
Abstract
Urban regeneration (UR) programmes are recognised as a type of Population Health Intervention (PHI), addressing social and health inequalities. Policy recommends programmes involve communities through engagement and empowerment. Whilst the literature has started to link empowerment with health improvement, this has not been within an UR context. As part of broader research on the economic evaluation of community empowerment activities, this paper examines how health gains can be generated through promoting empowerment as well as identifying whether feelings of empowerment are associated with residents personal characteristics or perceptions of their neighbourhood. Using 2011 Community Health and Wellbeing Survey (GoWell) cross-sectional data, ordinal logistic regression and simple linear regression analysis of 15 Glasgow neighbourhoods undergoing regeneration with 4302 adult householders (≥16 years old) was completed. Analyses identified strong associations (P≥ 0.05) between empowerment and the mental health subscale of the SF12v2 and with several items of the Warwick-Edinburgh Mental Well-being Scale (WEMWBS) scale. Furthermore, residents’ who felt more empowered reported more positive attitudes towards their surroundings and housing providers. This concurs with recent evidence of the importance of residents’ psychological investments in their neighbourhood influencing their sense of place attachment. Such analyses present initial evidence of the value of investing resources within UR programmes to activities geared towards increasing residents’ empowerment as a means of producing those health gains often sought by more costly aspects of the programmes.
Introduction
The association between health and the natural and built environment is well researched (Braubach and Sanvelsberg, 2009; Macintyre and Ellaway, 2000; Scottish Government, 2010; Stafford and Marmot, 2003) and indicates that more deprived living conditions increase susceptibility to poorer health. Thus, population health improvements and health inequalities reductions have been identified as potential outcomes of regeneration programmes (Ellaway and Macintyre, 2010; Kearns et al., 2009). These increasingly multi-sectoral urban regeneration (UR) programmes ‘involve complex packages of “components”, such as employment, education, income, crime and housing interventions’ (Petticrew, 2011: 397) and a myriad of activities seeking to ‘improve the interlinked dimensions of household dwelling, community and neighbourhood environment’ (Bond et al., 2013: 941). Despite difficulty evaluating effects of regeneration programmes, there is growing evidence of their wide-ranging impact on residents’ lives. Given this, UR schemes can be seen as a form of Population Health Intervention (PHI) akin to a form of ‘upstream intervention’ (Kelly et al., 2005; MacGregor, 2010; McIntosh et al., 2012).
A renewed focus is being applied to the role of the community within UR programmes (Adamson and Bromiley, 2008; Bailey, 2010; Campbell, 2011). This is evident in Scotland with the Community Empowerment (Scotland) Bill (Scottish Government, 2015) and strategies, such as Glasgow Housing Association’s (GHA) ‘Empowerment and Engagement Strategy 2008/11’, striving to ensure community involvement in the deliverance of local services and neighbourhood renewal (GHA, 2008; Scottish Government, 2015). It is thought that increased participation and autonomy, will give communities a greater sense of local control and empowerment (Bailey, 2010; GHA, 2008; Scottish Government, 2015).
Community actions within regeneration could include: tenant membership of governance structures or establishing consultation groups/public meetings to consider development options (Scottish Government, 2015). Yet the potential for these activities to increase empowerment and whether they could act as a pathway to producing health gains is currently unknown. We have found no published evidence as to whether, in what form, or through which combination of activities, empowerment in regeneration schemes impacts upon the health and wellbeing of the target population groups.
What is empowerment?
As defined by the World Bank, ‘empowerment is the process of increasing the capacity of individuals or groups to make choices and to transform those choices into desired actions and outcomes’ (World Bank, 2011). However, the concept can vary in its form and occur at different ‘levels’: personal/psychological and community.
Personal/psychological empowerment (PE)
PE refers to individuals gaining control over their lives. PE is a term most commonly associated with personal capacity and realising one’s perception of competence and control, the cognitive state (Woodall et al., 2010). At its most basic, ‘individual empowerment basically means people feeling and actually having a sense of control over their lives’ (Woodall et al., 2010: 9). However, it is possible to go beyond this and appreciate that such simplicity disguises the myriad of dimensions behind PE. Highly variable, the ‘root’ of this form of empowerment is within the individual and as such, perceptions and feelings are individual- and context-specific, can fluctuate over a lifespan and can take different forms in difference circumstances.
