
Abstract
The outbreak of a virus such as COVID-19 is composed of a series of seemingly random incidents which are nevertheless interconnected. In a novel approach, this article adopts the event system theory (EST), established in organisational behaviour science, to investigate the mechanism of epidemic governance in Wuhan, the city which reported the first case of COVID-19 and thereafter successfully controlled the outbreak. The event system analysis divided Wuhan’s response mechanism to COVID-19 into four dimensions: the graded response systems, the interactive relationship between multilevel entities of epidemic governance, the quarantine regulations and the governance of public sentiment. There are numerous lessons learned and effective measures developed from the ‘Wuhan experience’. These lessons and measures can assist other cities around the world to cope with the current COVID-19 crisis and prepare their urban governance systems for similar infectious diseases in the future. We urgently advocate the addition of more scholarly discussion on urban epidemic governance by incorporating interdisciplinary approaches like EST in particular.
Introduction
The COVID-19 pandemic is an unprecedented disaster that severely impacts the development of human society, especially in densely populated urban areas. Wuhan was the first city to report a case of COVID-19 in December 2019, but in June 2020, less than seven months after the outbreak, Wuhan successfully demonstrated control of the situation. In contrast, many other cities around the world are still fighting multiple waves of the pandemic. Primarily, the success of Wuhan in containing the virus is attributable to the effective countermeasures taken by the city. Subsequently, the ‘Wuhan experience’ was used for reference by other cities in China and elsewhere.
However, in the current literature, there is a lack of in-depth analysis of how Wuhan was able to achieve successful control of the outbreak. Seeing that the COVID-19 pandemic shows no signs of slowing, the urban public health response mechanisms and governance systems around the world are facing severe challenges. In this context, utilising knowledge gained in Wuhan such as epidemic prevention and control and exploring generalisable urban responses and strategies will have immediate and practical significance, helping to guarantee the health and safety of cities worldwide.
Furthermore, this is not the first example of an urban society under threat by an infectious disease. In the past two decades, driven by the successive appearance of the 2003 SARS epidemic, the 2009 H1N1 epidemic and recently the COVID-19 pandemic, urban epidemic governance systems have been constantly improving (Ali and Keil, 2008). Previous outbreaks have demonstrated that major public health incidents represent opportunities to optimise governmental responses to emergent epidemics. However, it is usually challenging to provide a holistic analysis of the effects of each epidemic on urban governance systems because the outbreak of a new epidemic usually involves a series of fragmented emergent events. These events are random, uncertain and seemingly inconsequential but closely interconnected. As far as these events are concerned, existing urban studies offer limited theoretical instruments that can provide a reasonable way of understanding the causalities and links between them.
In view of this, this article clarifies the response mechanism to COVID-19 in Wuhan using the event system theory (EST), adopted from organisational behaviour science. It constructs a novel research framework for urban studies based on diversified, multi-dimensional and multi-faceted events. By adopting this approach, this article establishes ties between the major events involved in the outbreak, spread, control and evolution of COVID-19 in Wuhan. The aim is to provide theoretical and empirical support for further optimising urban epidemic governance with regard to collaboration between different entities involved in epidemic governance. EST is capable of identifying the causality between, and external effects of, complicated multi-entity events so as to more easily uncover the black box from a series of ‘disorganised’ events.
The remaining sections of this article are arranged as follows: the second section offers an introduction to EST and its applications in urban governance studies. The area of focus and the methods employed in this article are outlined in the third section. The fourth section, the main part of the article, explores the evolution and improvement of the mechanism of epidemic governance in Wuhan through event system analysis. Finally, the fifth section gives a summary of the article and discusses the generalisability of the ‘Wuhan experience’.
Urban epidemic governance and multilevel entities
Research on epidemic governance in cities
Cities, on account of their dense, highly mobile population and rapid cross-regional traffic networks, are extremely vulnerable to emergent infectious diseases. The bubonic plague, also called the ‘Black Death’, that swept across Europe in the 14th century was a typical urban epidemic. However, studies on urban epidemic governance did not receive close attention from scholars until 20 years ago. In this field, a book edited by Ali and Keil (2008), Networked Disease: Emerging Infections in the Global City, is a pioneering work. By offering a systemic elaboration of the relationship between the SARS outbreak and cities, the authors hold that modern cities create ideal conditions for the spread of emergent infectious diseases. Particularly, against the backdrop of globalisation and commercialisation, cities have become hubs in the network of infectious diseases. Accordingly, the authors summarise three basic dialectical processes in the outbreak of an urban epidemic: the urban–global dialectic, the nature–social dialectic and the rural–urban dialectic. These processes suggest that future studies on urban epidemic governance should pay close attention to the interconnectivity between people, viruses, and technologies, and how these interconnections are influenced by cultural, economic, and political forces.
Meanwhile, some scholars have proposed a conceptual framework involving the political ecologies of health and disease (PEHD), arguing that this political, ecological approach can satisfactorily explain the political relations involved in urban epidemic governance. This theory offers a systemic method for interpreting the social inequalities and environmental damages caused by diseases. It is an important theoretical basis for investigating the issues of health justice, the politics of epidemic management and the debate on urban density (Connolly et al., 2017; Duminy, 2023; Harper, 2004; Houston and Ruming, 2014; Jackson and Neely, 2015; King, 2010; McFarlane, 2023). In their latest publication, Connolly et al. (2020) combine urban epidemic studies with the PEHD framework and highlight the need for future urban health policies that focus on the threats posed by epidemics to peri-urban or suburban areas. The lack of development in these areas in terms of demographic change, infrastructure and urban governance makes them vulnerable to epidemic outbreaks (Connolly et al., 2020). Further, many studies have focused on the resilience of communities to natural disasters (like earthquakes and climate change) by building bioecological models. These allow for the multi-scaled measurement of the effects of natural disasters on different ecological, social, economic, infrastructural or institutional aspects (Bronfenbrenner and Ceci, 1994; Cui et al., 2018; Folke, 2006; King, 2007).
