
Abstract
Disabled people are exposed to a higher incidence of violence compared to the population average. Consequently, they are often described as ‘vulnerable’. This article argues that this concept focuses explanations for violence on the person at risk. It therefore redirects attention towards the social forces that make violence more likely to occur. With reference to case studies, a micro-analysis outlines how subtle forms of oppression, including imbalanced personal relationships, social exclusion, restricted autonomy and a higher tolerance for maltreatment within segregated settings, affect the daily experiences of disabled people. This is followed by a macro-analysis, which exposes further structural inequalities and a societal ratification of hostility towards disabled people. These processes are described as forming a continuum, which highlights that boundaries between mundane experiences and contact violence are at times blurred and shifting.
Keywords
Introduction
We urge all social scientists to think about the power they have to construct [concepts of violence]. We urge them to consider who benefits, who loses, and what is implied through the questions they choose to ask and the way they define terms. (Muehlenhard and Kimes, 1999: 243)
Muehlenhard and Kimes (1999: 234) assert that ‘what counts as violence is socially constructed, has varied over time, and reflects power relationships’. Moreover, ‘definitions of terms depend on who gets to define them; thus, definitions reflect the interests of people with power’. In this article, the author seeks to utilise her power to influence the social construction of oppression and violence by suggesting a broad definition.
Disabled people consistently report higher incidences of intimate violence compared to the population average (Smith et al., 2011). There is furthermore an increasing awareness of disablist hate crimes. This term refers to targeted crimes, ranging from verbal abuse through to bodily harm, torture and murder (Quarmby, 2008). This article highlights how oppressive social systems and processes facilitate conditions within which violence is more likely to occur. The discussion will initially engage with case studies from a sample of adults who are labelled with learning difficulties. This micro-analysis highlights how invasive, restrictive and harmful processes impact on their daily lives. This is followed by a macro-analysis, which demonstrates how social structures facilitate oppression, intrusion and violence.
Key Concepts: Vulnerability, Disability and Violence
In everyday discourse, disabled people are often described as ‘vulnerable’. For example, this term is routinely used by the popular media (e.g. Dampbell and Bawden, 2012), policy makers and professionals. The most commonly used definition amongst this group describes a ‘vulnerable adult’ as someone who:
… is or may be in need of community care services by reason of mental or other disability, age or illness; and who is or may be unable to take care of him or herself, or unable to protect him or herself against significant harm or exploitation. (Lord Chancellor’s Department, 1997: 68)
This definition assumes a direct relationship between impairment, age or illness and risk. However, this is not always helpful. If a person is seen to be ‘vulnerable’ because of who they are, then nothing can be done but to protect that defenceless person (Hingsburger, 1995). Yet, having to rely on protection by others increases dependency on support workers and family carers, which can make these relationships more easily exploitable.
Furthermore, explanations for increased risk of violence should not focus on the individual. Feminists have put it bluntly: Women are not raped because they are women. They are raped because of men’s attitudes, men treating women as property and relationships based on power (Kelly, 1988). Similarly, disabled people are not violated because they are disabled, but because those who are perceived as different have less power, they are marginalised and targeted. Focusing on individual ‘vulnerability’ (for example the fact that someone is disabled, female, young or old) does not enable us to understand how social conditions make violence more likely to occur. This article therefore adopts a social model approach, which invites us to focus on social, rather than individual factors.
The social model makes a distinction between disability and impairment. Whilst impairment is a personal characteristic, disability is a social condition, which is imposed on a person on top of their impairment:
Impairment is a characteristic of the mind, body or senses within an individual which is long term and may, or may not, be the result of disease, genetics or injury. Disability is the disadvantage or restriction of activity caused by the political, economic and cultural norms of a society which takes no or little account of people who have impairments and thus excludes them from mainstream activity. (Oliver et al., 2012: 16)
There is a direct link between violence and disability, as impairments may be caused by physical and psycho-emotional injuries. Nonetheless, in such situations the political connotations of the social model have the potential to facilitate the victim’s transition to a more positive (survivor) identity: ‘The importance of this social model of disability is that it no longer sees disabled people as having something wrong with them – it rejects the individual pathology model’ (Oliver, 1983: 27).