Community empowerment (CE)
Laverack and Labonte (2000) and Laverack (2006) highlight that central to many narratives of CE is the idea of ‘power’, particularly how communities work together to gain more control over decisions that influence their lives through a shift in power relations between themselves and others (notably policy-makers). In this form CE is a ‘process’, however it can also be treated as the ‘outcome’ from this enhanced autonomy and influence. Such opinions are mirrored by the Scottish Government with their 2015 Community Empowerment (Scotland) Bill and previously published ‘Scottish Community Empowerment Action Plan’, acknowledging that in order to create vibrant communities, the government cannot force or compel empowerment processes on the citizens. Instead some facilitating may be needed in order to ‘remove barriers, promote better opportunities and support those already involved’ (COSLA and Government 2009: 3). This process of building a relationship between the community and a public body ‘to help them both understand and act on the needs or issues that the community experiences’ is known as ‘community engagement’ (Scottish Community Development Centre (SCDC), 2005), a key to building Community Empowerment (GoWell, 2011).
Zimmerman (1995) and Speer (2000) have argued that PE is an inherently interactive process as individuals do not become empowered on their own. As individuals gain a positive self-perception and more confidence they will be willing to seek change in their local environment and develop their awareness of key issues, by engaging with others, their local surroundings and developing relationships. This perception of an individual’s sense of PE necessitating the incorporation of relationships and stepping outside their own concerns to be able to embrace the issues of others, striving to act for the collective good, demonstrates how PE and CE may be interlinked. It also provides an initial indication of how looking at PE could provide further information on the potential for fostering CE yet as explained later in this research, such development is highly context specific.
The research described in this paper is located within the GoWell programme. Research previously conducted within GoWell examined what is meant by empowerment within UR (Kearns and Lawson, 2006; Lawson and Kearns, 2006), and for the UR context and purposes of this paper we apply the resulting definition of empowerment as: a community’s ability to make choices and ultimately exert influence on decision-making, thus feeling that they have some ‘control’ over the UR process (GoWell, 2011; Scottish Government, 2015) whilst operationalising a measure of an individual’s perception of their own empowerment within the community context.
Place and empowerment
The geographical context within which empowerment occurs is important, as it is in specific ‘places’ that individual/psychological and CE may be linked. Skerratt and Steiner (2013) argue PE does not always result in CE occurring and that there should be a stronger consideration in research of the complexities of empowerment. Moreover, studies should acknowledge that communities are the result of many differing identities, histories and social relationships. These differences between individuals and their allegiances to places affect a community’s potential capacity and sense of empowerment. Furthermore, places are residential psychosocial environments that can affect individual and collective wellbeing through factors such as environmental quality and relative social position, in turn affecting people’s commitment and optimism about empowerment (Kearns et al., 2012). Area perceptions (such as relative status and quality) can also influence individual’s self-regard, in turn affecting their mental wellbeing and PE (Bond et al., 2012; Gilchrist, 2009). Studies of empowerment must incorporate this place–individual–collective interplay.
Empowerment in an UR context
UR programmes vary in form and impact on residents. Community participation has become recognised as integral to successful regeneration (Adamson and Bromiley, 2008). Expectation is that communities should be central actors (COSLA and Scottish Government, 2009). This contrasts to top-down processes, led by professionals, criticised for not meeting communities’ requirements or expectations (Findlay, 2010). As Lawson and Kearns (2014) highlight, local and national agencies are recognising the benefits of working with communities. However, they acknowledge that the current evidence base poses questions regarding the suitable delivery of these policies. Researchers such as Taylor (2003) clearly demonstrate how failure to address power imbalances between stakeholders and communities can restrict benefits and exclude communities. Yet successful stakeholder and community partnerships, working towards common goals has shown evidence of empowerment occurring (Colenutt and Cutten, 1994).
Collaborative partnerships seek to address community and stakeholder agendas in a manner suiting both parties. Approaches such as flexible timetables to fit other resident commitments allow communities the appropriate timeframes to engage in participation activities (Colenutt and Cutten, 1994; Mathers et al., 2008). Furthermore, when stakeholders recognise communities’ local expertise and existing social ties, communities have felt more involved and in control within the decision-making process (Adamson and Bromiley, 2008; Muir and Rhodes, 2008).
In contrast, exclusion from decision-making can create feelings of powerlessness and mistrust. Studies have reported residents frustration with the UR process and their lack of control (Pollock and Sharp, 2012; Stubbs et al., 2005). Non-transparency of decision-making can produce resentment, with communities feeling ‘disenfranchised’ as influential decisions are made out of their hands (Pollock and Sharp, 2012; Stubbs et al., 2005).
It may also be the case that residents of disadvantaged areas may obtain feelings of empowerment from sources other than their involvement in decision-making. Specifically, if regeneration serves to improve the quality of people’s housing and neighbourhoods, this may result in positive mental wellbeing outcomes and feelings of empowerment (Bond et al., 2012), particularly if residents’ have waited a long time for improvements. People may also derive feelings of empowerment through the social capital – friendship networks and social interactions – they develop within their neighbourhood (Halpern, 2004).