In response to the current global COVID-19 pandemic, more studies are focusing on urban epidemic governance. Cities with integrated urban governance strategies are more likely to implement effective controls and processes. As such, they can recover more quickly than other cities (Sharifi and Khavarian-Garmsir, 2020). Such actions involve engaging in substantial testing and surveillance, introducing timely lockdowns and social distancing, providing sufficient medical and technical support and, most significantly, ensuring coordination between all levels of the government and non-governmental organisations (Duggal, 2020; Earl and Vietnam, 2020; Pulighe and Lupia, 2020; Qian and Fan, 2020). Successful lessons were observed in countries such as China, Vietnam and South Korea where the immediate responses by local governments and top-down governance mechanisms were essential in coordinating different social sectors. Contrastingly, in countries like Australia and the USA, the fragmented policy and confused countermeasures severely affected responses to the pandemic (Hesse and Rafferty, 2020; Wilkinson et al., 2020). By comparing responses in East Asian countries, Shaw and his colleagues found that the performance of local governments, community solidarity and citizens’ behaviour all played a decisive role in controlling the COVID-19 pandemic. Furthermore, the use of modern technology was also vital for delivering effective treatment and tracking asymptomatic cases (Shaw et al., 2020).
Though great progress has been made by previous studies in urban epidemic governance and related fields, there is still a lack of appropriate theoretical instruments capable of probing the interconnectedness and interactions between different stakeholders like citizens, professional groups, enterprises and municipal governments during ‘disorganised’ public health emergencies such as the COVID-19 pandemic. For instance, the PEHD framework specifically concentrates on social and environmental justice in epidemics. Meanwhile, bioecological models for responding to natural disasters focus on assessing the factors that cause the emergent events. The analytical framework contributed by Shaw et al. (2020) utilises events analysis but does not follow EST in its key concepts and mechanism of interpretation. This article, therefore, is one of the first to focus on the municipal response mechanisms to COVID-19 by using EST, which will be addressed in the following section.
Event system theory in relation to urban epidemic governance
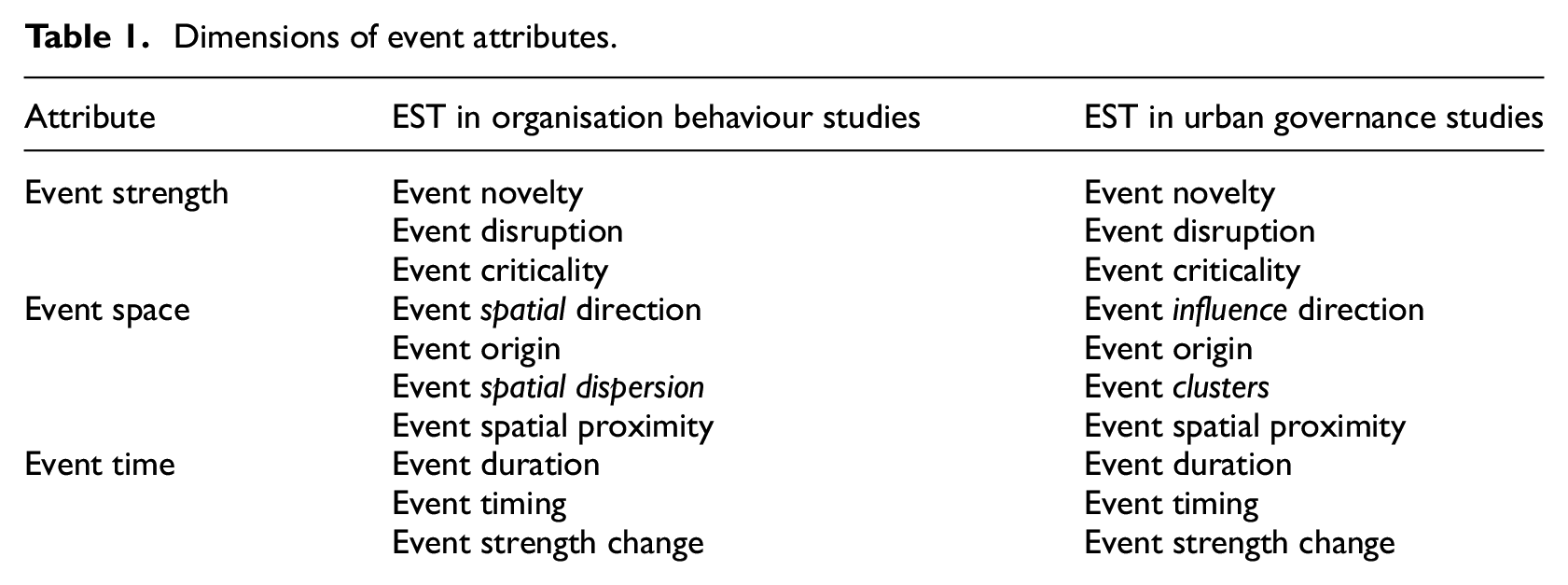
EST was developed as part of organisational behaviour science. Compared with open system theory (OST), which concentrates on recurring events that create a state of organisational stability (Miller and Rice, 2013), EST explores the dynamic effect of event–external environment interactions on organisations based on the interactions between organisational hierarchies and entities. The degree of the effect depends on three essential attributes of an event: event strength, event space and event time (Table 1). Among them, event strength includes the three dimensions of novelty, disruption and criticality. A more novel, disruptive and important event is more likely to change or create behaviours, characteristics and subsequent events (Morgeson et al., 2015). Event space refers to the specific occurrence position of an event and the spread of its effect in an organisation. The event takes place at a certain level in the organisational hierarchy, and its effect ‘moves’ within a certain level or between different levels. Studies of event space consider four dimensions: event spatial direction, event origin, event spatial dispersion and event spatial proximity. Event time is investigated from three perspectives: event duration, event timing and event strength change. Specifically, spatial attributes (such as event origin, event spatial dispersion and event spatial proximity) and temporal attributes (such as event duration, event timing and event strength change) regulate the relationship between event strength and event result (Morgeson et al., 2015).
Dimensions of event attributes.