Finally, this discussion should operationalise the term ‘violence’. However, as the following debate indicates, it is perhaps not possible, nor desirable, to settle on a clear-cut definition at this stage. Kelly (1988) suggests that sexual violence occurs on a continuum. This includes any unsought or unwanted contact and non-contact sexual experiences, including sexual harassment, sexual assault, pressurised and coercive sexual intercourse and rape. She asserts that this continuum can highlight how men routinely control women. The threat of rape and the fact that it happens to some women create a climate of fear. According to Kelly (1988), all men benefit from this and thus benefit from the fact that some men rape women. Contact violence is used only when other methods of control have failed.
However, it has been argued that such a broad use of ‘violence’ is inappropriate and that the term should be reserved for physical coercions or their threat (Jacobs et al., 2000). As ‘violence’ continues to be strongly associated with physical acts, some feminists have suggested that the term ‘abuse’ offers the breadth required to take account of the emotional and psychological impact of maltreatment in the domestic sphere. This, they argue, is often more pervasive and long term than physical injuries. Thus, ‘abuse can still be occurring even when there is no evidence of physical harm’ (Tapley, 2010: 142).
The result of such debates is an inconsistent use of terminology, which reflects the diversity of definitions in use. For instance, the Women’s Aid (2012) website appears to use the terms ‘violence’ and ‘abuse’ almost interchangeably. The Scottish Women’s Aid (2012) website, on the other hand, acknowledges colloquial interchangeable use, but it then adopts ‘abuse’ consistently throughout, in line with the definitions and terminology used by Scotland’s strategy for Preventing Domestic Abuse (Scottish Executive, 2003). Yet, UK central government publications continue to use the term ‘domestic violence’ (e.g. HMSO, 2010). In late 2011, the public was invited to a consultation on the definition of ‘domestic violence’ (Home Office, 2011), but changing terminology from ‘violence’ to ‘abuse’ was not one of the points under consideration.
It can be concluded that researchers, policy makers and activists are doing exactly what Muehlenhard and Kimes urged (1999) us to do, as we are considering what the consequences of our definitions may be. Settling on one approach would mean losing the benefits offered by all the others. The resulting variety may look confusing to those who seek simplistic and fixed definitions and terminology. Yet, ongoing public debates can take account of the fact that what counts as violence is socially constructed and arises from particular historical and cultural understandings.
Whilst feminists have spent recent decades exploring and redefining what constitutes ‘abuse’ and ‘violence’, there have been limited explorations in disability studies. In UK policy guidance, the term ‘abuse’ continues to be widely and mostly uncritically applied (e.g. Department of Health, 2010). This article seeks to demonstrate how the notion of ‘oppression and violence on a continuum’, modelled on Kelly’s (1988) approach, can offer an alternative explanation.
Methodology
The findings presented in this article arose from a research project, which explored to what extent risk of sexual violence against adults with learning difficulties is shaped by social processes (Hollomotz, 2011). The study aimed towards a participatory methodology (Zarb, 1992). Such research differs from traditional approaches, as it seeks to be accountable to disabled people, who have some control over the research process. A group of 15 self-advocates (8 women and 7 men) with the label of learning difficulties who met weekly at an independent self-advocacy agency were involved as research advisors during the design and analysis stage. Amongst others, they helped to develop accessible research tools and to determine the focus of the analysis and to interpret the data (for more information, see Hollomotz, 2011).
Self-advocacy can be defined as a very specific and individual act: ‘A person assumed to have no voice, or nothing to say, speaks; and so challenges the identity they have been assigned’ (Dowson, 1990: 6). Self-advocates stand up for their rights, make choices and strive towards independence (People First Workers, 1996). In short, self-advocacy is a practice that contests oppression (Dowse, 2001).
Semi-structured interviews were conducted with 12 men and 17 women with learning difficulties. The research advisors helped to ensure that the interviewing schedule did not include complex grammatical structures or concepts (Finlay and Lyons, 2001). Instead, short sentences and simple words were used. The group was also involved in developing three picture story vignettes, which were used to discuss risk. In addition, 36 picture cards accompanied the 23 question categories. These provided further concrete prompts, to facilitate the communication needs of less articulate respondents. For further information on the research design, see Hollomotz (2011).
All of the participants were White British with the exception of one respondent, whose ethnicity was Pakistani. Respondents were between 22 and 68 years old. About half had additional impairment labels, such as physical impairments, epilepsy and ‘Autistic spectrum’ labels. About half lived with their parents or other family carers. About a quarter lived in residential group settings and another quarter lived on their own or with a partner. These figures are roughly representative of the accommodation arrangements for this population (Emerson and Hatton, 2008). Table 1 presents an overview of some personal attributes of those who are cited in this article.
