing CKD. We examined whether CKD at baseline is associated with degree of PA.
Methods: Participants were from UK Biobank: a prospective cohort study with over 500,000 participants. Estimated glomerular filtration rate was calculated using cystatin C (eGFRcys). CKD was defined according to the KDIGO guidelines (eGFRcys <60 ml/min/1.73 m2 and/or albuminuria > 3 mg/mmol). Type of PA was self-reported using the International Physical Activity Questionnaire (IPAQ) and included none (reference), walking, light or heavy DIY, moderate exercise (cycling, swimming) and participation in strenuous sports. Logistic regression models were used to model the probability of the presence of CKD at baseline across PA categories. Models were adjusted for other known risk factors associated with CKD development, including age, blood pressure and history of or use of medications for cardiometabolic disease.
Results: Of 502,460 participants in UK Biobank, 123,167 were excluded because of missing biochemistry or IPAQ data: 379, 293 participants were included in the analyses, of whom 32,050 (8.4%) had CKD. In participants without CKD, 17,454 (5.0%) reported undertaking no PA and 2948 (0.8%) participated in strenuous sports. For those with CKD, 3402 (10.6%) reported undertaking no PA and 138 (0.4%) participated in strenuous sports. Compared to taking no regular PA, undertaking any PA reduced the risk of baseline CKD (Figure 1: walking, OR 0.6, CI 0.58–0.63; moderate exercise, OR 0.64, CI 0.60–0.67; light DIY, OR 0.84 CI 0.80–0.89; heavy DIY, OR 0.74, CI 0.68–0.80; strenuous sports, OR 0.48, CI 0.40–0.57: p < 0.001).
Conclusion: Self-reported increasing duration and intensity of PA are associated with significantly reduced risk of CKD at baseline, even when adjusted for other recognised risk factors. Benefit is seen with any PA including walking and light DIY. PA is a low risk and cheap intervention which warrants further study to reduce the risk of incident CKD.
Moving more associates with reduced risk of cardiovascular disease and death across all stages of chronic kidney disease: a UK Biobank study
K.I. Stevens1,2, C. Delles2, P.B. Mark1,2, P.C. Thomson1,2, J.M.R. Gill2, S.R. Gray2, E. Rutherford1,2, J.S. Lees1,2
1Glasgow Renal and Transplant Unit, Queen Elizabeth University Hospital, Glasgow
2ICAMS, BHF Cardiovascular Research Centre, University of Glasgow
Introduction: Physical activity (PA) is widely recommended for prevention of chronic conditions including cardiovascular (CV) disease. In chronic kidney disease (CKD), it is unclear whether PA confers similar benefit. We examined whether duration and intensity of PA is associated with risk of CV disease and mortality and whether the relationship differs in CKD.
Methods: Participants were from UK Biobank: a prospective cohort study with over 500,000 participants. Estimated glomerular filtration rate (ml/min/1.73 m2) was calculated using cystatin C (eGFRcys). CKD was defined according to the KDIGO guidelines and participants were categorised as no CKD, CKD G1–2 or CKD G3–5. Exercise duration and intensity was self-reported using the international physical activity questionnaire (IPAQ) and participants categorised into 6 groups, according to PA duration and intensity from sedentary (reference) to extremely active. Cox proportional hazards models tested associations between PA category, mortality and a composite CV end point (myocardial infarction or stroke) across CKD categories, censored for competing risk of all-cause mortality. Models were adjusted for other known risk factors for CV disease and death including age, eGFRcys and albuminuria.
Findings: Of 502,460 participants in UK Biobank, 123,167 were excluded because of missing biochemistry or IPAQ data and a further 21,084 were excluded because of pre-existing cardiovascular disease: 358,209 participants were included in the analyses. PA was reported as sedentary PA in 38,897 (11%) participants; 188,671 (53%) reported extremely active PA levels. Over median follow-up of 11.5 (10.8–12.2) years, 8558 reached the composite CV endpoint and 19,894 died. In 182,457 participants with no CKD, undertaking any PA above sedentary level reduced the risk of the composite CV endpoint and mortality. This was most marked in the extremely active group (HR 0.78, CI 0.69–0.88, p < 0.001, HR 0.74, CI 0.68–0.80, p < 0.001, respectively). In CKD this relationship is maintained; in 162,621 participants with CKD G1–2 and 13,131 participants with CKD G3–5, being extremely active substantially reduced the risk of the CV endpoint (CKD G1–2: HR 0.83, CI 0.76–0.91, p < 0.001; CKD G3–5 HR 0.75, CI 0.61–0.92, p = 0.005) and associates with a survival benefit (CKD G1–2 HR 0.71, CI 0.67–0.75, p < 0.001; CKD G3–5 HR 0.65, CI 0.58–0.72, p < 0.001).
