
Abstract
Objective
To examine associations between systemic inflammation, sex hormones, and vitamin D levels in U.S. women.
Methods
A cross-sectional study was conducted using NHANES 2021–2023 data from 3179 women aged 18–80 years. Participants were grouped by high-sensitivity C-reactive protein (hs-CRP) quartiles. Demographic, anthropometric, lifestyle, dietary, and clinical variables were analyzed. Serum biomarkers included hs-CRP, sex hormones, lipid parameters, and 25-hydroxyvitamin D3 (25OHD3). Multivariable linear regression assessed independent associations between hs-CRP and endocrine markers after adjustment for confounders.
Results
Women in the highest hs-CRP quartile had higher age, body weight, waist circumference, body mass index, and prevalence of hypertension and diabetes than those in the lowest quartile. Higher hs-CRP levels were associated with lower concentrations of 17α-hydroxyprogesterone, androstenedione, anti-Müllerian hormone (AMH), dehydroepiandrosterone sulfate, follicle-stimulating hormone (FSH), sex hormone-binding globulin, and 25OHD3. After adjustment, hs-CRP remained positively associated with AMH (β = 0.212, p = 0.007), estrone (β = 0.142, p = 0.048), low-density lipoprotein cholesterol (β = 0.241, p = 0.002), and total cholesterol (β = 0.224, p = 0.001), and inversely associated with FSH (β = −0.194, p = 0.039) and luteinizing hormone (β = −0.191, p = 0.019).
Conclusion
Systemic inflammation was associated with reproductive hormones and lipid profiles, while many associations weakened after adjustment for adiposity. These findings highlight complex links between inflammation, endocrine function, and cardiometabolic health, influenced by obesity-related factors.
Introduction
In both men and women, the immune system serves as the body's primary defense against infections. However, women exhibit a more robust immune response compared to men, which provides better protection against microbial infections. 1 Despite this advantage, women are more prone to autoimmune diseases such as arthritis, multiple sclerosis, and systemic lupus erythematosus. 2 Among women in the USA, elevated levels of inflammation have been reported in specific populations, including pregnant African American women. 3 Inflammation poses a significant threat to health due to its strong association with various chronic disease conditions. 4
Sex hormones play a critical role in modulating both innate and adaptive immune responses. Testosterone exhibits anti-inflammatory properties, while estrogen can exert both pro-inflammatory and anti-inflammatory effects depending on the context. 5 Previous studies have reported that C-reactive protein (CRP) levels may increase during the phases of hormonal fluctuation, including menstruation and periods of declining estrogen levels, although findings have been reported across mixed populations of premenopausal and postmenopausal women. 6 Elevated CRP levels in menopausal women are indicative of increased inflammation, which often coincides with a reduction in estradiol levels. Estradiol has been shown to be negatively correlated with CRP concentrations in postmenopausal women. 7 A decrease in serum sex hormone-binding globulin (SHBG) has also been linked to inflammation, as pro-inflammatory cytokines such as tumor necrosis factor-alpha (TNF-α) and interleukin-1 beta (IL-1β) can suppress SHBG synthesis. 8 Multiple studies have explored the relationship between inflammation, SHBG, and sex hormones. A retrospective cross-sectional analysis reported that SHBG levels were inversely associated with pro-inflammatory markers, while estradiol was positively correlated with inflammation in postmenopausal women. 9 Women with chronic inflammatory conditions tend to have lower plasma concentrations of SHBG. 10 SHBG is thought to provide protective effects against various inflammatory diseases by attenuating inflammation in adipocytes and macrophages. 11 Progesterone also exhibits immunomodulatory and predominantly anti-inflammatory effects by influencing cytokine production and immune cell activity. 12
There is substantial evidence supporting the role of vitamin D in enhancing the balance of anti-inflammatory cytokines. Both in vitro and in vivo studies have shown that vitamin D increases the production of anti-inflammatory cytokines, such as transforming growth factor beta-1 and interleukin-4 (IL-4), while reducing the synthesis of pro-inflammatory cytokines like interleukin-2 (IL-2), interleukin-6 (IL-6), and TNF-α. 13 Vitamin D deficiency has been associated with increased expression of monocyte receptors, thereby promoting inflammation. 14 Additionally, vitamin D levels have been inversely correlated with CRP concentrations in the U.S. population. 15 Meta-analyses have also consistently demonstrated negative associations between vitamin D and CRP levels.16,17
Biologically, chronic inflammation may influence endocrine function through cytokine-mediated effects on the hypothalamic–pituitary–gonadal axis, steroidogenesis, and hepatic synthesis of hormone-binding proteins such as SHBG. Pro-inflammatory cytokines, including TNF-α and IL-6, have been shown to alter hormone production and metabolism, supporting the plausibility that elevated CRP and systemic inflammation may contribute to hormonal dysregulation.18,19
Despite growing interest in the interaction between inflammation and endocrine biomarkers, relatively few studies have simultaneously evaluated high-sensitivity CRP (hs-CRP), sex hormones, and vitamin D in nationally representative samples of U.S. women using recent National Health and Nutrition Examination Survey (NHANES) data. Therefore, this study aimed to investigate the associations between CRP levels, sex hormones, and vitamin D in a representative sample of U.S. women using NHANES 2021–2023 data. We hypothesized that higher CRP levels would be associated with altered sex hormone profiles and lower vitamin D concentrations, reflecting the potential influence of systemic inflammation on endocrine and metabolic regulation.