The respondents.

Note: All names used throughout this article are pseudonyms. M = male, F = female. Living arrangement: 1 = independent, 2 = independent with support (not 24/7), 3 = living with family or parents, 4 = 24/7 staffed.
Potential participants were accessed at two statutory and one private day service and two advocacy organisations. Participant observations here furthermore enabled the researcher to familiarise herself with individuals’ communication needs and with part of their daily routine. The research gave rise to a number of specific ethical concerns, because it involved talking to participants with learning difficulties about sensitive issues. These have been addressed in line with the British Sociological Association’s (2002) requirements for ethical practice. Ethical approval has been granted by a local authority ethics committee.
The interviews were recorded and partially transcribed. The data were then processed and analysed with the assistance of NVivo8, using thematic analysis. The research advisors engaged in a range of focus group discussions. Together, we made sense of and analysed the data. Themes that emerged from the overall study included experiences of sex, sexuality and personal relationships, disability and identity, discussions about minor and major choices, oppression and violence. This article draws on some of these themes, with a particular focus on invasive processes. It therefore focuses on problematic accounts, whilst respondents also reported many positive experiences. For further examples, see Hollomotz (2011).
The following three sections present a micro-analysis, which draws on the accounts of respondents, who describe how a range of practices act to permit oppression and violence. In the first section, the focus is on labelling effects, segregation and restrictions to choices. Next, power imbalances within social relationships are considered. The third section explores hostility, exploitation and contact violence. The fourth section adds a macro-analysis of historical, political and further structural contexts. Finally, the ensuing discussion draws all of these processes together by describing them as forming a continuum.
Becoming ‘Disabled’
In Great Britain, 29 per cent of adults aged 16 and over have at least one impairment (Vine et al., 2011). However, there is a difference between having an impairment and having the condition of disability imposed on top of the impairment. Emma’s case demonstrates this well. She was impaired all her life, but she only became disabled when she was labelled in her early 30s and when services began to ‘help’. Previously, she had been living independently with a partner and their two children. Nowadays Emma, who lost custody of her children to their non-disabled father, lives in a residential group setting. Her care plan states that she needs support with many tasks she had managed independently before, such as shopping. Emma states:
It upsets me cause I want to be like a normal, normal person […] without having a carer or help […]. I just wanna do it myself. […] I’m still doing the same things as before, but ehm… now I’m having help with it and I just … it … I just don’t like. I, I don’t like it cause it upset, like, cause, people are helping me and I wanna do it myself.
Britney used to live in her own flat with some formal support. Four years ago, a group of ‘friends’ threatened to harm her in a dispute over her reluctance to engage in illegal activities. Amongst others, they wanted to store stolen goods in her flat and they attempted to engage Britney in their activities. Individuals in semi-sheltered accommodation are at greater risk of exploitation from people in their local community than those living in 24-hour staffed residential services (Emerson et al., 2001). This is precisely why Britney was moved to a more controlled environment. She now lives in a large institutional complex and shares a unit with 14 residents, all of whom are at least 20, some 40, years her senior.
Britney believes that her current residential setting is not meeting her needs: ‘It’s not the right place for me. I’m too independent and it’s the wrong age limit. They don’t do fun stuff like we [young people] do.’ Although she believes that her quality of life has decreased, Britney is now better protected from risks arising from community inclusion. Paradoxically, new risks of institutional abuse arise (Stanley et al., 1999). This poses questions about the effectiveness of the intervention. One effect is clear: this intervention is contrary to the Valuing People (Department of Health, 2001) policy framework that should have affected practice at the time, which is underpinned by the principle that the rights, choices and independence of people with learning difficulties must be promoted.
Lack of control in everyday life affected many respondents. This study explored the following opportunities for minor and major choice: food and clothes, daytime activities, living arrangements and social and sexual relationships. It exposed restrictions in all of these areas. A practice of presenting individuals with pre-agreed options, rather than opportunities to exercise autonomy through genuine, free choice was exposed (Hollomotz, in press).
For instance, respondents who attended day services generally had some level of control when determining which activity groups they attended. Nonetheless, a significant minority, five of 22 respondents, perceived that they could not make meaningful selections. Moreover, attendance at the service meant that during this time an infinite range of alternative options, such as employment, alternative leisure opportunities or staying at home became unavailable. The options on offer were restricted and pre-agreed by staff, who remained in control, while an individual’s selections between activities were merely tokenistic.