From available evidence, it may be concluded that empowerment in UR is closely associated with feelings of control and a sense of involvement in the process. These feelings have also been linked to empowerment in recent reviews on health and empowerment (Laverack, 2006; Wallerstein, 2006; Woodall et al., 2010). To foster empowerment successfully in an UR context collaboration is needed between the community and other stakeholders (Adamson and Bromiley, 2008). Empowerment in UR can take a number of forms, yet central to its development is residents feeling their views are heard by policy-makers, and having some control over local issues.
Relationship between empowerment and health
Empowerment strategies, whereby communities have a key role in decision-making, have demonstrated a potential to induce positive health outcomes.
There is evidence based on multi-level research designs that empowering initiatives can lead to health outcomes and that empowerment is a viable public health strategy. (Wallerstein, 2006: 4)
Underpinning most expressions of empowerment is the aim that people will gain the ability to seek an improvement in their circumstances (Woodall et al., 2010). Processes by which PE and CE could produce health gains have been recognised in the work of Woodall et al. (2010) and Wallerstein (2006), both demonstrating that the empowerment of individuals and communities can enable them to control their local circumstances, health concerns and behaviours. They also suggest that empowered communities could have the capability to undertake a more active role in the provision of services such as healthcare, with the associated potential for impacting a range of health issues (Woodall et al., 2010).
Evidence suggests that empowerment could improve six aspects of an individual’s mental health and wellbeing (Woodall et al. 2010). These are: improved self-efficacy and self-esteem; greater sense of control; increased knowledge and awareness; behaviour change; greater sense of community; and broadened social networks and social support.
Based on a review of existing evidence, Woodall et al. (2010) argue that the clearest evidence of empowerment strategies and interventions impacting health outcomes is demonstrated by improvements to an individual’s psychological wellbeing and sense of control over their circumstances. Their review demonstrates that participation or collective working led to increased feelings of control over issues and enhanced perceptions of their self-worth (Woodall et al., 2010).
Aims
The aims of this research were to examine, in an UR context:
whether feelings of empowerment are associated with personal and socio-demographic characteristics of residents;
to what extent feelings of empowerment are associated with processes of area regeneration that involve different types of resident and community engagement;
whether feelings of empowerment are associated with residents’ relationships with, and perceptions of, their housing and neighbourhood;
whether feelings of empowerment are associated with general, physical and mental health and wellbeing outcomes.
Methods
Setting
The research was undertaken in the UK city of Glasgow, where there has been a regeneration programme underway since 2006, following the transfer of the city’s housing stock to GHA in 2003 (Pawson et al., 2009). The stock transfer was unique in scale, involving 83,000 dwellings (Scottish Executive, 2000; Kearns and Lawson, 2009). Crucially, three things were enabled. First, investment financed the improvement of approximately 50,000 housing units, to bring them up to new legally required housing standard (Communities Scotland, 2007). Second, the initial stock transfer to GHA was to be followed over the next decade by further, smaller acts of Second Stage Transfer (SST), whereby local groups of dwellings would become ‘community ownership’, initially envisaged to involved around 60 smaller transfers (GHPSG, 2000). Third, GHA and the city council, would identify Transformational Regeneration Areas (TRAs) for large-scale housing demolition and subsequent redevelopment. GHA anticipated demolishing nearly 19,000 dwellings city-wide (Glasgow City Council, 2007; GHA, 2006). Our study covers areas undergoing each of these three types of regeneration, positioned at the heart of all of which was the Scottish Government’s commitment to empowerment for all communities, but particularly disadvantaged communities (Scottish Executive, 2002; Scottish Government, 2009).
The GoWell Survey
Empowerment data from the 2011 GoWell Community Health and Wellbeing Survey of 15 Glasgow communities undergoing regeneration was used (Egan et al., 2010). These study areas, comprising 32 subareas, are among the most deprived neighbourhoods nationally, all with levels of income deprivation falling within the bottom 15% of areas in the Scottish Index of Multiple Deprivation (Egan et al., 2010).
Four thousand two hundred and seventy adult householders aged 16 years or over (one householder per household) from these areas were interviewed about their personal circumstances, perceptions of their communities and neighbourhoods, and the state of their health (Egan et al., 2010). Full details of the study design have been published elsewhere (Egan et al., 2010).
Measures
These analyses utilise data from those respondents who answered the empowerment related question: How much do you agree or disagree with the following statement: ‘On your own, or with others, you can influence decisions affecting your local area?’. This question formed the outcome measure for study aims 1–3 and the independent variable for the fourth study aim. Five response categories were used: strongly disagree, disagree, no opinion/unsure, agree and strongly agree. The ‘agree’ and ‘strongly agree’ response categories are seen as positive indicators of empowerment. The question was adapted from the Home Office Citizenship Survey (Attwood et al., 2003) by the GoWell research team. As highlighted in the introduction, there is evidence to suggest that PE and CE are interlinked, as PE involves individuals increasing interaction with others as they gain more control over local decisions and is not something achieved in isolation from their surroundings and others and is highly context specific (Laverack, 2006; Zimmerman, 1995). Therefore, we used this measure of PE which embraces both the respondent’s personal influence but also that which they gain with others. This hybrid question relates to both PE and also collective CE issues and processes.