Conclusion: Self-reported increasing duration/intensity of PA are associated with significantly reduced risk of a combined CV endpoint and death. This association is preserved in people with CKD, even when adjusted for other recognised risk factors. Benefit is seen with any PA but is more marked with longer duration/more intense exercise. PA is a simple, low cost intervention which warrants further study to improve CV morbidity and all-cause mortality amongst people with CKD.
Validation of a Vascular Access Specific Quality of Life Measure (VASQoL)
Sabine Richarz1, Sharon Greenwood2, David B Kingsmore1, Peter C Thomson1, Mark Dunlop3, Matt-Mouley Bouamrane4, Ramsay Meiklem3, Karen Stevenson1
1Glasgow Renal & Transplant Unit, Queen Elizabeth University Hospital, Glasgow
2Graduate School, College of Medical, Veterinary & Life Sciences, University of Glasgow, Glasgow, G12 8QQ, Scotland
3Department of Computer and Information Sciences, University of Strathclyde
4Centre for Medical Informatics, Usher Institute of Population Health Sciences and Informatics, University of Edinburgh
Background: A self-administered 11 item Vascular Access Specific Quality of Life Measure (VASQoL) was previously derived from detailed qualitative interviews with adult patients with kidney failure who have experienced vascular access using the Capabilities Approach as a theoretical base1. This study reports the psychometric validation of the VASQoL measure including its reliability, content validity and responsiveness to change.
Methods: Cognitive interviews were conducted with 23 adult patients with kidney failure after completion of the VASQoL measure. Focus group discussion with a vascular access professional multidisciplinary team was undertaken (n = 8) and subsequently a further 101 adult kidney failure patients with vascular access (TCVC, AVF or AVG) completed the digital VASQoL measure, EQ-5D and SF-36 questionnaires in a longitudinal study with prospectively recorded vascular access events.
Results: Transcript analysis of cognitive interviews after VASQoL completion indicated that the content was comprehensive and well understood by participants. Assessment of Internal reliability for the VASQoL measure was high (Cronbach's alpha 0.858). Test-retest reliability of the overall VASQoL measure was high (intra class correlation coefficient 0.916). In those patients who experienced a vascular access event, significant differences were observed in paired analysis of the VASQoL physical domain questions and vascular access function domain questions and in the EQ-5D usual activities, pain and anxiety domains. In those with no vascular access event, variation was observed in longitudinal analysis in VASQoL questions relating to worry about VA function and capability domains, whilst no variation was observed in the EQ5D measure.
Conclusion: The VASQoL measure has good internal consistency, test-retest reliability, convergent validity and responsiveness to change for clinically relevant vascular access outcomes. This provides a validated, vascular access specific quality of life measure that can be used in future trials of vascular access, evaluation of new technologies and routine use as a patient reported outcome measure (PROM).
Michael Sullivan, Bhautesh Jani, Frances Mair, Patrick Mark
University of Glasgow
Background: Major adverse cardiovascular events (MACE) are the leading cause of mortality in chronic kidney disease (CKD). We studied the relationship between the number of long-term conditions and the risk of MACE in patients with CKD.
Methods: We studied patients with CKD in the SAIL Databank: a cohort of 79% of the population of Wales (2011–2018). Patients were categorised by the number of long-term conditions additional to CKD. The outcome was MACE: myocardial infarction, stroke, heart failure hospitalisation. The risk of MACE was estimated via multivariable cox proportional hazards models. Adjustments were made for age, sex, smoking status, deprivation status, baseline eGFR and cholesterol. Subgroup analysis studied the relationship between the number of conditions and MACE in different age groups (18–60 years, 60–80 years and >80 years).
Results: Of the 173,388 patients with CKD, median age was 78 years, 57% were female, 98.6% were of white ethnicity and median eGFR was 51 ml/min/1.73 m2. Compared to patients with CKD only or CKD + 1 condition, there was a graded rise in the risk of MACE by the number of long-term conditions: CKD + 2 conditions adjusted hazard ratio (aHR) 1.22 (95% confidence interval 1.16–1.28), CKD + 3 conditions aHR 1.50 (1.42–1.57), CKD + 4 conditions 1.82 (1.74–1.91), CKD + 5 or more conditions 2.61 (2.50–2.73). Subgroup analysis showed that risk of MACE was particularly elevated in the youngest patients with multiple conditions (Figure 1).