Methods
Study design and setting
We explored the association between total CRP levels, sex hormones, and vitamin D using data from the NHANES database. This study analyzed data collected between 2021 and 2023, including 3179 participants. NHANES is a comprehensive program designed to assess the health and nutritional status of children and adults across the USA. Each year, it collects information from a nationally representative sample of around 10,000 individuals through interviews and physical examinations. The interviews address topics such as demographics, socioeconomic status, dietary habits, and health conditions, while the physical examinations and laboratory tests, performed by trained professionals, include medical, dental, and physiological evaluations. For this analysis, we focused on a subset of 3179 women aged 18 to 80 years.
Measures
Baseline demographic data included participants’ age, body mass index (BMI), calculated as weight (kg) divided by height squared (m2), body weight (kg), waist circumference (cm), sex, and race/ethnicity, categorized as Hispanic, White, Black, or other. Hypertension status was recorded as either “yes” or “no,” and smoking status was classified as nonsmoker, former smoker, or current smoker. The use of dietary supplements was also documented as “yes” or “no.” Dietary intake, including energy, nutrients, and other food components, was assessed through a 24-h dietary recall, which captured data from midnight to midnight on the day before the interview.
Baseline comorbidities included conditions such as coronary heart disease and physician-diagnosed diabetes, angina pectoris, myocardial infarction, cancer, and stroke, all recorded as “yes” or “no.” Laboratory analyses at baseline involved serum samples collected during medical examinations. These samples were frozen and stored at temperatures below −70 °C until analyzed.
Serum hs-CRP concentrations were measured using a two-reagent immunoturbidimetric assay in NHANES. In this method, serum specimens are first incubated with a Tris buffer, followed by the addition of latex particles coated with mouse anti-human CRP monoclonal antibodies. In the presence of CRP, immune complexes form and increase light scattering proportional to the CRP concentration. The resulting turbidity was measured photometrically at a primary wavelength of 546 nm (secondary wavelength: 800 nm), and hs-CRP concentrations were calculated from a stored calibration curve. Analyses were performed at the University of Minnesota Advanced Research Diagnostics Laboratory using Roche Cobas analyzers. During the 2021–2023 NHANES cycle, laboratory instrumentation transitioned from the Cobas 6000 to the Cobas 8000 analyzer.
Hormone analyses were conducted using isotope dilution liquid chromatography-tandem mass spectrometry (ID-LC-MS/MS). This technique measured levels of 17 α-hydroxyprogesterone, androstenedione, dehydroepiandrosterone sulfate (DHEAS), estrone, estrone sulfate, estradiol, progesterone, and testosterone. The method employed a triple quadrupole mass spectrometer with electrospray ionization in both positive and negative modes. Specific mass-to-charge transitions and chromatographic retention times identified analytes, while isotopically labeled internal standards ensured accurate quantification.
Anti-Müllerian hormone (AMH) levels were measured using an immunoassay that employed antibody interactions and chemiluminescent detection following two incubation steps. Similarly, luteinizing hormone (LH) and follicle-stimulating hormone (FSH) were measured through immunoassays using antibody reactions and chemiluminescence detection with two incubation steps.