Seen from the perspective of organisational behaviour science, EST effectively integrates the advantages of variation-oriented and process-oriented theoretical paradigms. EST also distinctly reveals the hierarchical structure and temporal dynamics of event-related organisational phenomena (Liu and Liu, 2017). Existing EST studies are primarily focused on the effects of events on entity behaviours. They look at two basic levels: the organisational level of enterprises (e.g. Connelly et al., 2020; Hartwig et al., 2020) and the micro level of employees (e.g. Johnson and Johnson, 2017; Koopmann et al., 2016; Laulié and Morgeson, 2021). Against the backdrop of the COVID-19 pandemic, some scholars have explored the effects of the pandemic on different entities in organisational systems using EST. Vaziri et al. (2020) discuss the changes in the work–family conflict faced by employees in an organisation during epidemics and the work-related consequences caused by shifts in employees’ moods. They also explore how an organisation can give more credit to the roles of employees in public health emergencies. McCluney et al. (2020) investigate the generation of anti-racist resources during epidemics and other events. Craighead et al. (2020) use EST to analyse the effects of epidemics on supply chain management and policy making. Shaw et al. (2020) investigate how China controlled the outbreak of COVID-19 on a national scale over time using a narrative style. They identify four event clusters with great implications on epidemic governance. More recently, Liu et al. (2023) suggest that organisational interventions have a positive effect on frontline health workers when it comes to their perception of the meaningfulness of their work. Similarly, Lin et al. (2023) propose that adaptive practices in organisations have played a positive role in mitigating the impact of the novelty and criticality of COVID-19 (but not the disruption) on employees’ perception of their job insecurity.
Nevertheless, the above EST-based studies do not investigate urban behaviours in an epidemic in detail. Relatively few of them focus on the connections between events (event chains) and the continuous interactions between entities (event evolution) in epidemics. EST offers a novel research perspective and epistemological method for studying the roles and actions that unconventional, discrete events play in complex systems like urban response mechanisms to COVID-19, which are sporadic and dynamic. Notably, however, compared with the hierarchical structure composed of environments, organisations, teams, individuals and other entities in organisational systems (Figure 1(a)), the multi-level entities in urban epidemic governance are highly multiplexed and loosely organised. However, this does not mean that EST is not applicable to city-level governance. In the view of liberal and neoliberal governance, the city is the basic unit for dealing with all sorts of public affairs, such as environmental policy, planning practices and crisis management (Gibbs and Jonas, 2000; He et al., 2020; Jessop, 2002; Sager, 2011). To achieve an efficient response to a public emergency, there must be significant coordination. This can cause tension between the different levels of urban entities, as in the case of single institutions. Therefore, this article proposes a comparable framework of a hierarchical urban event system structure composed of the institutions or regulations, governments (including central and local governments), professional groups or teams (e.g. doctors, engineers and specialised enterprises) and citizens (Figure 1(b)). Under this framework, the inheritance, establishment and evolution of institutions are general factors affecting urban responses. They interact with governments, organisations, individuals and the institutional environment.

The hierarchy of EST for urban epidemic governance. (a) Hierarchy of EST in organisation behaviour study. (b) Hierarchy of EST in urban governance study.
On the other hand, however, because the structure of event entities at the city level is different from that of single organisations where subordinate relationships exist between various entities, it is necessary to modify some dimensions of event attributes, concerning, in particular, the attribute of event space. As urban entities are essentially dispersed, it might be less applicable to examine the spatial direction and dispersion in the urban event system. Instead, it is very important to identify inter-connected events (event clustering) in public health emergencies like the outbreak and control of COVID-19 (Shaw et al., 2020). Therefore, we replace event spatial direction with event influence direction, and adopt the concept of event clusters as a substitute for event spatial dispersion in event space analysis (Table 1). This modification will make the EST approach more adaptive for an investigation on urban epidemic governance.
Study area and data collection
Wuhan, the city used as the case study in this article, is the provincial capital of Hubei Province in Central China and has a resident population of more than 11 million. As a megacity, Wuhan is well-known as a ‘thoroughfare of China’ and has a high population density, large mobility scale and a rapidly growing manufacturing sector. According to Ali and Keil (2008), Wuhan, as a traffic hub of the country, is one of the central places of networked diseases and is naturally vulnerable to the spread of emergent epidemics.
This article offers a summary of the events related to the outbreak, spread and control of COVID-19 in Wuhan (see Supplemental Material). The statistics for the events started in December 2019 when a patient in Wuhan was recorded with pneumonia from an unknown cause. The statistics ended on 13 June 2020 when the response grade to public health emergency in Hubei province was adjusted to Level III. The events were carefully selected and processed with the support of an expert-based assessment that was conducted by five experts in the field of public health management and urban studies. First, in the process of searching for raw materials, keywords and headlines such as ‘COVID-19’, ‘novel coronavirus’ and ‘pandemic’ were used to identify the relevant reports through official channels (e.g. the Information Office of the State Council, the official website of the Chinese Center for Disease Control and Prevention) and public media (e.g. Xinhua News Agency, China Daily, BBC News). Each event had to be confirmed by multiple sources of information to guarantee its authenticity. It is important to keep in mind, however, that biases might exist both in domestic and external channels for reasons such as political prejudice and gaps in the first-hand sources. Therefore, the second step was to evaluate the objectivity of events by an expert scoring method. Thereafter, the final selection of the events was conducted based on an overall evaluation of their reliability, relevance and significance to urban epidemic governance of COVID-19 in Wuhan. Redundant events and less influential events (i.e. events with a low Baidu search index), as well as biased reports, were excluded. Finally, a total of 114 events were documented over a period of nearly eight months. These events were further categorised into four levels according to their origins in the hierarchy of EST for urban epidemic governance (Figure 1(b)). There were 16 institution-related events (e.g. Wuhan city locked down), 33 government-related events (e.g. a working group was sent to Wuhan by the central government), 49 professional group-related events (e.g. Zhong Nanshan confirmed human-to-human transmission) and 16 citizen-related events (e.g. students began online classes at home). Admittedly, this classification system is not infallible since there were some events involving multilevel entities.
Urban response mechanisms of Wuhan in coping with COVID-19
The outbreak of COVID-19 in Wuhan, as a typical urban public health emergency, was unforeseeable, nonlinear, urgent and fuzzy. A large event number, multiple event entities and high event density characterise the urban response event system of Wuhan. To establish event ties for numerous incidents related to the outbreak and control of COVID-19 in Wuhan, this article classifies the events into four sequences that constitute the basic framework of the urban response mechanism to epidemics: the graded response systems, the interactive relationship between multilevel entities, the quarantine regulations and the governance of public sentiment.