Respondents were aware of boundaries beyond which they could not exercise control and some articulated compliance. For instance, when explaining why he would not buy an item of clothing that the support worker who accompanies him to the high street does not approve of, Ryan asserts: ‘I’ve always tried pleasing people in my life, cause that’s with my difficulty, that’s what I’ve always thought I’ve had to do’. Ryan’s readiness to please may be easily exploited. The next section highlights further how social relationships of disabled people are at times characterised by power imbalances.
Imbalanced Social Relationships
Friendships can present an opportunity to pursue equal social relations. They are typically voluntary and involve intimacy (e.g. Fehr, 1996). Mary asserts that friends can rely on each other when ‘anything happens’. For example, she states that a friend called her immediately after she had broken her leg. Mary supported her emotionally and also helped her to complete some practical tasks. However, only about a third of the respondents (eight of 29) had such informal contact with their friends. Those who did had comparatively low support needs. In other words, people who relied on assistance that would enable them to socialise informally were much less likely to do so. Nevertheless, with one exception, all of the respondents asserted they had friends.
The above may explain why young disabled people have been reported to become less socially active and more isolated after leaving school, while the opposite is the case for their able-bodied peers (Stevens, 1996). Similar to an example cited by Chappell (1994), none of the 14 respondents who attended council run day services socialised with their friends outside the service. Such relationships are therefore extremely vulnerable to break-up. For example, Rose states that one of her friends attends a different day service venue since the facility was reorganised. They have not had any contact since.
For all of the above reasons, disabled people often rely on relationships with family carers and support workers to fulfil some of their social and emotional needs. Many report that they view their assistants as companions (Yamaki and Yamazaki, 2004). Yet, such relationships are by their very nature less balanced than friendships. For instance, the support worker may know a wealth of intimate information about the individual they support, but they generally do not reciprocate this trust by confiding their personal issues. Moreover, support staff tend to have social contacts outside their work environment, while the service user may have limited social intercourse and depend on this relationship. This amplified socio-emotional dependence puts vast responsibilities and power into the hands of the support worker. To illustrate this imbalance, the following accounts demonstrate how support workers’ authority determines whether a person’s concerns about intrusive experiences are addressed.
Gemma told me that she was unhappy about attending one of her weekly activity groups at the day centre, because a woman in the group kept verbally harassing her. We spoke to Gemma’s key worker. However, the key worker was already aware of these issues. She could not be persuaded to change Gemma’s group or indeed to talk to the woman who was upsetting her. Instead, she advised Gemma that she should ‘simply ignore’ the woman. When Gemma turned her back to us, the key worker rolled her eyes at me. Later on, she described Gemma as a ‘drama queen’.
Terms like ‘drama queen’ or ‘challenging’ were applied to a range of individuals in this study. This is potentially dangerous, as these labels may prevent individuals from being listened to and thus from accessing the support they require to protect themselves from harm. Such labels furthermore emphasise the difference of such relationships to friendships: friends are generally more likely to listen and less likely to dismiss a concern as ‘drama’.
The reaction by Gemma’s key worker was not exceptional. Peter describes the following incident, perpetrated by another user of his day service, which took place during an arts and crafts activity group:
He was teasing with his scissors. He says: ‘I will cut your hair!’ And then he came one time and put the point of the scissors in the back of my head […] And then you just, you just say: […] ‘You’ve been warned. Stop it!’ ‘Why, would I go to prison?’ I says: ‘You did that outside.’ I says: ‘You would.’ I said: ‘If you did anything like that to anybody in [city centre] or round where you live’, […] I says: ‘They wouldn’t put up with it!’
Peter implies that people who attend day centres have fewer rights to protection from threats and intimidation than people ‘outside’. When Peter reported the incident, he was told that the man who threatened him ‘cannot help it’. As with Gemma’s case, staff asked Peter to ignore the behaviour. Peter’s observations mirror research findings of increased levels of violence within segregated settings (Strand et al., 2004) and findings of some level of tolerance for violence amongst staff, who will weigh up whether they perceive an occurrence to be a ‘serious’ incident before reporting it (Jenkins et al., 2008). By doing so, they assert their power to construct what they understand to be ‘abuse’ or ‘violence’, resulting in narrower definitions.