SHBG was assessed through a chemiluminescent immunoassay. Magnetic fields were used to capture microparticles on an electrode, and the chemiluminescent reaction was detected via a photomultiplier tube.
Vitamin D analysis followed the Centers for Disease Control and Prevention (CDC's) method to measure 25-hydroxyvitamin D3 (25OHD3), 3-epi-25-hydroxyvitamin D3, and 25-hydroxyvitamin D2 (25OHD2) in human serum using high-performance liquid chromatography-tandem mass spectrometry (HPLC-MS/MS). Separation was achieved with one of the three pentafluorophenyl columns, optimized with a mobile phase of 69–72% methanol in water. Solutions for serum extraction, reconstitution, and needle washing were matched to the mobile phase composition to ensure consistency. 20
Statistical methods
Participants were divided into four groups according to their CRP levels. Differences in general characteristics among these groups were analyzed using one-way analysis of variance for continuous variables and chi-square tests for categorical variables. To investigate the association between CRP levels, hormone parameters, and vitamin D, multivariate linear regression analysis was performed, adjusting for potential confounders. All statistical analyses were conducted using SPSS software (version 25), with a p-value below 0.05 considered statistically significant.
Results
Participant characteristics
Table 1 outlines the demographic and biochemical profiles of participants categorized by total CRP quartiles (3179 women). Among those in the highest quartile, the majority (62.3%) were non-Hispanic White. This group exhibited a higher average age (54.75 ± 17.27 years) compared to the lowest quartile (47.95 ± 19.30 years). Participants in the highest CRP quartile also showed greater mean body weight (91.05 ± 23.76 kg) and waist circumference (109.11 ± 16.46 cm) compared to those in the lowest quartile (62.77 ± 11.69 kg and 84.22 ± 11.92 cm, respectively).
Characteristics of NHANES participants across quartiles of serum high-sensitivity C-reactive protein (hs-CRP) levels.