The graded response systems
After the SARS epidemic, the central government of China proposed an emergency management system called ‘one plan supported by two systems’. The ‘plan’ was to implement classified management and graded responsibility for governments at different levels. ‘Two systems’ referred to the two types of classified response systems. The first type is comprised of national classified response systems, which were developed by the Chinese Center for Disease Control and Prevention (‘China CDC’). Depending on their severity, public health emergencies are classified into four grades: general, major (Level III), serious (Level II) and especially serious (Level I). The second type is comprised of local classified response systems. According to the Law of thePeople’sRepublic of China on Prevention and Treatment of Infectious Diseases, the classification of the outbreak, the prevalence of infectious diseases within a jurisdiction and the necessary emergency work plan should be made by local governments and reported to higher levels of government for their records.
By examining the evolution of the critical events that triggered the adjustment of response measures, it is suggested that the graded response mechanism of Wuhan played a critical role in the governance of COVID-19. At the national level, the Wuhan Municipal Health Commission (WMHC) made the judgement on 5 January 2020 that the novel virus was not SARS or any other respiratory virus. It reported 59 confirmed cases (G8). This event conformed to the following circumstance for triggering a major public health emergency: ‘An infectious disease that has not yet been discovered in China has occurred or has been introduced.’ The following day, China CDC launched a Level-II emergency response mechanism (I2) (Figure 2). On 12 January, the WMHC announced in an information circular that the pneumonia found in patients was caused by a novel coronavirus (G10). In the meantime, the Ministry of Public Health in Thailand reported that a laboratory had confirmed a case imported from Wuhan, which met one of the criteria for an especially serious public health emergency: ‘A new infectious disease has occurred or an infectious disease that has not yet been discovered in China has occurred or has been introduced, with a tendency to spread.’ On 15 January, the National Health Commission (NHC) held a national teleconference (G11) to emphasise the urgent need to control the epidemic. Then, China CDC launched a Level-I emergency response (I4).
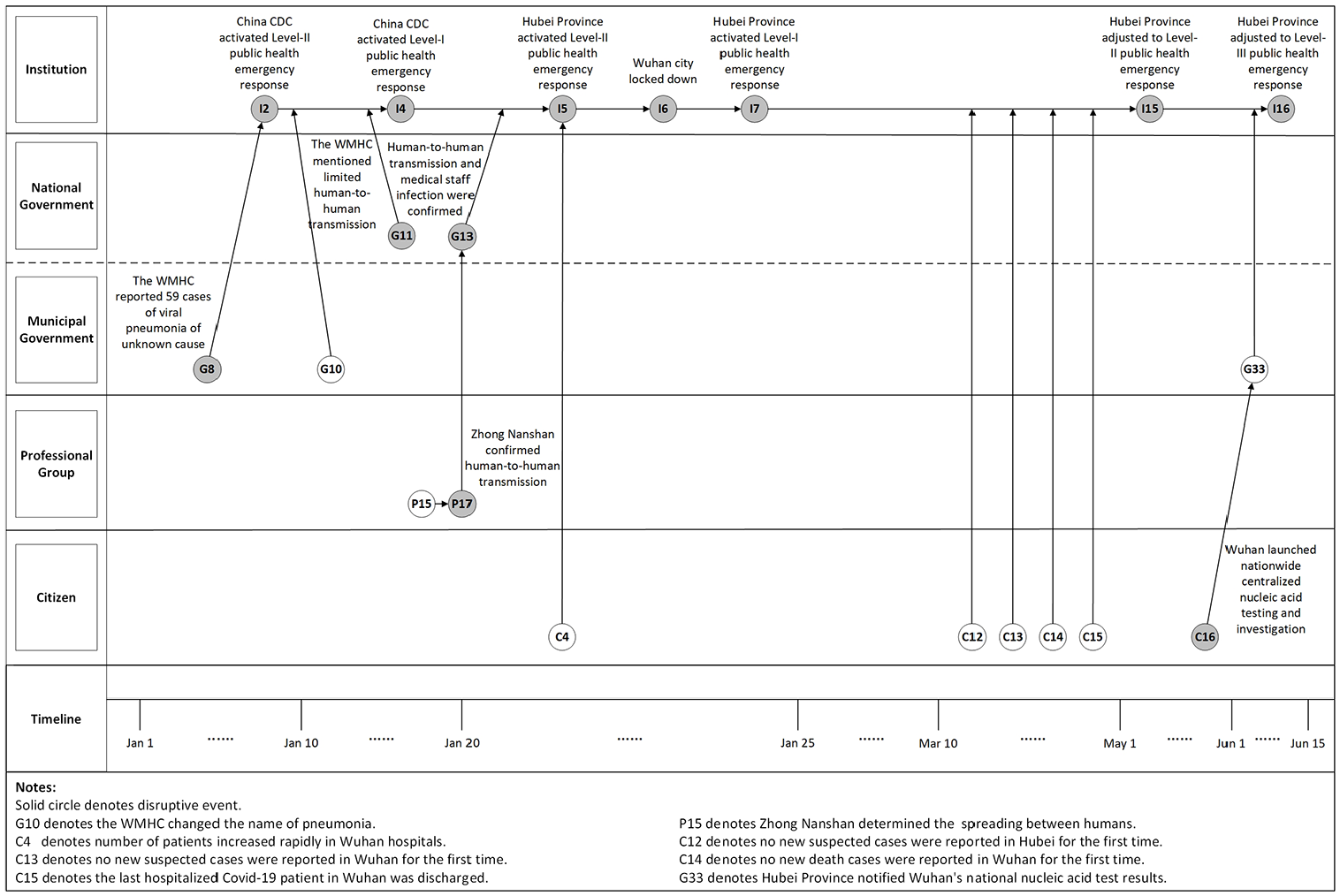
Evolution of events on the graded response systems to COVID-19 in Wuhan.
Seen from a local level, the occurrence of COVID-19 was somewhat unprecedented (novel) for Wuhan since the city is far away from the epicentre of SARS. Only a dozen SARS cases were reported there in 2003. However, soon after the professional group confirmed ‘person-to-person transmission’ and medical staff infection (P15, P17, G13), as well as further aggravation of the epidemic (C4), the local government triggered a Level-II public health emergency response mechanism (I5) in Hubei Province. Later, the local government in Wuhan introduced the ‘lockdown’ (I6) measure, the most important and disruptive urban response in epidemic governance. Only three days after launching the Level-II emergency response mechanism, it was upgraded to Level I (I7). This urgent response was not lowered until Wuhan had reported zero new suspected cases (C12), zero newly confirmed cases (C13) and zero new deaths (C14) and the last hospitalised COVID-19 patient had been discharged (C15). On 2 May, the public health emergency response was lowered to Level II in Hubei Province (I15). After conducting citywide nucleic acid testing (C16) and reporting the results of tests (G33) in Wuhan, the emergency response mechanism was further lowered to Level III (I16) on 13 June 2020. The event chains related to the adjustment of the public health emergency grades in Wuhan suggest that timely responses to emergent epidemics are key to mitigating the rapid spread of a disease in its early stage.