A suite of socio-demographic variables were used to explore whether specific personal characteristics have an association with sense of empowerment (study aim 1). See Table 1.
Ordinal logistic regression of empowerment with socio-demographic characteristics and area-based engagement type.
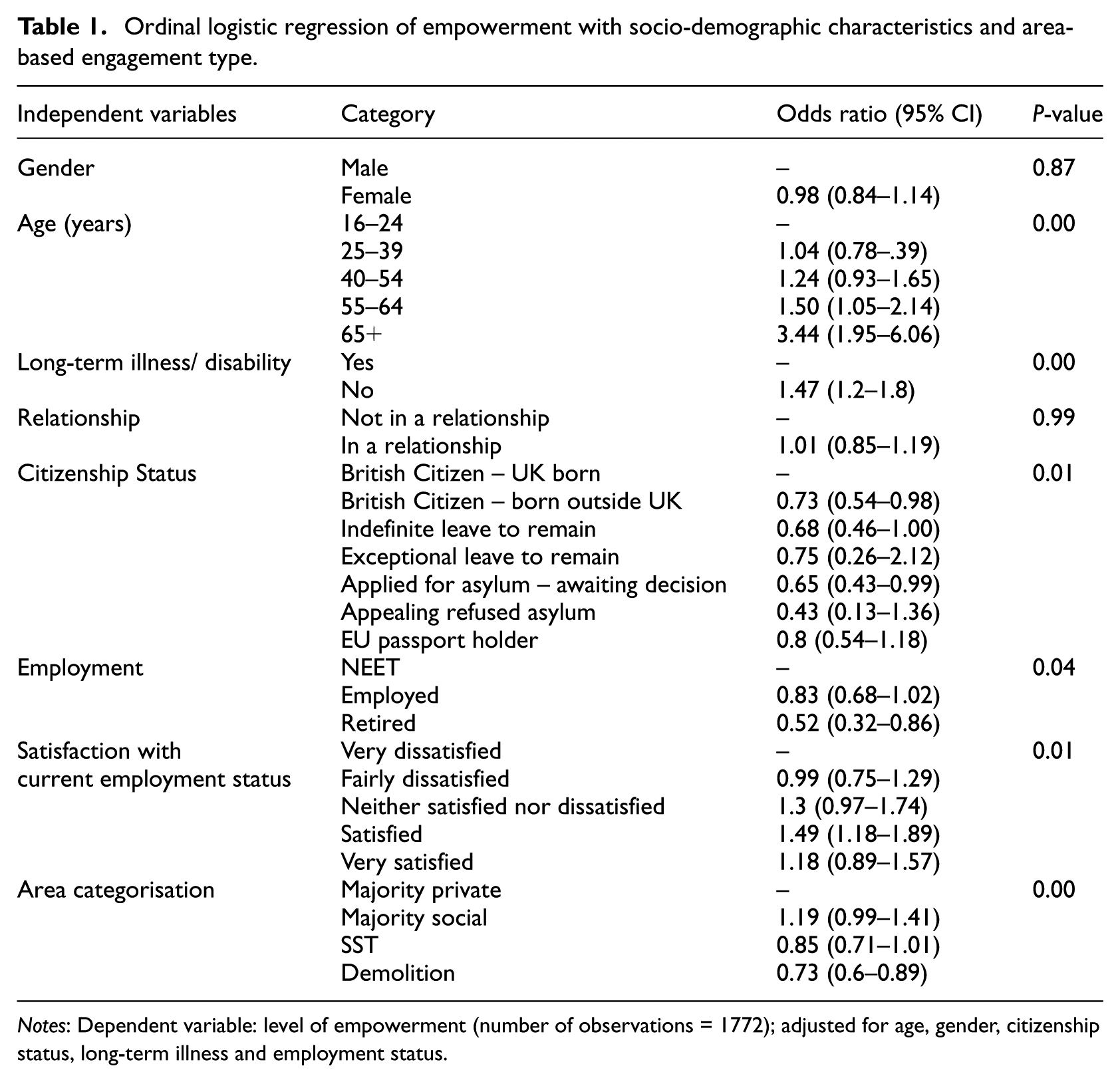
Notes: Dependent variable: level of empowerment (number of observations = 1772); adjusted for age, gender, citizenship status, long-term illness and employment status.