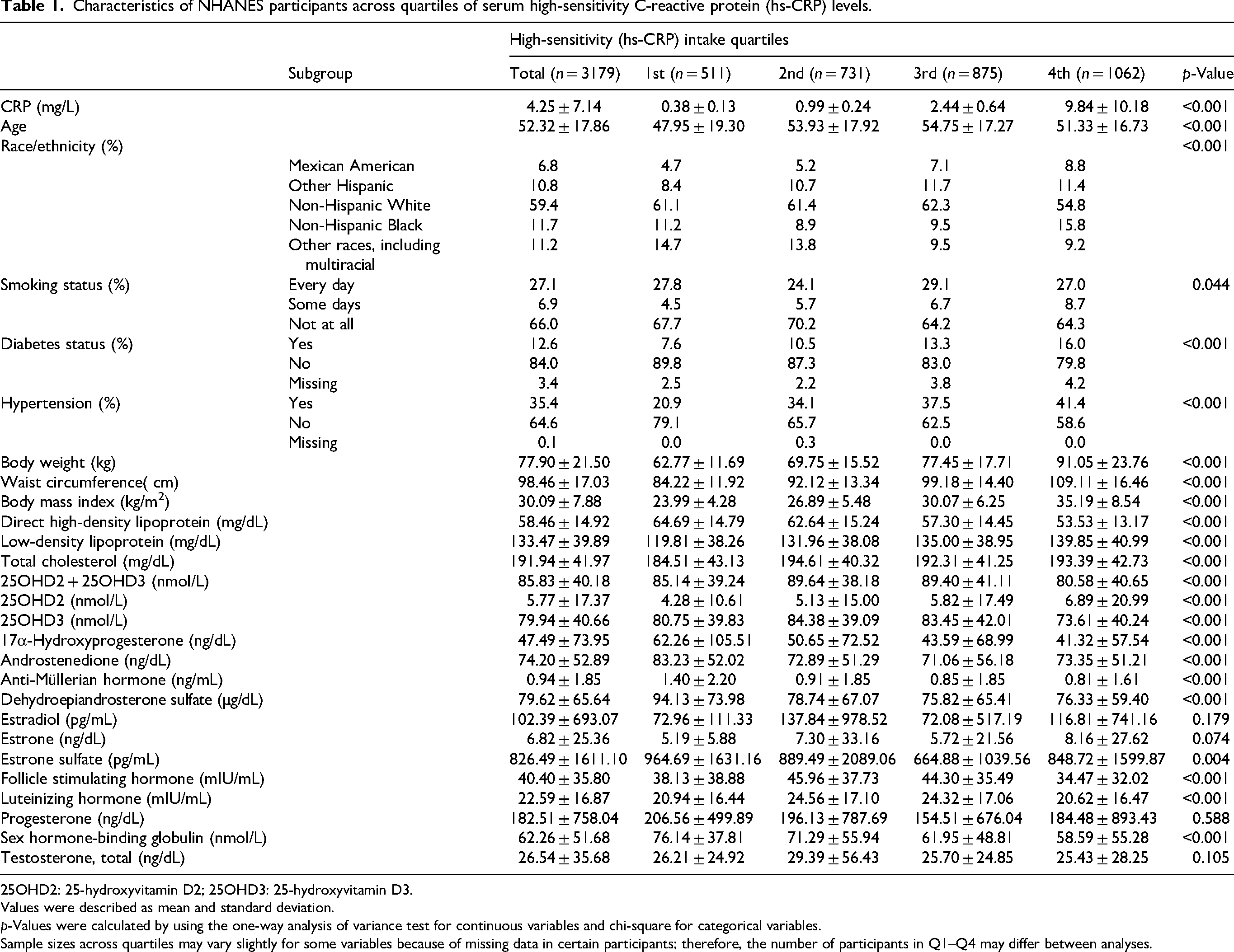
25OHD2: 25-hydroxyvitamin D2; 25OHD3: 25-hydroxyvitamin D3.
Values were described as mean and standard deviation.
p-Values were calculated by using the one-way analysis of variance test for continuous variables and chi-square for categorical variables.
Sample sizes across quartiles may vary slightly for some variables because of missing data in certain participants; therefore, the number of participants in Q1–Q4 may differ between analyses.
Biochemical measures varied significantly between quartiles. High-density lipoprotein (HDL) levels were lower in the highest CRP group (53.53 ± 13.17 mg/dL) compared to the lowest group (64.69 ± 14.79 mg/dL). Conversely, low-density lipoprotein (LDL) levels were elevated in the highest CRP quartile (139.85 ± 40.99 mg/dL) relative to the lowest quartile (119.81 ± 38.26 mg/dL). Total cholesterol was also higher in the highest quartile (184.51 ± 43.13 mg/dL) compared to the lowest (119.81 ± 38.26 mg/dL). Similarly, BMI was significantly greater in the highest CRP quartile (35.19 ± 8.54 kg/m2) compared to the lowest (23.99 ± 4.28 kg/m2).
Hormonal parameters
Several hormonal parameters exhibited significant differences across CRP quartiles. Participants in the highest quartile had lower levels of 17α-hydroxyprogesterone (41.32 ± 57.54 vs. 62.26 ± 105.51 ng/dL), androstenedione (73.35 ± 51.21 vs. 83.23 ± 52.02 ng/dL), AMH (0.81 ± 1.61 vs. 1.40 ± 2.20 ng/mL), FSH (34.47 ± 32.02 vs. 38.13 ± 38.88 mIU/mL), DHEAS (76.33 ± 59.40 vs. 94.13 ± 73.98 µg/dL), and SHBG (58.59 ± 55.28 vs. 76.14 ± 37.81 nmol/L). Estrone sulfate levels were also lower in the highest CRP quartile (848.72 ± 1599.87 vs. 964.69 ± 1631.16 pg/mL).
In contrast, estrone (8.16 ± 27.62 vs. 5.19 ± 5.88 ng/dL) and LH levels (24.32 ± 17.06 vs. 20.94 ± 16.44 mIU/mL) were higher in the highest CRP quartile. Total testosterone levels were similar between groups, showing no significant difference.