The interactive relationship between multilevel entities
The mechanism of epidemic governance in Wuhan was a sturdy, top-down response. It is generally believed that this highly concentrated response mechanism offers an effective way of controlling the spread of epidemics (Sharifi and Khavarian-Garmsir, 2020). There are five top-down management paths that can be identified in the event system, namely: ‘National Government–Municipal Government’, ‘National Government–Professional Group’, ‘Municipal Government–Professional Group’, ‘Municipal Government–Community’ and ‘Community–Citizen’ (see Figure 3). Among these relationships, ‘National Government–Municipal Government’ interactions were impressively effective. For instance, after a continuous surge in the number of patients at the respiratory clinics of hospitals in Wuhan (C2), the NHC sent its working group and expert team to Wuhan (G3) and drew up the Guidelines on Early Detection, Early Diagnosis and Early Quarantine for Prevention and Control of Viral Pneumonia of Unknown Cause (G6) along with nine other documents (G7), including the Diagnosis and Treatment Protocol for Viral Pneumonia of Unknown Cause (for Trial Implementation). These measures provided guiding support to local governments in their urban responses.

Interactive relationships of multilevel entities in Wuhan epidemic governance.
‘National Government–Professional Group’ interactions were demonstrated by the events of national support for urban medical institutions. For instance, after ‘lockdown’, medical support teams from the national military and other provinces were sent to Wuhan (P23), which was the largest dispatch of medical forces since the founding of new China. A total of 17 military medical teams arrived in Wuhan within three days of the ‘lockdown’, followed by more than 100 medical teams from other provinces. Additionally, during the outbreak and spread of the disease, Wuhan faced a huge shortage of medical supplies (P18, P26). To solve this problem, the central government coordinated and provided medical supplies to Wuhan’s medical institutions on many occasions.
‘Municipal Government–Professional Group’ interactions were primarily manifested as the direct administration of medical institutions and research institutions by municipal governments. For instance, the Wuhan government organised the planning, building, opening and closure of Huoshenshan Hospital (P19, P35, P47), Leishenshan Hospital (P25, P38, P48) and several mobile cabin hospitals (P34, P36, P41, P43). ‘Municipal Government–Community’ and ‘Community–Citizen’ interactions were present in community management and governance events. After proposing zero-COVID communities on 12 February 2020 (G23), the municipal government empowered grassroots communities to properly control the citywide access of residential communities by reporting suspected cases, delivering daily necessities to families, controlling mobility and gathering residents (P24, P28). In addition to the collaborative interactions between multilevel entities, sharp conflicts and tensions developed under different circumstances. For example, when the strict quarantine was implemented in some communities (I10, I11), there were conflicts between residents and supervisors (C10). Meanwhile, due to a shortage of medical and living supplies in the lockdown (I6), local citizens were discontented with the institutions in charge of social donations (e.g. the Wuhan Red Cross) because of their inefficient delivery and distribution of donated materials (P44).
Although top-down management systems played a critical role in the governance of the epidemic, our retrospective event analysis reveals that bottom-up information transmission mechanisms were also critical. As shown in Figure 2, among various types of response mechanisms triggered by events, disruptive events usually depend on a bottom-up transmission route; that is, event entities that upgrade the response mechanisms are frequently individuals and professional groups. For instance, the first case of COVID-19 in Wuhan could be traced to 1 December 2019, but it did not immediately trigger the local public health response mechanism. In fact, high-level epidemic governance entities failed to fully appreciate the danger of the infectious disease even after the suspected case had been reported by a doctor (P1). Local health organisations also did not adjust the emergency response level at the very beginning. This led to wide criticism over the government’s response from local professional groups (P45).
However, after the confirmation of ‘person-to-person transmission’ (G11, P17, G13) by Zhong Nanshan and other members of the medical expert team sent by the NHC, the Wuhan government triggered a Level-II public health emergency response mechanism (I5) immediately. It took several measures (e.g. lockdown, community quarantine, building new hospitals) to counter the contagion of COVID-19. This led citizens to eventually win the battle. Event timing analysis of the multilevel interactions highlights the importance of a fast mechanism for bottom-up information transmission, especially considering that advice from professional groups may play a decisive role in effective epidemic control.
The quarantine regulations
According to Ali and Keil (2008), cities are vulnerable to epidemic outbreaks because of their dense populations and high levels of mobility. As a result, restricting population mobility and person-to-person contact and maintaining social distancing are essential for preventing and controlling infectious epidemics. The ‘Wuhan experience’ tells us that it is critical to introduce a comprehensive quarantine system to prevent the spread of COVID-19. This must involve hospitals, communities and other local social actors. The ‘lockdown’ of a city can effectively cut off the inter-city and large-scale transmission routes. Meanwhile, when it comes to the precise quarantine of citizens, modern technical means are also indispensable, such as detection techniques and the tracking of personal mobile phones.
Quarantine regulations in hospitals
During the 2003 SARS epidemic, an important prevention and control measure taken by Beijing was to isolate sources of infection. For instance, Xiaotangshan Hospital was built to provide isolated diagnosis and treatment for patients infected with SARS. However, COVID-19 is more infectious, and its spread was exacerbated by the Spring Festival travel increase (C3). Thus, besides isolation of infected people, it was also critical to isolate virus carriers and control super-spreader events. To cut off the transmission of COVID-19, a series of even more rigorous quarantine measures was conducted in hospitals in Wuhan and nationwide.