For study aim 2, we considered the areas where respondents lived. The 32 subareas were categorised according to the main regeneration process underway, involving a different resident engagement procedure. As a reference category, we identified areas where the majority of the housing was private sector (not subject to regeneration). Next, areas of majority social housing were identified. Here dwelling improvement works involving individual consultation with occupants regarding timing, and choice of finishings (Curl and Kearns, 2015a). Third, areas where SST had occurred in recent years and both individual and collective/community consultation had actively taken place, with residents voting ballots regarding which alternative landlord (if any) they wished to transfer to achieve local ownership of the housing stock (McKee, 2007; Scottish Housing Regulator, 2009). Lastly, areas of major demolition and redevelopment were identified. Here collective consultation processes were enacted to consult on intended demolition and create masterplans for the area redevelopment (Lawson and Kearns, 2010b). The categories are shown in Table 1.
For the third aim of the research, we examined how long residents had lived in the area and in their current home. Level of satisfaction with their home, existing housing services and local neighbourhood as a place to live were also incorporated. Lastly, respondents’ participation in social clubs and associations, sense of belonging to the neighbourhood, level of acquaintance and interaction with neighbours and proximity to close friends and family were included to indicate whether participants’ social interactions in their local neighbourhood were associated with empowerment (Table 2). For the fourth study aim the outcome of interest was physical and mental health and wellbeing. Two health scales were included: the Warwick-Edinburgh Mental Wellbeing Scale (WEMWBS) and the SF-12v2 Health Survey (Tennant et al., 2007; Ware et al., 1996), see Table 3.
Ordinal Logistic Regression of Empowerment with Housing and Neighbourhood Variables.

Notes: Dependent variable: level of empowerment (number of observations = 1772); adjusted for age, gender, citizenship status, long-term illness and employment status.
Linear regression results for SF-12v2 and WEMWBS scores.

Note: adjusted for age, gender, citizenship status, long-term illness and employment status.
Analyses
The first phase of analysis involved exploring univariate relationships between the empowerment variable and, first, a range of socio-demographic characteristics, level and type of engagement enacted within their area through regeneration, and, lastly, housing and neighbourhood factors, to build a profile of empowerment within the study communities. Following cross-tabulations, ordered logistic regressions were conducted. The empowerment question was the dependent variable, providing an indication of those characteristics with a relationship to empowerment that might be viewed as empowerment predictors. Respondents with missing data were excluded from the analyses.
The second phase of analysis involved multivariate analysis of associations between empowerment and the three health-dependent variables, controlling for socio-demographic measures. Linear regression was used when analysing the continuous dependent variables: WEMWBS overall score and SF-12v2’s two component scores and overall score. Lastly, a further stage of analysis examining the impact of empowerment on WEMWBS health states was conducted. Empowerment was the independent variable whilst the 14 WEMWBS health states were the dependent variables in the logistic regressions. STATA 12SE statistical software was used to conduct these analyses. Variables were adjusted for age, gender, citizenship status, long-term illness and employment status. A statistical significance level of 5% was used throughout.
Results
The sample comprised 41% males and 59% females. 40% of participants described themselves as feeling empowered; 31% stated their views do not influence local decision-making; and the remaining 28% were uncertain of their sense of empowerment, responding either ‘don’t know’ or ‘neither agree nor disagree’.
The results tables show the odds of giving a higher (more positive) response to the empowerment question, across the five response categories.
Empowerment and socio-demographic characteristics
Table 1 shows that participants’ age, absence of long-term illness, citizenship status, employment status and satisfaction with their current employment situation are each significantly associated (p-value < 0.05) with empowerment. Long-term illness was the only socio-demographic characteristic to show a clear, positive, association with empowerment, throughout all levels of empowerment. Absence of a long-term illness increased the odds of reporting a higher level of sense of empowerment by over 40% (OR 1.47, 95%CI 1.2–1.8). With regard to the findings by age group, those who were older were more likely to report a greater sense of empowerment. Those aged 65 years and over were significantly (p = 0.03) more likely to report the greatest sense of empowerment (OR 3.44, CI 95%1.95–6.06).
Empowerment and area-based engagement
Table 1 shows that ‘area categorisation’ and ‘type of engagement’ were significantly associated (p-value 0.00) with empowerment. Those people living in areas of majority social housing, where housing improvements and associated consultation with individual occupants was the predominant form of engagement, were more likely to feel empowered than those people living in areas of majority private housing (OR 1.19, 95% CI 0.99–1.41). However, people living in areas where either SST or demolition had occurred (also consisting mostly of social housing) were less likely than those in the other two areas to report feelings of empowerment (OR 0.85, 95% CI 0.71–1.01 and 0.73, 95% CI 0.60–0.89, respectively), despite processes of both individual and collective engagement occurring in these locations.