Hostility and Violence
Thus far, the discussion has considered case studies that are not commonly viewed as ‘abuse’ or ‘violence’. However, there is a thin line between mundane experiences of oppression and violence. In fact, mundane oppression makes it difficult to discern when this line has been crossed. In this section, a sample of case studies that can no longer be minimised and would be classed as maltreatment within more conventional frameworks are discussed.
Approximately half of the participants reported an incident of physical or emotional maltreatment, including intimate partner violence and violence by family members. This figure excludes bullying at school, which was reported by three-quarters of those who could remember that far back. Respondents asserted that impairment-specific name-calling was rife in segregated schools and continued at adult day centres. They were addressed with explicitly disablist terms, like ‘backwards’, ‘terminator’ and ‘Mongol’. About a third of people with learning difficulties in Emerson and Hatton’s (2008) study reported that someone had been rude to them within the last year because they are disabled. That includes other users of services, but also, as Ann described, members of the general public: ‘People mean … or they’re saying: “Nut!” Or being away or, walking away … Not talking to me. They no like it, that.’ Ann reported such name-calling as a regular experience.
She furthermore described the day she was robbed: ‘Me meself outside. Boys nicked my … all nicked my purse […] “Give me my purse back!” “No!” And that I said. […] He hit me over here.’ Ann was notably shaken by the incident and made repeated reference to it throughout the interview. This experience led to Ann’s further social exclusion. For instance, she no longer walks to the day centre on her own. Instead, she relies on the council bus. There are some distinct parallels to Britney’s account, which was cited earlier. In both cases, dependency on supporters was furthered, following an incident of victimisation in the community. However, supporting relationships may also be exploited, as the subsequent account demonstrates.
Mary used to live with her nephew, who was physically and emotionally violent and exploited her financially:
Many times I was locked in a room all day and all night. […] I had a bucket [to go to the toilet]. And […] he’s taken all the money off me. He wouldn’t let me have any money, unless I asked him for it and he’d be watching over while I had that.
Here, a range of factors that were described earlier accumulate and characterise this imbalanced relationship. First, Mary was living in a socially excluded setting with limited contact to the outside world. This initially hindered her from seeking help. Mary’s nephew took choices away from Mary, including the choice of how to spend her money and, indeed, he restricted her freedom even further by locking her in a room.
Five respondents described experiences of sexual violence. This incidence is likely to be lower than the actual prevalence amongst the researched population, as about five people who were approached for participation decided not to take part in this study when they learned that violence would be discussed. They were explicit that they did not wish to talk about their personal experiences.
Tyler was sexually violated by a roommate at residential school:
Basically what happened was: He was bi[bisexual]. I didn’t know what bi was when I was at this age. […] I think the phrase is ‘give me a hand job’ whilst I was playing on the games console. … I won’t go down how it escalated from that. It did. […] and then you elbow them in the face to get them off you and they go and tell on you because they raped you. They say you raped them.
As in Mary’s case, the violator exploited an opportunity that arose within a sheltered social setting. He was in a more powerful position, as he was older and possessed knowledge that Tyler did not have at the time. Tyler was therefore unable to make an informed choice about his participation in the sexual acts. He was not taken seriously when he reported the incident, leaving the violator unpunished and indeed free to roam within the residential school, making it likely that further incidents would occur.
Rachel becomes upset whenever she speaks about her past relationship. She and her boyfriend had lived together. The couple were supported by an agency each day and allowed privacy at night. They were initially happy. After about a year her boyfriend became emotionally and physically violent towards her. He was throwing money ‘round the living room … harassing me … getting into bed. Harassing me. Swearing at me. … Pushed me up the wall.’
This experience was painful for Rachel, but nobody had predicted this change in her boyfriend’s behaviour. When Rachel felt unable to deal with the situation herself, she alerted a member of support staff and promptly received the assistance she asked for. She moved out of the couple’s home immediately. She had been listened to. The violence was not tolerated. Rachel was able to make the choice to access support and to break out of a harmful domestic relationship.
Thus far, the discussion has presented an in-depth micro-analysis, which has described oppression and violence from the perspective of affected individuals. In order to present a holistic picture, the following section moves beyond this case study approach and offers a macro-analysis.