Dietary intake
Table 2 presents nutrient and energy intake by CRP quartiles. Participants in the highest quartile reported higher intakes of energy, protein, carbohydrates, fats, dietary fiber, total sugars, saturated fatty acids, monounsaturated fatty acids, polyunsaturated fatty acids, cholesterol, vitamin D, vitamin E, and vitamin C. However, most of these differences were not statistically significant. Significant trends were observed for dietary fiber (p < 0.001), monounsaturated fatty acids (p = 0.031), polyunsaturated fatty acids (p = 0.008), vitamin E (p < 0.001), vitamin C (p < 0.001), and vitamin D (p = 0.007), all of which were higher in the highest CRP group compared to the lowest.
Dietary intake of NHANES participants across quartiles of serum high-sensitivity C-reactive protein (hs-CRP) levels.
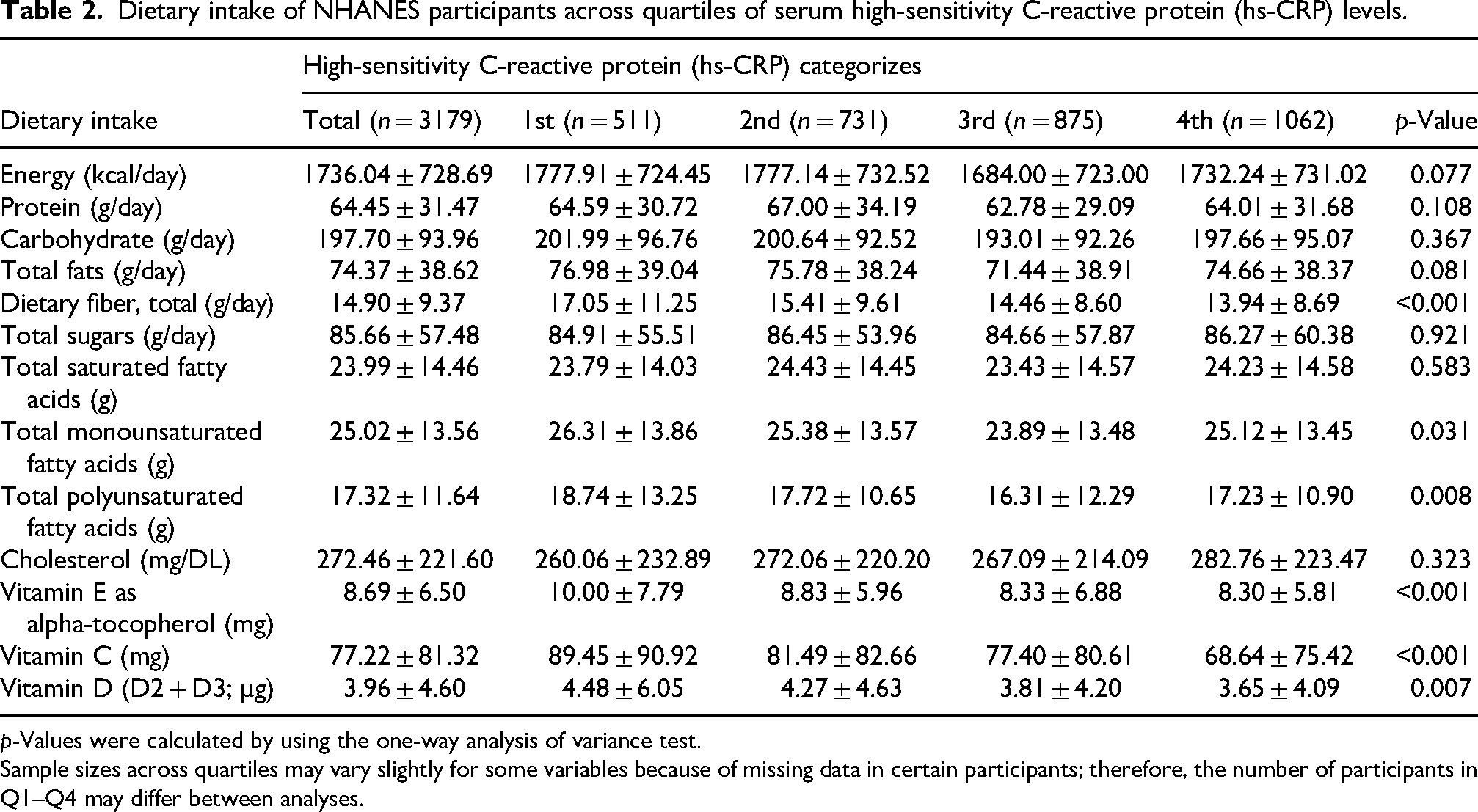
p-Values were calculated by using the one-way analysis of variance test.