On 6 January 2020, Zhongnan Hospital of Wuhan University renovated its ICUs into isolation wards (P6) but had already reached full capacity on 10 January (P8) (Figure 4). In mid-to-late January, the existing shortage of medical resources, medical supplies and test kits was further aggravated, and hospitals were overwhelmed by patients from the entire region. Those who could not get admitted into a hospital became mobile infection sources. To solve this problem, Wuhan officials prepared to construct Huoshenshan Hospital on the day of ‘lockdown’ (P19) and then Leishenshan Hospital two days later (P25). They were opened for clinical reception on 10 and 13 January, respectively (P35, P38). Simultaneously, a condition-specific and category-based approach was taken by all Wuhan medical institutions in treating feverish patients (I8). On 3 February, the Wuhan Municipal COVID-19 Prevention and Control Command Center decided to build mobile cabin hospitals (P34), and the first mobile cabin hospital was put into use two days later. From 5 to 22 February, 16 mobile cabin hospitals with more than 14,000 beds were opened (P36). In mid-February, the Chinese government formally proposed to ‘admit all confirmed cases for treatment’ and ‘treat and quarantine them by categories’ (G21). After that, the number of newly confirmed cases began to drop rapidly in Wuhan. This testifies to the critical role of medical quarantines in urban emergency responses.

Evolution of events related to the hospital quarantine system.
Quarantine regulations in communities
In China, due to economic system reform and changes to social patterns, the centralised ‘working unit system’ social governance pattern is being gradually replaced by a ‘community system’ pattern, or ‘xiaoqu’ in Chinese. Under the ‘community system’, gated and semi-gated neighbourhoods progressively become the basic units of China’s urban governance. While practising community quarantine, Wuhan successfully established a system of community-based governance.
The event system analysis suggests that after Wuhan’s ‘lockdown’, increasing emphasis was placed on local governance at the neighbourhood level, which had become the key to preventing the spread of COVID-19 within the city (Figure 5). In the initial period after the outbreak, no community-oriented prevention measures were taken in Wuhan. On 18 January 2020, two days before the confirmation of ‘person-to-person transmission’ (P17, G13) by the prominent experts of the NHC, the Baibuting Community of Wuhan was still holding its traditional party called the ‘Banquet of Ten Thousand’ (P16). Considering that more than 40,000 households in the community took part in the banquet, the dissemination risks posed by this event were significant. The unprecedented surge in the number of patients in some hospitals (C4) further promoted the ‘lockdown’ of Wuhan (I6). On the next day, more than 2000 community secretaries in Wuhan joined the online networking groups of community residents to screen feverish patients within their respective jurisdictions and to serve residents better (P24).
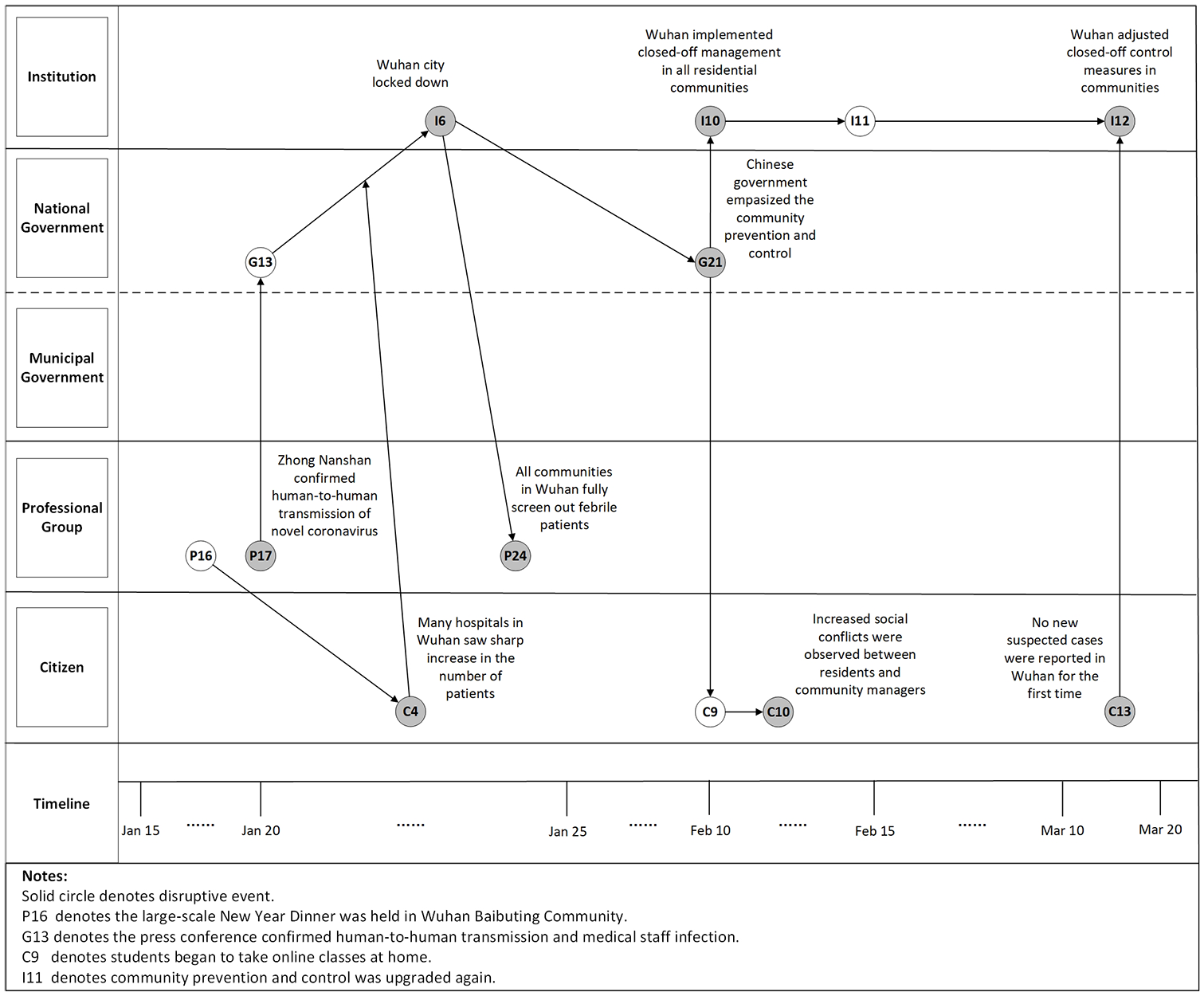
Evolution of events related to quarantine regulation in communities.