Structural Inequalities and a Legacy of Oppression
A workshop at the 5th National Social Work Continuing Professional Development Conference highlighted that there are now such an immense amount of referrals for adult protection that the system has become overstretched (Fyson and Patterson, 2011). Yet, some issues, it was argued, are best addressed elsewhere, as the system is now operating beyond its capacity, which has a negative effect on the timely prioritisation of the ‘more serious’ adult protection cases. The presenters provided attendees with a range of case studies to encourage discussions about this prioritisation process. These included incidents of infringed autonomy, as well as descriptions of indicators that may suggest contact violence has taken place. The task was to decide whether each case study was ‘abuse’ or ‘just poor practice’.
This exercise may be useful for practitioners, as it enables them to evaluate which incidents require adult protection interventions. On the other hand, it could be questioned whether there is such a thing as ‘just poor practice’. Many of the case studies described in the first two data sections of this article could be construed to fall into this category. Yet, these sections described oppressive conditions, which most non-disabled people would not tolerate. Could the label of ‘just poor practice’ therefore be seen as a means by which the powerful, i.e. mostly non-disabled professionals, exercise their authority to define ‘abuse’ in a way that excludes their own behaviours (Baumeister, 1997)? Rather than seeking simplistic estimations on where categories, however defined and named, start and end, this article invites the reader to consider a much broader approach. The macro-analysis presented in this section encourages us to take a further step back and to appreciate the complexity of oppressing and violating structures and processes.
When violence against disabled people is discussed in the popular media, the focus is usually on case studies of extreme incidents, such as that of Fiona Pilkington, who killed herself and her disabled daughter, after her family had been subjected to persistent hostility and attacks by groups of young people in their neighbourhood. UK Prime Minister David Cameron attributed these events to ‘a breakdown of morality in the minds of those thugs; a total absence of feeling or conscience’ (cited in Carter, 2009). This approach focuses explanations for hostility on a few ostracised members of society, who need to be further policed and controlled. Assertions about a continuing ‘moral decline’, leading to social breakdown, keep reappearing in political discourse, for instance, more recently in response to the August 2011 riots in UK cities (Cameron, 2011).
However, as Levin and Nolan (2010) have pointed out, targeted attacks should not be understood as extraordinary occurrences. Instead, they arise from prejudice that is deeply ingrained in the fabric of society. Thus, disabled people are not subjected to violence merely because there are violators. Violence is often allowed to continue because ‘good citizens’ stand by passively and because, as this article demonstrates, incidents are at times trivialised and further facilitated by social systems.
Hostility towards disabled people is by no means a recent phenomenon. Throughout history, philosophers, scientists and medical professionals advocated for differential treatment. For instance, the practice of infanticide dates back to antiquity (Stainton, 1994, cited in Parmenter, 2001: 269). Closer to our times, in the early decades of the 20th century, British eugenicists advocated the view that people with ‘mental deficiencies’ might reproduce ‘excessively’, threatening the national heritage of intelligence (Weeks, 1989). The Nazi project included a strong eugenicist ideology to rid the ‘Aryan race’ of genetic ‘deficiencies’ (Burleigh, 1991).
Even today, some commentators question the extent to which we value disabled people’s lives in the context of the ongoing assisted suicide debate (Campbell, 2004) and in a society that supports selective abortion of disabled foetuses (Saxton, 2010). A recent paper in the Journal of Medical Ethics revived the age-old debate around infanticides by putting forward the new term ‘after-birth abortion’, ‘to emphasise that the moral status of the individual killed is comparable with that of a fetus […] rather than to that of a child’ (Giubilini and Minerva, 2012: 2). It is argued that that the killing of ‘unwanted’ newborns with impairments should be permitted, as ‘life with certain pathologies is not worth living’ and as such children may bring ‘an unbearable burden on to the family and on society as a whole’.
Giubilini and Minerva (2012) may have chosen to refer to disabled people as ‘burdensome’, as they continue to be affected by structural inequalities, resulting in increased access barriers to housing, education, transport, employment and leisure opportunities (Vine et al., 2011). Consequently, many disabled people continue to work, live, learn and socialise in segregated settings.
Mainstream settings often embrace zero tolerance of invasive and violent behaviour. For instance, many workplaces have bullying and harassment policies (see for example NHS Employers, 2006). Such policy frameworks are not common practice in segregated settings. In fact, it was already mentioned that there can be a higher tolerance for violence amongst staff (Jenkins et al., 2008). Within this context, reports of continuing institutional maltreatment of disabled people (e.g. BBC1, 2011), as well as of the overuse of sedative medication on dementia patients (Hollingworth et al., 2011), are perhaps less surprising.