Empowerment and housing and neighbourhood factors
With regard to housing and neighbourhood factors, feelings about the neighbourhood as a place to live, and views about housing services mattered more for empowerment than social relationships. Table 2 shows that neighbourhood satisfaction was associated with a trebling of the odds of higher feelings of empowerment compared with extreme dissatisfaction (p-value 0.00). Similarly, satisfaction with housing services from the landlord or factor was associated with more than a doubling of the odds of higher feelings of empowerment (p-value 0.00). Those who had a strong sense of belonging or who knew more people in their neighbourhood also had higher odds of reporting stronger feelings of empowerment. Despite being significant (p-value 0.02) no overall trend was shown between feelings of empowerment and length of residence in current home or area. In contrast, participation in clubs and associations and proximity of friends and family did not show any association with sense of empowerment.
Empowerment and health
Table 3 presents the results the linear regressions examining whether empowerment acts as a predictor of better physical or mental health and wellbeing. There is a clear significant (p-value < 0.00) trend for general health that those who express a stronger sense of empowerment have a higher SF-12 overall score than those who are unsure or feel they are not empowered.
Physical health scores show no association with feelings of empowerment. For mental health and wellbeing, both the SF12_MCS and WEMWBS overall scores exhibit a clear trend whereby higher levels of empowerment are associated with better mental health and wellbeing. The effect is stronger for the positive mental wellbeing (WEMWBS) score than for the mental health (SF12-MCS) score. Those with the strongest sense of empowerment have a higher SF-12 MCS score (+3.56, 95% CI: 1.60–5.51) and a higher WEMWBS score (+6.70, 95% CI: 4.99–8.35) than those with the lowest feelings of empowerment.
Five aspects of mental wellbeing within the WEMWBS had a statistically significant overall trend of association with levels of empowerment. These were; ‘I’ve been feeling optimistic about the future’ (p-value ≤ 0.02); ‘I’ve been feeling useful’ (p-value ≤ 0.05); ‘I’ve been feeling relaxed’ (p-value ≤ 0.02); ‘I’ve been feeling good about myself’ (p-value ≤ 0.05) and ‘I’ve been interested in new things’ (p-value 0.00).
Discussion
As previously identified, the role of empowerment within the delivery of UR has become a core element and objective over recent years. Analyses presented show that, within the context of deprived neighbourhoods undergoing UR, empowerment acts as a predictor of better general and mental health. Additionally, other personal and residential characteristics can also predict a resident’s sense of empowerment.
Our empowerment profiling has shown that those with a long-term illness or disability feel less empowered, which may suggest that current practices employed by stakeholders have failed to engage with these residents, and particular attention is required to ensure that these individuals can interact with decision-making. The link between PE and CE is also a consideration here. Other GoWell analyses have shown that respondents with a long-term illness or disability experienced amongst the highest levels of financial problems during the recession period 2008–2011, leading up to the survey analysed here (Curl and Kearns, 2015b). Additional qualitative research with groups at risk of financial difficulty also revealed that psychological responses to such problems included lower feelings of self-worth and withdrawal from peer interaction (Trevisan et al., 2014). It is therefore possible that our findings on lower levels of empowerment among the ill and disabled partly reflects this wider sense of isolation.
Older participants felt more empowered than their younger counterparts. This is unlikely to simply be a consequence of having more time to participate in local activities, as analyses on employment found no association between empowerment and those not in work (retired or unemployed). That is not to underestimate the importance of stakeholders considering the time commitments expected of residents, and the timing of engagement activities to take account of people’s other commitments. Previous work by Adamson and Bromiley (2008) similarly suggest the important role of collaboration and the need for communities and policy-makers to understand one another’s agendas and other commitments.
Satisfaction with housing services was strongly associated with feelings of empowerment, with those most satisfied with the delivery of landlord services reporting a greater sense of empowerment. Our findings on satisfaction with housing services suggest that policy initiatives such as the Scottish Social Housing Charter, encouraging landlords to view tenants as valued customers who should be ‘treated fairly and with respect’ (Scottish Government, 2012: 5) could have positive spill-over effects upon feelings of empowerment and mental wellbeing outcomes for the tenant population. This may be because relatively deprived populations experience few situations in which they are treated as valued citizens.