Sample sizes across quartiles may vary slightly for some variables because of missing data in certain participants; therefore, the number of participants in Q1–Q4 may differ between analyses.
Regression analysis
Table 3 presents the multiple linear regression analysis evaluating the associations between serum hs-CRP and sex hormone variables as well as vitamin D markers after adjustment for demographic, lifestyle, dietary, and clinical covariates. Among the examined variables, anti-AMH showed a significant positive association with hs-CRP levels (β = 0.212, p = 0.007), indicating that higher AMH concentrations were associated with increased systemic inflammation. Estrone was also positively associated with hs-CRP (β = 0.142, p = 0.048). In contrast, FSH (β = −0.194, p = 0.039) and LH (β = −0.191, p = 0.019) demonstrated significant inverse associations with hs-CRP, suggesting lower inflammatory status with higher gonadotropin levels.
Multiple linear regression analysis showing the association of serum high-sensitivity C-reactive protein (hs-CRP) with sex hormone variables and vitamin D.

25OHD2: 25-hydroxyvitamin D2; 25OHD3: 25-hydroxyvitamin D3.
Data of each variable was adjusted for age, race/ethnicity, educational level, body mass index, waist circumference, alcohol intake, smoking status, physical activity, energy intake, protein intake, fat intake, carbohydrate intake, total sugar intake, fiber intake, diabetes status, retinol (µg), total polyunsaturated fatty acids (g), lycopene (µg), country of birth, history of hypertension, vitamin C (mg), cholesterol (mg), riboflavin (vitamin B2; mg), selenium (µg), vitamin E as alpha-tocopherol (mg), vitamin A (RAE, µg), calcium (mg), total saturated fatty acids (g), dietary fiber (g), protein (g), total monounsaturated fatty acids (g), carbohydrate (g), energy (kcal), and total fat (g).
Regarding vitamin D parameters, 25OHD3 showed a borderline positive association with hs-CRP (p = 0.050), whereas total vitamin D (25OHD2 + 25OHD3) and 25OHD2 were not significantly associated with hs-CRP. Lipid markers, including LDL cholesterol (β = 0.241, p = 0.002) and total cholesterol (β = 0.224, p = 0.001), were positively associated with hs-CRP levels. No statistically significant associations were observed for 17α-hydroxyprogesterone, androstenedione, DHEAS, estradiol, estrone sulfate, progesterone, SHBG, total testosterone, or direct HDL.
Discussion
Main findings
In this cross-sectional study of 3179 U.S. women from NHANES 2021–2023, several hormonal and metabolic parameters differed across serum hs-CRP quartiles. Women in the highest hs-CRP quartile had higher age, body weight, waist circumference, BMI, diabetes prevalence, and hypertension prevalence compared with women in the lowest quartile. Significant differences across hs-CRP quartiles were also observed for several endocrine markers, including lower concentrations of 17α-hydroxyprogesterone, androstenedione, AMH, DHEAS, FSH, SHBG, and 25OHD3.
However, after multivariable adjustment for demographic, lifestyle, dietary, anthropometric, and clinical covariates, only a limited number of endocrine markers remained independently associated with hs-CRP. Specifically, hs-CRP was positively associated with AMH and estrone, while inverse associations were observed with FSH and LH. No independent associations were identified between hs-CRP and estradiol, SHBG, testosterone, progesterone, DHEAS, total vitamin D, or 25OHD2. These findings suggest that many apparent relationships between inflammation and endocrine biomarkers may be substantially influenced by adiposity, metabolic status, and lifestyle-related confounding factors. In addition, LDL cholesterol and total cholesterol remained positively associated with hs-CRP after multivariable adjustment, indicating a persistent relationship between systemic inflammation and adverse lipid profiles.