On 10 February, General Secretary Xi Jinping emphasised the importance of communities as the first line of defence in the control of the epidemic (G21). Later that day, Wuhan implemented city-wide access control of residential communities (I10). Initially, this measure restricted access to one person at a time every three days (I10). Later, with the continual upgrading of community control systems, this control limited access only to patients and people in critical positions related to epidemic prevention or social functioning, and no community residents were allowed to leave Wuhan (I11). This rigorous quarantine lasted until Wuhan officials reported zero newly confirmed cases (C13). On the same day as C13, the community epidemic governance group of the Wuhan Municipal COVID-19 Prevention and Control Command Center issued a statement on adjusting the epidemic governance measures. They allowed limited access to zero-COVID communities (I12). Activities in small groups were allowed only in batches at certain times in specific buildings. School teaching and business operations were moved online (C9).
In the early stages of implementing strict community isolation in Wuhan, social inadaptability and conflict were observed between residents and community managers (C10). However, after the city authorities publicised the recent occurrences in Wuhan and demonstrated how harmful it would be to everyone if the epidemic spiralled out of control (C9), citizens began to work together during the lockdown. At this time, community-based actors, including street committees, property management companies, volunteers and other social forces, were vital in maintaining order in the community and in channelling external supplies (e.g. food and medical necessities) to those who needed it. Later, when the city returned to normal, community-based actors continued their significant role in reporting on the health of rehabilitated persons and organising massive nucleic acid testing (C16) and vaccination. This story tells us that grassroots governance and community autonomy are indispensable in strict quarantines as part of the overall process of urban epidemic governance.
The technical support for quarantine from enterprises
Enterprises were heavily involved in the response to COVID-19 in Wuhan. They produced and distributed medical supplies and provided technical support during the quarantine. There are different roles that enterprises had in the urban response to COVID-19 (Figure 6). First, producers of medical materials around the country produced as many medical supplies as the hospitals and citizens in Wuhan needed. In mid-to-late January 2020, Wuhan began to experience a shortage of surgical masks, protective suits and other medical supplies (P18, P26). Since enterprises based in Hubei Province could not resume operations and production at that time, external support was crucial to maintain the supply of medical necessities. Taking masks as an example, the daily mask production capacity of the whole country was about 8 million on 25 January, but this rose to 116 million by the end of February (G18). Second, construction enterprises took part in building temporary infrastructures for emergency responses. For instance, Wuhan Zall, a local logistics company, participated voluntarily in the construction of seven hospitals during the epidemic. The company also deployed two mobile cabin hospitals (P39). Third, technological enterprises provided urban governance solutions. In the early stage of the pandemic, many high-tech enterprises provided dependable technical support to increase governmental efficiency. They delivered supplies using robots and tracked and forecasted the pandemic using big data and robust computing platforms. They helped non-COVID-19 patients use online inquiry platforms. Notably, Tencent, a Chinese company that develops Internet-related products and services, actively developed the first standard on ‘health QR codes’, which labels citizens’ risk of being infected based on their trajectory. The standard was formally submitted to the NHC for approval in March 2020 (P42). It later became the universal standard to control mobility in China through access to public transport, for example. This support significantly improved urban and community responses and created a management pattern that was extensive and robust.

Evolution of events related to technical support from enterprises.
To identify asymptomatic carriers after effective epidemic control, citywide nucleic acid testing and screening were conducted (C16). Testers went door to door after the lockdown was lifted (I14). The citywide screening covered nearly 10 million people (almost the entire population of Wuhan), excluding children below six years of age. More recently, to promote vaccination for all citizens, online booking systems based on personal mobile numbers were developed to allow people to register for vaccination. By 15 June 2021, over 70% of the adult population in Wuhan had been injected with at least one dose of the COVID-19 vaccine. Without energetic support from medical and technological enterprises, it would have been impossible to accomplish nucleic acid testing and vaccination on such a large scale. All in all, numerous enterprises demonstrated a strong sense of social responsibility, took part in varied urban responses and offered material and technical support for urban epidemic governance.
Governance of public sentiment
Public sentiment is an important factor affecting epidemic governance. It refers to the attitudes of the public towards epidemic policies, as well as their willingness to cooperate with these policies. In the early stage of the COVID-19 outbreak, responses from multi-level entities varied dramatically due to their differences in proximity to the event. Local governments, for instance, were rather cautious about increasing publicity about the unknown, infectious disease. On the other hand, professional groups like doctors on the front line who were coping with COVID-19 were fully aware of the risk it posed. They strongly recommended upgrading the level of emergency response. By contrast, citizens were still largely uninformed about COVID-19 and the severity of the situation. Therefore, at this point, the authoritative dissemination of knowledge, education and guidelines was essential to ensuring public calm.
In the event system of urban responses to COVID-19 in Wuhan, many disruptive events affected public sentiment significantly. For instance, the upgrading of the epidemic situation (G2, G8), the lockdown of Wuhan (I6), the access control of residential communities (I10), the construction of mobile cabin hospitals (P34), the provision of online education (C9), the organisation of city-wide nucleic acid testing (C16) and many other unprecedented events all aroused surges in public sentiment. In this article, two typical event clusters were extensively examined due to their substantial effect on stabilising social mentality and rectifying unreasonable behaviours.
The first event cluster is related to the authoritative notification of COVID-19, which proved to be crucial for reassuring the public and dispelling rumours in the early stages of the outbreak (Figure 7). The COVID-19 crisis in Wuhan started when Dr Zhang reported suspected cases to the hospital and the Wuhan Jianghan Center for Disease Control and Prevention (P1). Local governments then immediately issued an urgent notice (G2), activated the epidemic notification system (G4) and reported it to the NHC. On 15 January, the WMHC first stated that ‘limited person-to-person transmission cannot be ruled out’ (G11). However, on 20 January, the NHC confirmed that ‘person-to-person transmission and medical staff infection’ (G13) were taking place. This change regarding the risk of COVID-19 and the lockdown of Wuhan (I6) led to increased social panic. Numerous rumours and fake news stories were diffused via social media, which resulted in significant social disturbances, such as people panic-buying food and misusing medicine. In response to the public sentiment, the central government of China instructed local governments at all levels to ‘release information on COVID-19 in a timely manner’ (G27). The WMHC started to provide updates on new cases and the prevention efforts every day or twice a day. Meanwhile, beginning on 3 January 2020, China regularly shared information about the situation in Wuhan with the World Health Organization (WHO) and other organisations (I1). After 11 January, information was exchanged between the WMHC and the WHO daily (I3). The disclosure of information about the epidemic to the WHO in the early stages of the COVID-19 outbreak in Wuhan is thought to have benefited other countries, allowing them to make the necessary preparations for when COVID-19 reached their populations (Tedros Adhanom, cited in China Daily, 2020).