Our findings on the relationship between housing services and feelings of empowerment are reflected in our assessment of area-based engagement processes. Here, we found that the highest likelihood of feelings of collective empowerment was to be found in areas of predominantly social housing, where engagement with individuals around housing improvements had occurred. It is interesting that this one-to-one relationship may spill over into feelings of empowerment in relation to area-based decisions (the subject of our empowerment question). This may either be because the improvement to someone’s home, and the respectful, empowering interaction between landlord and tenant that occurs over this, gives the tenant a broader sense of efficacy, or that the landlord is seen to be an effective conduit for tenant concerns about the area, i.e. the resident may derive feelings of direct or indirect empowerment as a result. This is an example of the growing need and demand for recognition and respect among the poor, the absence of which is said to damage people’s sense of identity, generating feelings of anger and invisibility (Lister, 2002).
In the other two situations examined here – where collective, area-based engagement processes had occurred around second stage stock transfer and demolition and redevelopment – we found lower likelihoods of feelings of empowerment than elsewhere, contrary to expectations. Findings from other strands of the multi-methods GoWell programme can help understand this. Earlier qualitative research with local housing committees showed how the outcomes of SST are very place-contingent. In areas where local committees faced a lot of non-housing issues such as poor quality environments, lack of services and facilities more generally, and transient populations, stock transfer could still leave residents feeling a lack of power, although this could be ameliorated if the housing organisation of which they were part had good connections to other organisations and partnerships outside the area to help find solutions to local problems (Lawson and Kearns, 2010a).
Similarly, research with residents in areas of demolition, including with those who had been involved in consultation processes around master-planning exercises, revealed that, despite a number of engagement events and processes organised by the regeneration partners, people still felt a lack of empowerment, sometimes because they had no understanding of who was making the final decisions about their areas’ futures – the decision-making process had not been explained to them, or because they did not know how agreed plans were to be funded and progressed, nor who they could ask about progress – the implementation process had not been explained to them either (Lawson and Kearns, 2010b, 2014). Others have argued that housing providers should put in place feedback mechanisms that allow residents to understand the impact of their views and the rationale for the final decisions that were taken (Stubbs et al., 2005).
Thus, community engagement processes can be inadequately specified, producing weaknesses in the process and its aftermath, or narrowly proscribed such that they are unable to respond to variations in circumstances faced by communities living in different places. The result is that individual residents may not derive a sense of empowerment from either their participation in, or the ripple effects of, collective community engagement processes.
Our results demonstrate that feelings of empowerment were also associated with places in other respects, namely satisfaction with the neighbourhood as a place to live, and having a sense of belonging to the local community. As residents feel more connected to surroundings they develop more interest in the happenings and issues affecting themselves and others (Nienhuis et al., 2011), promoting greater involvement in local issues and potentially higher feelings of empowerment.
Surprisingly, no association between respondents’ feelings of empowerment and their degree of social connectedness or their participation in local activities was shown. Empowerment appears to be affected by perceptions of the extent to which the actions of others can be influenced, and whether those actions create a satisfactory environment (whether in terms of service provision, neighbourhood quality or ‘belonging’) for the respondent. In contrast, the respondent’s own actions (in terms of participation in activities or links with others) do not appear as markers of empowerment. The important narrative is more about a neighbourhood identity where a sense of pride in the local neighbourhood and genuine connection to their local area has led to respondents pursuing an interest in local issues and developing a sense of empowerment. Residents’ psychological investment in places with which they are associated has been investigated previously to demonstrate its influence on place attachment (Livingston et al., 2008). Whether this process of psychological investment similarly impacts on a community’s sense of empowerment has yet to be determined.
In this research, those with higher levels of empowerment reported higher levels of mental health and wellbeing. Indeed, those who felt they have some influence over local decisions recorded significant improvements in several items of the WEMWBS scale, measuring positive mental wellbeing. As discussed earlier, the link between empowerment and health has previously been theorised in literature and policy guidance, yet there has been no clear evidence of health being directly influenced by empowerment within an UR setting. The results in this paper are subject to limitations, but they suggest that successful facilitation or fostering of empowerment may contribute to some of the additional health gains sought in PHIs.
The lack of evidence in our study of links between empowerment and improvements in physical health gains is in line with previous research (Wallerstein, 2006; Woodall et al., 2010), where physical health was only seen to be affected by empowerment once the community felt empowered and then chose to change the delivery of local services such as local leisure facilities. This might suggest a pathway whereby mental health gains are necessary precursors to physical ones, as participants’ self-efficacy, confidence and coping behaviours (as shown in the WEMWBS scale) confer an ability to shape factors that in turn benefit physical health.
Investments by stakeholders increasing interaction with the community and ensuring that residents feel involved in the decision-making process, or foster feelings of community and belonging to their neighbourhood, could benefit individuals’ health. Thomas et al. (2013) highlighted that engagement with communities requires ongoing partnerships with stakeholders to enhance their current resources and knowledge thus enabling the community to ‘sustain its own efforts’ and ensure it can raise issues of concern effectively and act in a collective manner (Thomas et al., 2013: 123). Implicit within this argument is recognition of the value of bringing the human resources and capabilities that exist within communities alongside those of service providers to produce more sustainable and equitable outcomes. Our findings could be seen as providing a health rationale for the co-production of community services which others have called for (Durose et al., 2013). There are, however, resource implications and the study reported here is the first stage of a programme of research seeking to understand the additional economic ‘worth’ of investing in empowerment activities in relation to the benefits gained within a formal economic evaluation.