Conclusions: Patients with CKD and multiple health conditions are at high risk of MACE. Multimorbidity is a key risk factor for young patients. Cardiovascular risk stratification in patients with CKD should take into account the number of additional long-term conditions.
Subgroup analysis: risk of major adverse cardiovascular events (MACE) by age group. *Adjusted for age, sex, smoking status, eGFR, cholesterol and deprivation.
Comparing renal replacement therapy (RRT) prevalence between a high-income country (HIC) and a low-to-middle income country (LMIC)
Ashwarya Verma1, Gary Campbell1
1Ninewells Hospital and Medical School, Dundee, UK
Background: End-stage kidney disease (ESKD) is a rapidly increasing global health and health care burden. RRT incidence and prevalence is rapidly increasing in many LMICs whilst it appears to have stabilised in HICs. The aim of this study was to compare the prevalence of RRT between a region in a HIC (NHS Tayside, Scotland) and a region in a LMIC (Gaborone, Botswana) and variations in RRT modality, vascular access patterns and patient co-morbidities.
Methods: We performed a cross-sectional study, including all adult patients ≥ 18 years with established ESKD and on chronic RRT, from the population catchments areas of Gaborone, in Botswana, and NHST in Scotland. In Gaborone, patient and RRT data were obtained from both state and privately-run dialysis units, as well as the main public hospital. Electronic and paper patient records were accessed. Data for NHST patients were obtained from the electronic patient records ‘eMed’ and ‘Clinical Portal’ and the biochemical reporting system, ‘ICE’. All relevant permissions were obtained from the various healthcare settings. Statistical analysis was performed in SPSS v28.
Results: Verma The catchment populations were approx. 230,000 (Gaborone) and 400,000 (NHST), with 342 and 447 chronic RRT patients respectively (p < 0.001). The majority of RRT patients in Gaborone (93.9%) receive dialysis; haemodialysis (HD) or peritoneal dialysis (PD), compared with 42.5% of RRT patients in NHST (p < 0.001). In Gaborone, 77.9% of dialysis patients receive HD whilst 22.1% receive PD. In NHST, 89.5% of dialysis patient receive HD and 10.5% receive PD (p < 0.001). 57.5% of NHST RRT patients have a functioning renal transplant compared with only 6.1% in Gaborone (p < 0.001).
The mean age of patients on HD in Gaborone (49.8, 95% CI 48.1–51.5) is significantly lower than that of HD patients in NHST (64.8, 95% CI 62.7–66.8), (p < 0.001). No significant difference was identified in the gender of HD patients between Gaborone and NHST (33.2% vs 41.8% female, p = 0.074). This was also true for PD patients (31.0% vs 35.0% female, p = 0.734). A higher proportion of female patients in NHST have a functioning renal transplant than in Gaborone (38.7% vs 25.0%, p < 0.001), although numbers in Gaborone were small. Patients on HD in NHST were much more likely to have definitive vascular access, in the form of an arteriovenous fistula (AVF) or graft (AVG) (74.1% vs 32.8%, p < 0.001). There were significant differences in several reported co-morbidities in prevalent HD patients in Gaborone and NHST, including HIV (27.2% vs 0%, p < 0.001), Hepatitis B (4.1% vs 0%, p = 0.005) and hypertension (84.3% vs 51.2%, p < 0.001). There was no difference in the prevalence of diabetes mellitus (29.6% vs 37.1%, p = 0.257). Access to fully publically-funded RRT treatment was 73.6% in Gaborone and 100% in NHST (p < 0.05). An additional 15.6% of RRT patients in Gaborone had access to a mixture of public and private funding.
Conclusions: This study has demonstrated significant variation in RRT modality, vascular access and patient co-morbidities between a region in a HIC (NHST, Scotland) and a region in a LMIC (Gaborone, Botswana). The prevalence of RRT in Gaborone is higher than NHST, at around 1480 vs 1120 pmp. This trend has been recognised globally, in many LMICs, but is unlikely to be representative of all sub-Saharan African countries.
There is significantly less access to renal transplantation for RRT patients in Gaborone, as well as lower rates of definitive vascular access.