Interpretation of findings
Previous studies have reported associations between inflammation and reproductive hormones in women, particularly involving SHBG, estradiol, and androgen metabolism.9,21 However, many of these associations appear to weaken after adjustment for obesity-related and metabolic variables. In the present study, SHBG concentrations differed significantly across hs-CRP quartiles in unadjusted analyses, but this association was no longer statistically significant after multivariable adjustment. This finding suggests that the relationship between SHBG and inflammation may be partially mediated by adiposity, insulin resistance, or other metabolic factors rather than reflecting an independent inflammatory effect. 22 Experimental studies have demonstrated that inflammatory cytokines such as TNF-α and IL-6 may suppress hepatic SHBG synthesis and influence steroid hormone metabolism. 23 Nevertheless, caution is warranted when extrapolating mechanistic findings from in vitro studies to population-based observational data. Our results indicate that the observed associations between hs-CRP and SHBG in crude analyses may largely reflect shared metabolic determinants.
We also observed significant inverse associations between hs-CRP and both FSH and LH after multivariable adjustment. Chronic low-grade inflammation may influence hypothalamic–pituitary–gonadal axis regulation through cytokine-mediated mechanisms affecting gonadotropin secretion.24,25 However, interpretation should remain cautious because menopausal status, menstrual cycle phase, hormone therapy use, and reproductive conditions such as polycystic ovary syndrome were not available or could not be fully accounted for in the present analysis.
Interestingly, AMH and estrone demonstrated positive independent associations with hs-CRP. The biological significance of these findings remains uncertain and may reflect residual confounding or differences in ovarian aging, adiposity, or peripheral estrogen metabolism. Estrone is produced predominantly through peripheral aromatization in adipose tissue, 26 which may partially explain its positive association with inflammatory status in women with higher BMI.
Although significant differences in vitamin D measures were observed across hs-CRP quartiles, multivariable regression analyses did not demonstrate statistically significant independent associations between hs-CRP and total vitamin D or 25OHD2 concentrations. The borderline association observed for 25OHD3 should therefore be interpreted cautiously. Prior epidemiological studies and meta-analyses have suggested inverse associations between vitamin D status and inflammatory markers27,28; however, the present cross-sectional study cannot determine causality or directionality. Furthermore, the divergent findings between 25OHD2 and 25OHD3 remain uncertain and may reflect differences in dietary intake, supplementation patterns, metabolism, or residual confounding.
The present study also demonstrated significant positive associations between hs-CRP, LDL cholesterol, and total cholesterol after adjustment for multiple confounding factors. These findings are consistent with previous evidence linking chronic low-grade inflammation to adverse cardiometabolic risk profiles.29,30 Inflammatory pathways may contribute to altered lipid metabolism through cytokine-mediated effects on hepatic lipid synthesis and transport. 31 Conversely, dyslipidemia itself may promote inflammatory activation, suggesting a bidirectional relationship between metabolic dysfunction and systemic inflammation. 32 The persistence of these associations after extensive adjustment highlights the close interrelationship between inflammation, obesity, and cardiovascular risk factors in women.
Participants with higher hs-CRP levels also had substantially higher BMI and waist circumference, supporting previous evidence linking adiposity with chronic low-grade inflammation. 33 Adipose tissue is metabolically active and contributes to inflammatory cytokine production, which may influence both CRP concentrations and endocrine function. 34 The attenuation of several hormone associations after adjustment for BMI and metabolic variables further highlights the importance of obesity-related confounding in studies examining inflammation and hormonal status.
Dietary differences across hs-CRP quartiles were also observed, particularly for dietary fiber and selected fatty acids. Women with higher hs-CRP levels reported lower fiber intake, consistent with previous evidence suggesting anti-inflammatory effects of higher dietary fiber consumption. 35 However, dietary intake variables were included as covariates rather than primary exposures in the present study, and these findings should therefore be interpreted descriptively.
Clinical implications
First, the strong relationships observed between hs-CRP, obesity-related measures, and adverse lipid profiles reinforce the importance of systemic inflammation as a marker of underlying cardiometabolic risk in women. Elevated hs-CRP concentrations in clinical practice may therefore prompt more comprehensive evaluation of obesity, central adiposity, dyslipidemia, hypertension, and metabolic health rather than the isolated assessment of reproductive hormones alone.
Second, although several endocrine biomarkers differed across hs-CRP quartiles, most associations were attenuated after adjustment for adiposity and metabolic factors. This suggests that clinicians should interpret alterations in reproductive hormone profiles within the broader context of metabolic health and chronic low-grade inflammation. The findings indicate that obesity and metabolic dysfunction may substantially contribute to hormonal variation previously attributed directly to inflammation.