Limitations of the study
The cross-sectional design of this research means that our findings can only be understood as establishing associations, and we have been unable to demonstrate causality. We have been able to illustrate that empowerment could lead to improvements in mental wellbeing at a specific point in time, but we are unable to examine if this association has occurred or endured over time in this context. The picture might indeed be one of reverse causality (better mental wellbeing leading to empowerment) or, more likely, of a two-way relationship.
Capturing residents’ and communities’ engagement levels through recording willingness to participate in the intervention has attracted criticism as shown in the recent work carried out by ‘Well London’ (Philips et al., 2014). Solely using participation levels to conceptualise engagement could fail to capture external factors that impact respondents’ level of participation (Philips et al., 2014). Yet, despite the potential limitation of only having the responses of those individuals inclined to engage in the GoWell programme, the work being presented here can act as a preliminary indicator of how fostering the development of CE can lead to improvement in the mental wellbeing of residents.
Our variables are self-reported and, although based on validated questions, we recognise the scope for reporting bias. More objective measures, however, would not have penetrated the issues of interest in this study.
The empowerment question used to depict respondent’s levels of empowerment incorporates both considerations of PE and CE. The wording ‘on your own, or with others’ does not allow the researcher to determine whether it is a stronger sense of PE or CE that the respondent is referring to, although the question was placed between others which referred to the ‘people in the area’, thus encouraging a collective train of thought. Furthermore, as previously discussed within this work, there is existing research on how an individual’s sense of place can affect their sense of PE and CE. Whilst the use of the wording of the empowerment question does raise some doubt if it refers explicitly to CE, analyses conducted and shown in Table 2 show a clear positive association between this measure and respondents’ satisfaction with their neighbourhood and their sense of belonging, therefore it could be argued that it acts as a validated indicator of CE. Nonetheless, future research could better distinguish between these different dimensions, possibly with the introduction of separate measures for PE and CE.
Lastly, the empowerment question asks respondents about their perceived sense of CE (On your own, or with others, you can influence decisions affecting your local area?), it does not ask participants to provide examples of when they feel they had actual empowerment and influence. Building on analyses shown here and previous qualitative work, there is scope for future work investigating the potential differences between perception of empowerment and actual evidence of having influence over decisions. However, this was beyond the reach of this piece of work.
Conclusions
In addressing its research aims, this study has found statistically significant positive associations between individuals’ perceptions of their sense of empowerment and mental health (but not physical health) in neighbourhoods currently undergoing regeneration. The study used respondents’ perceptions of empowerment and influence gained not only by themselves but working collectively. The findings present a compelling argument for paying more attention to PE and CE in UR programmes as empowerment represents a clear pathway to producing those health gains commonly sought from the more substantial and costly aspects of the UR programmes (improvements to local environments and the quality of homes). Policy-makers have emphasised the role of the community in the delivery of UR yet evidence has shown that despite these recommendations, practice often fails to fully realise this vision (Lawson and Kearns, 2014). Communities are not regularly involved in decision-making beyond initial consultation processes. Opportunities for CE are not always sustained and communities are often left feeling alienated from their immediate environment and the changes taking place and impacting on their lives (Blakeley and Evans, 2009; Bowie et al., 2005). As Lawson and Kearns (2014) illustrate, this can lead to feelings of disempowerment in the community.
Our findings add to, and reinforce, messages from previous research in this area which similarly suggest that stakeholders should seek to engage more with the community and examine possible ways to ensure that residents feel both part of the community and some degree of control over their immediate surroundings and the changes occurring as a result of regeneration. There is, however, a lack of understanding of ‘what works’ in sharing decision-making with communities, and how stakeholders might most effectively facilitate and foster CE in regeneration programmes in a cost-effective way. The findings presented here emphasise a need for more research and a clearer understating of residents’ capabilities and assets in the early stages of UR programmes. We have shown how different types of engagement activities can both foster and hinder sense of empowerment and thus, if stakeholders wish to promote CE, they should first consider residents’ PE and the current roles in which they work collectively. Such work will provide evidence to inform the optimal allocation of resources within regeneration processes in the pursuit of improved and more equitable health and wellbeing within and across communities.
Footnotes
Funding
The authors are grateful to the following for funding: NHS Greater Glasgow & Clyde; NHS Health Scotland; Scottish Government; University of Glasgow 66597; Wheatley Group.