A large treatment gap exists between HICs and LMICs in general, which demands a focus on population-based prevention strategies and the development of affordable and cost effective-RRT. The goal is to improve global equity in patient access to all modes of RRT, including renal transplantation.
Scottish Renal Association
Science Abstracts
Siglec-9 engagement attenuates ANCA-mediated neutrophil activation in vitro
Dana Kidder1,4, Kristine Nellany2, Paul Brown3, Moira Davie3, Catriona Walls4
1Renal Unit, Aberdeen Royal Infirmary, Aberdeen.
2Grampian Biorepository, Department of Pathology, Aberdeen Royal Infirmary, Aberdeen
3Department of Pathology, Aberdeen Royal Infirmary, Aberdeen
4Institute of Medical Sciences, University of Aberdeen School of Medicine Medical Sciences and Nutrition, Aberdeen
Background: Sialic acid-binding Ig-like lectin 9 (Siglec-9) is constitutively expressed on neutrophils and monocytes. The expression and potential role of siglec-9 in ANCA-associated vasculitis (AAV) is yet to be determined. We aimed to examine the expression of siglec-9 in patients with AAV and explore the impact of siglec-9 engagement on ANCA-mediated neutrophil responses in vitro.
Methods: Leukocytes and serum were isolated from peripheral venous blood of AAV patients and siglec-9 expression was measured by flow cytometry and ELISA, respectively. Immunohistochemistry was performed on kidney biopsies of AAV patients with AAGN and stained for siglec-9, recombinant siglec-9 Fc chimera and leukocyte markers. Functional studies were done using healthy donor neutrophils in the presence of ANCA and siglec-9 mAb to investigate its role in apoptosis and ROS production.
Results: We found increased serum siglec-9 expression in active AAV compared to remission AAV and a positive correlation with disease activity. Neutrophils and intermediate (CD14 + /CD16 + ) monocytes from PR3-AAV patients displayed higher siglec-9 expression compared to MPO-AAV patients. Siglec-9 expression in AAGN was restricted to areas of active inflammation. Using recombinant siglec-9 Fc chimera protein in immunohistochemistry experiments, we identified glomerular endothelial cells to express siglec-9 ligands. ANCA stimulation of primed neutrophils was associated with siglec-9 shedding. Siglec-9 engagement using anti-siglec-9 mAb was associated with increased neutrophil apoptosis and reduced ROS production compared to isotype control and unstimulated neutrophils.
Conclusion: Siglec-9 expression correlates with disease activity in AAV. Surface of siglec-9 on key cell players in AAV pathogenesis, is biased towards PR3-AAV. The biologic relevance of this finding is unclear. Our in vitro experiments support a potential role for siglec-9 in attenuating ANCA-mediated neutrophil responses. Further evaluation is required to determine the relevance of these findings on neutrophil-endothelial interactions.
Unexpected Positive Flow Crossmatches due to the Presence of HNA-3a Antibodies
Sylvia McConnell1, Richard Battle1, Emma Cannon2, Samina Hussain3, Paul Phelan2, David Turner1.
1Histocompatibility and Immunogenetics Laboratory, SNBTS,
2Transplant Unit, Royal Infirmary of Edinburgh,
3Renal Unit, Ninewells, Dundee.
Recent reports have described renal transplant cases where a positive flow cytometry crossmatch (FC-XM) was observed as a result of human neutrophil antigen (HNA)-3a donor specific antibodies (DSA). HNA-3a/b (found on choline transporter-like protein 2 (CTL2)) is a biallellic polymorphism to which alloantibodies can be formed, most often if a HNA-3b/b individual is exposed to HNA-3a. The HNA-3 antigen may be of relevance in transplantation as it has been shown to be expressed on kidney endothelium. Approximately 95% of the UK population express HNA-3a and a recent review of local female apheresis platelet donors shows ∼1.6% have HNA-3a antibodies.
We report two cases where female recipients with a history of pregnancy received a primary kidney allograft, one from a live donor and the other a deceased donor. Following unexpected positive FC-XMs in both cases, recipients were tested for HLA antibodies by Luminex® and HNA antibodies by various techniques: granulocyte immunofluorescence test (GIFT), granulocyte agglutination test (GAT), lymphocyte immunofluorescence test (LIFT), rHNA-3 cell lines and a Luminex® based assay. Recipients and donors were HNA genotyped by either PCR-SBT or SSP and crossmatched by 3 colour flow cytometry.