Exclusion from the labour market further contributes to disabled people’s increased likelihood to live in poverty, which has been described as a form of structural violence (Cassiman, 2007). Households that include disabled persons are up to twice as likely to report increased financial difficulties compared to other households (Vine et al., 2011). Possible effects of the ‘structural violence of poverty’ include malnutrition, illness and psycho-social trauma (Cassiman, 2007). In other words, poverty can often cause or amplify impairment.
It has furthermore been suggested that contemporary welfare rhetoric encourages hostile attitudes. For instance, a recent headline story in The Guardian (Walker, 2012: 1) claimed that ‘the government’s focus on alleged fraud and overclaiming to justify cuts in disability benefits has caused an increase in resentment and abuse directed at disabled people, as they find themselves being labelled as scroungers’. In September 2011, two-thirds of disabled people said they had experienced recent hostility or taunts, which is up from 41 per cent four months before (Scope, cited in Walker, 2012: 1). Thus, it is claimed that anti-welfare rhetoric serves to justify derogatory treatment.
This section has provided a brief overview of macro forces, which highlighted how social structures act to systematically oppress and violate disabled people. The discussion has been limited in scope. For a more in-depth exploration of historic developments, see Barnes (1997) or Shah and Priestley’s (2011) discussion of disabled people’s more recent life histories, starting in the mid-20th century. Furthermore, various contributions in the edited collection Disability, Hate Crime and Violence (Roulstone and Mason Bish, 2012) seek to make sense of the incidence of and facilitating factors for targeted attacks against disabled people in contemporary societies.
Discussion: A Continuum of Oppression and Violence
The research advisors articulated outrage about the processes described in the first three data sections. It was therefore initially decided to label all of them as ‘violence’, in order to make a clear statement about their unacceptability (Hollomotz, 2011, 2012). In line with the overall aims of self-advocacy, the intention was to exercise resistance against existing assumptions and to challenge contemporary social care provisions. Yet, this approach did not address the issues that may arise when incidents are excluded from this category and are then labelled as just lesser misconduct. Furthermore, other disabled people who are less politically articulate than the research advisors may not feel as confident to use the term ‘violence’ when describing their experiences.
This article therefore presents a more nuanced, further developed approach. It adopts a broad definition, which takes account of mundane experiences of power, control, oppression and violence. Figure 1 illustrates that these processes can be viewed as forming a continuum.
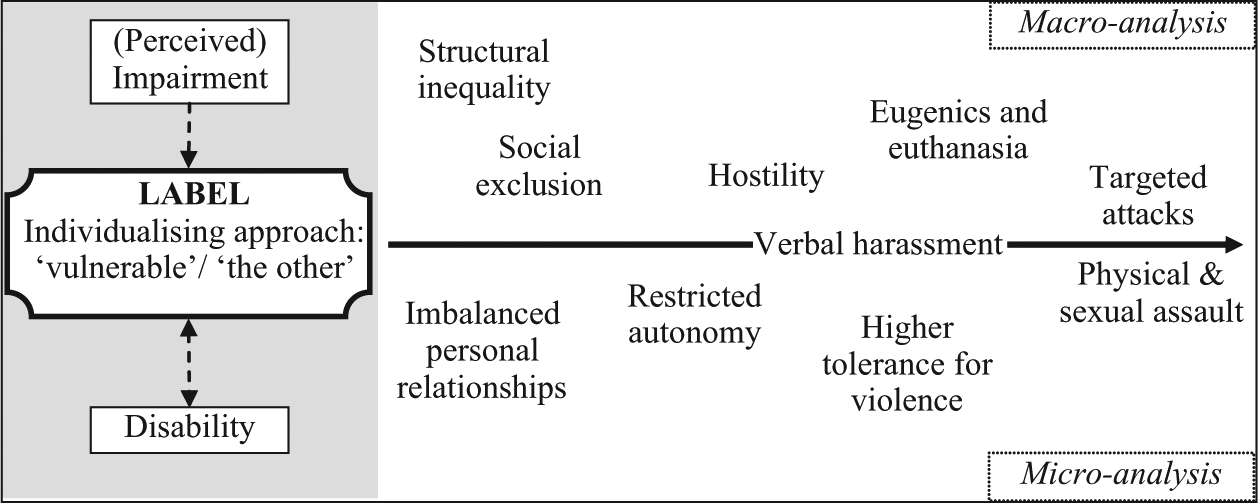
A continuum of disability, oppression and violence.