Third, the persistent associations between hs-CRP and lipid parameters support the potential value of inflammatory markers in identifying women at increased cardiometabolic risk. Women with elevated hs-CRP may benefit from earlier lifestyle-focused interventions targeting weight management, dietary quality, physical activity, and cardiovascular risk reduction. In particular, the observed relationship between central obesity and inflammation highlights the importance of waist circumference and BMI assessment during routine women's health screening.
Fourth, although vitamin D measures were not consistently independently associated with hs-CRP after adjustment, the observed differences across inflammatory categories suggest that vitamin D status may still reflect broader metabolic and lifestyle-related health patterns. Routine evaluation of vitamin D deficiency may therefore remain clinically relevant in women with obesity or elevated inflammatory burden.
Fifth, importantly, because of the cross-sectional design, these findings should not be interpreted as evidence that inflammation directly causes hormonal abnormalities or that hs-CRP should currently be used as a standalone endocrine screening tool. Rather, the results support an integrated clinical approach in which inflammatory, metabolic, and hormonal factors are evaluated together when assessing women's overall health risk. Longitudinal studies are needed to determine whether reducing systemic inflammation can improve endocrine and cardiometabolic outcomes in women.
Strengths and limitations
This study utilized data from a large, nationally representative sample of U.S. women and incorporated extensive adjustment for demographic, anthropometric, lifestyle, dietary, and clinical confounders. Additionally, hormone and vitamin D measurements were performed using standardized laboratory methods.
Nonetheless, there are several limitations that need to be pinpointed. First, the cross-sectional design precludes conclusions regarding causality or temporal relationships, and reverse causation remains possible. Second, hs-CRP is a nonspecific inflammatory marker that may be elevated due to obesity, infection, smoking, autoimmune disease, malignancy, diabetes, cardiovascular disease, or other acute and chronic conditions. Some participants may have had markedly elevated hs-CRP levels suggestive of acute inflammatory conditions. The underlying causes of elevated hs-CRP were not directly evaluated, and additional inflammatory biomarkers such as IL-6, TNF-α, fibrinogen, leukocyte count, or neutrophil-to-lymphocyte ratio were not available for a comprehensive assessment of systemic inflammation. Third, reproductive factors, including menopausal status, menstrual cycle phase, pregnancy status, oral contraceptive use, hormone replacement therapy, hysterectomy/oophorectomy status, and polycystic ovary syndrome, could not be fully adjusted for and may have influenced hormone concentrations. Fourth, hormone and vitamin D levels were measured at a single time point and may not reflect long-term hormonal status or physiological fluctuations. Fifth, dietary intake was assessed using 24-h dietary recall, which is subject to recall bias and measurement error. Finally, residual confounding from unmeasured variables, including medication use and undiagnosed inflammatory conditions, cannot be excluded.
Conclusion
In this cross-sectional analysis of U.S. women participating in NHANES 2021–2023, several hormones, vitamin D, and metabolic differences were observed across hs-CRP quartiles. However, after adjustment for demographic, lifestyle, dietary, anthropometric, and clinical confounders, only AMH, estrone, FSH, LH, LDL cholesterol, and total cholesterol remained independently associated with hs-CRP. No significant independent associations were identified for estradiol, SHBG, testosterone, progesterone, or most vitamin D measures. These findings suggest that many previously reported associations between inflammation and endocrine biomarkers may be substantially influenced by adiposity and metabolic confounding factors. The persistent associations between hs-CRP and lipid markers further support the close relationship between systemic inflammation and cardiometabolic health in women. Prospective studies are needed to clarify the causal relationships between inflammation, endocrine function, vitamin D status, and lipid metabolism.
Footnotes
Ethical considerations
Ethics approval not required as this research does not involve direct patient or animal contact.
Author contributions
AA-Z, OA, and IAA-B contributed to study conception, data collection, data analysis, study supervision, and manuscript writing. SB, HMA, SAKS, SOA, HA, SMSA, MZJ, SA, MA, and AZ contributed to literature review, investigation, data validation, data interpretation, and revision of the manuscript for editorial and intellectual contents. All authors read and approved the final draft of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of data and material
Guarantor
Ahmed Abu-Zaid.