Both recipients had HNA-3a antibodies in the absence of HLA-DSA, were genotyped as HNA-3b3b with HNA-3a3a donors and had a T & B cell strong positive FC-XM, with negative autologous FC-XM. Recipient 1 received a live donor transplant on 19/01/18 and was given ATG induction therapy, because of the known presence of the HNA-3a antibody, along with standard maintenance immunosuppression. Biopsy at day 6 showed no rejection and was C4d negative. Serum creatinine on 20/09/21 was 70 µmol/L. Recipient 2 received a kidney from a deceased donor on 01/11/19 and was given Basiliximab induction therapy with standard maintenance immunosuppression. The FC-XM positivity was only identified in this case following a retrospective crossmatch. Biopsy at day 11 was C4d negative but showed moderate microcirculation inflammation and changes suspicious of active antibody-mediated rejection (AMR). Serum creatinine on 06/01/20 was elevated at 198 µmol/L. As of 20/09/21 this recipient has ongoing biopsy proven, HLA-DSA negative AMR with a serum creatinine of 397 µmol/L and has recently been treated with IV methylprednisolone, 5 cycles of plasma exchange and Rituximab.
These results illustrate the mixed picture observed after transplant in the presence of HNA-3a antibodies, as seen in other UK centres. When unexpected strong positive T & B cell FC-XMs are observed in renal patient/donor pairs, consideration should be given to the investigation of HNA-3a antibodies and the use of enhanced induction immunosuppression where feasible.
Single cell analysis of senescent epithelia reveals targetable mechanisms promoting fibrosis
Eoin D O'Sullivan1*, Katie J Mylonas1, Cyril Carvalho1, David P Baird1, Marie Docherty1, Carolynn Cairns2, Kevin M Gallagher3, Alexander Laird3,4, Neil C Henderson1,4, Tamir Chandra4, Kristina Kirschner5,6, Bryan Conway2, Laura Denby2, Gry H. Dihazi7, Michael Zeisberg8, Jeremy Hughes1, Hassan Dihazi7,9§, David A Ferenbach.1§*
1Centre for Inflammation Research, Queen's Medical Research Institute, University of Edinburgh, Edinburgh, UK.
2Centre for Cardiovascular Science, Queen's Medical Research Institute, University of Edinburgh, Edinburgh, UK.
3Department of Urology, Western General Hospital, Edinburgh, UK.
4MRC Human Genetics Unit, Institute of Genetics and Molecular Medicine, University of Edinburgh, Edinburgh, UK.
5The Institute of Cancer Sciences, University of Glasgow, Glasgow, UK
6Cancer Research UK Beatson Institute, Glasgow, UK.
7Institute for Clinical Chemistry/UMG-Laboratories, University Medical Centre Göttingen, Göttingen, Germany
8Clinic for Nephrology and Rheumatology, University Medical Centre Göttingen, Göttingen, Germany
9Center for Biostructural Imaging of Neurodegeneration (BIN), University Medical Center Göttingen, D-37075 Göttingen, Germany.
Effective renal repair following injury is essential for maintaining normal kidney function and is vital to health. Progressive fibrosis and maladaptive organ repair result in significant morbidity and millions of premature deaths annually. Senescent cells accumulate with ageing and after injury and are implicated in organ fibrosis. The elderly and those with chronic kidney disease are most susceptible to disordered repair post injury while also demonstrating the highest burden of senescent cells, suggesting senescent cells may negatively impact renal repair in such patients. However, the mechanisms by which senescence influences repair are poorly understood, and as a result there is an unmet need for both anti-senescent therapies, and new anti-fibrotic therapies to augment post injury renal repair.
Using a clinically relevant murine model of injury and repair we show that obstructive injury generates senescent epithelia which persist after resolution of the original injury, promote ongoing fibrosis and impede adaptive repair. We validate these findings in humans, showing that senescence and fibrosis persist after relieved renal obstruction. We next characterise senescent epithelia in murine renal injury using single cell RNA-Seq. We extend our transcriptomic classification to human kidney and liver disease and identify conserved pro-fibrotic proteins which we validate in vitro and in human disease.
We demonstrate a link between senescent epithelia and fibrosis by showing one of these conserved molecules, Protein Disulfide Isomerase Family A Member 3 (PDIA3), is essential for TGF-beta mediated fibroblast activation. Inhibition of PDIA3 in vivo significantly reduces kidney fibrosis after injury and is a new potential therapeutic pathway. Analysis of the signalling pathways of senescent epithelia connects senescence to organ fibrosis, permitting rational design of anti-fibrotic therapies.