The reader should note that this continuum is not hierarchical. That means that it does not intend to indicate that, for instance, restricted autonomy has a less damaging impact than hostility. Moreover, categories may overlap and some facets on the continuum will occur simultaneously. In fact, the more facets that occur at once, the more likely it becomes that contact violence will ensue. The continuum applies to the public and private as well as segregated spheres, and only to individuals who are perceived as having an impairment. This became apparent in the case of a woman who was labelled when she was in her early 30s. The processes on the continuum only started at that point. Thus, the starting point of the continuum is the imposition of disability on top of a person’s perceived impairment, via a socially imposed label of ‘otherness’. Many respondents had been subjected to verbal harassment, which reflected hostile attitudes. These were also observed during the macro-analysis of the wider society.
Most participants who led segregated lives understood that this was rationalised with reference to a perceived need to protect them, as they are assumed to be ‘vulnerable’. However, Beck (1992: 20–21) argues that, whatever preventative measures we take, risk remains a ‘primeval phenomenon of human action’. We may wish to predict the outcomes of actions in the social world but the haphazard nature of actual events means that there will always remain an element of risk. The discussion highlighted that the removal of one group of risk factors, such as risks posed by community inclusion, can result in the introduction of yet another, such as risks posed by institutionalisation. Risk is often further amplified by a higher tolerance for violence within segregated settings.
It was outlined that relationships with support workers were often imbalanced. Other important social relationships broke down, due to a lack of support to facilitate contact. This furthered socio-emotional reliance on support workers and family carers and contributed to the creation of isolated dependency relationships, which can become easily exploitable. For instance, many respondents did not recognise restrictions to their autonomy as intrusive. Instead, they expressed gratitude or obedience, which impaired their readiness to self-defend, should immediate danger arise within existing relationships.
To sum up, restrictions to autonomy, lack of opportunities to develop equal social relationships, and social exclusion and hostility are often engrained in disabled people’s everyday lives. This makes it difficult to discern when the boundary between routine experiences of oppression and violence is crossed. The fact that these processes affected a wide range of individuals indicates that targeted crimes and contact violence are not extraordinary occurrences in an otherwise untainted society. Instead they may, as Kelly (1988) suggests, be seen as a mere extension on a continuum of habitual intrusions.
Nonetheless, one case study referred to an incident when a woman who was experiencing domestic violence sought help. On that occasion, the violence was not tolerated. Support workers did not dismiss her concerns. Prompt interventions ended the imbalanced domestic relationships. Even though Rachel continues to carry emotional scars, her case study demonstrates that, even in a society with continuing unequal structures, power and violence can successfully be challenged by those who refuse to accept that different rules apply when we determine what constitutes acceptable behaviour and violence against disabled people.
Conclusion
Derogatory treatment of disabled people is not a recent phenomenon in a society with declining morals. It should not merely be attributed to a few ostracised groups. Instead, categorical treatment of disabled people emerges from a legacy of oppression (Barnes, 1997). It takes place in the public, private and segregated sphere and continues beneath the thin veneer of contemporary rights discourses. Previously, this author suggested that all of these processes should be termed ‘violence’. Yet, after further reflection, this article conveys a sense of uncertainty regarding whereabouts oppression ends and violence starts. With hindsight, identifying such an exact point is neither necessary, nor possible.
Social reality is rarely clear-cut. Asking whether an incident constitutes ‘just oppression’ or ‘violence’, suggests that one act causes less harm than the other and neglects to acknowledge that there is a relationship between the two. To describe disabled people’s experiences of oppression and violence as occurring on a continuum enables a more holistic approach, which has the advantage that shifting boundaries between mundane intrusions and contact violence do not distract attention away from the fact that a range of processes act to systematically oppress and disempower, as well as to breach the human rights of many disabled people.
This broad approach takes account of subtle and mundane incidents of oppression and intrusion. It ranges from structural inequalities, exclusion, imbalanced personal relationships and restricted autonomy, to the ratification of disablist attitudes and a higher tolerance for violence, to emotional, physical and sexual violence in the private sphere and targeted attacks in public. There is no hierarchy. The notion of a continuum acknowledges that all of these processes are harmful and mutually reinforcing.
Footnotes
Acknowledgements
I would like to thank the research advisors, as well as various colleagues and peers who have provided insightful advice, feedback and food for thought, which helped to shape this work. At this stage, I am particularly indebted to Susie Balderston and the reviewers at Sociology.