Event cluster of government notifications.
The second event cluster concerning public sentiment governance was related to the social concerns with medical staff infection (Figure 8). Particularly, the death of Dr Li Wenliang drew a lot of attention. On 30 December 2019, eight medical staff, including ophthalmologist Li Wenliang, who was working at the Central Hospital of Wuhan, shared information to friends via WeChat about a case of pneumonia of unknown cause, saying that ‘seven cases of SARS from South China Seafood Market have been confirmed’ (P2). On 3 January 2020, they were asked to sign a letter of reprimand (P4) on the suspicion that they were spreading inaccurate news. Unfortunately, Dr Li showed symptoms of pneumonia on 10 January (P9) and passed away on 7 February (P37). This provoked widespread public criticism and negative comments about the Wuhan government. This was later reported by international news outlets such as the BBC and CNN. In responding to public concerns, the central government of China sent a team to Wuhan to conduct an official investigation into issues related to Dr Li (I9). On 19 March, the Wuhan police announced the result of the investigation, revoked the reprimand order against Dr Li, apologised to his family and punished the officials responsible for their improper treatment of the warnings delivered by Dr Li and his colleagues (P45). On 28 May 2020, the central government proposed to ‘improve mechanisms for direct reporting and issuing early warning about infectious diseases’ at the Third Session of the 13 National People’s Congress (G32). The proposition stated that it is necessary to strengthen the early warning systems used in emergency governance by increasing protections and rewarding ‘whistleblowers’. This event cluster indicates that public sentiment drove the progress of the urban response on different levels. People’s concerns about the suffering and pain caused by the pandemic ultimately promoted long-term advances in the system and the relevant laws.

Event cluster of medical staff infection.
Discussion and conclusion
The outbreaks of several infectious diseases in modern urban societies (such as SARS, H1N1 and currently COVID-19) had a significant impact on all aspects of people’s lives. Though several approaches have been established regarding the geography of epidemiology and the political ecologies of health and disease (PEHD) (Ali and Keil, 2008; Connolly et al., 2017), there are currently limited theoretical instruments available for directing urban responses to the outbreak of COVID-19. While the existing literature tends to emphasise the integrated urban governance strategies underpinned by top-down administrative systems (Shaw et al., 2020), it still remains unclear how cities like Wuhan were capable of taking effective countermeasures on a city level to deal with the outbreak of COVID-19 and solve the crisis.
This article employs an organisational approach, using EST to carry out a systemic event analysis of what happened in Wuhan from the emergence of the first case of COVID-19 on 1 December 2019 to the final moment when the pandemic was brought under control on 13 June 2020. A frame of event system analysis of urban epidemic governance was established to explore the causality and mechanism for numerous incidents related to the outbreak and control of COVID-19 in Wuhan. The event system analysis separated the response mechanism to COVID-19 in Wuhan into four categories: the graded response systems, the interactive relationship between multi-level entities of epidemic governance, the quarantine regulations and the governance of public sentiment.
First, a graded response mechanism was critical for Wuhan in implementing timely restrictions of the population’s mobility and providing medical treatment for infected patients. However, to trigger a graded response mechanism, coordinated interactions were needed between top and bottom entities. Many scholars have emphasised the efficiency of top-down administrative systems in coordinating stakeholders and allocating aid sources efficiently (Hesse and Rafferty, 2020; Wilkinson et al., 2020). To amend this view, we added that the down-top transmission of information is equally important in the beginning stages of the recent outbreak during which professional groups played a key role in preventing the spread of COVID-19 in Wuhan.
Second, a set of quarantine regulations was an important but complicated measure for preventing the spread of COVID-19. These regulations required substantial support from different social entities, ranging from medical institutions to communities, the public and enterprises. Without this varied support, social contradictions and confusion would have resulted. The event system analysis in this article indicates that Wuhan had been in the process of refining its quarantine regulations since the early stages of the pandemic. These regulations involved a strict quarantine policy in hospitals, including building several temporary hospitals to ensure that all infected patients were isolated from others and treated effectively. To prevent the spread of COVID-19 to other regions, the city underwent a strict lockdown for 76 days. During this time, local governance by communities, neighbourhoods, social organisations and volunteers (which were all tightly coordinated with each other) was vital. Additionally, material and technical support from businesses and social donations were essential for maintaining the quarantine regulations. In particular, new technologies such as mobile tracking were widely applied to identify asymptomatic patients. The health code measures were later employed nationwide as a regulation to prevent the spread of COVID-19 in China.
Third, the Wuhan case study suggests that the governance of public sentiment was indispensable to easing social panic and fostering corrective action during the COVID-19 crisis. A transparent and timely notification system was essential for quelling rumours and negative sentiments during the pandemic’s peak. The information about daily increases in cases, where cases were clustered, high-risk locations, new evidence and indications about transmission helped Wuhan citizens to protect themselves while also providing information to other people around the world. Furthermore, paying close attention to public sentiment helped to correct the behaviour of government entities, leading to the amendment of the whistleblowing law.
Lastly, this article provides valuable lessons for cities around the world that are struggling with the ongoing spread of COVID-19, but not every measure of epidemic governance used in Wuhan is transferrable to other cities. This is because of differences in the cultures, social-political systems and physical environments of China and other countries. Even in countries where there was a successful response to the pandemic (such as China, South Korea and Vietnam), the strategies of urban epidemic governance differed greatly. China, for example, has high levels of governmental control and employed new technologies to identify infected cases in the initial stage of the outbreak of COVID-19. By contrast, South Korea relied on experts to establish an integrated national plan and share information with all the departments involved in the pandemic response (Shaw et al., 2020). Some countermeasures adopted in Wuhan (and other Chinese cities) such as strict quarantine might not be suitable in other cities like London where housing (particularly in deprived areas) tends to be post-industrial, dense and ethnically diverse with little social cohesion. In these and other cities where the political pattern is polycentric, there might be sharp social resistance and even violence against emergency measures like lockdowns. The gated communities and highly concentrated management systems in neighbourhoods in Chinese cities presented an advantage when it came to implementing effective community isolation. There is also the concern about privacy when it comes to new technologies used to track the mobility of citizens. This is strictly protected by the legal systems in western societies. Furthermore, there might be challenges in the governance of public sentiment in multicultural regions where people speak different languages. In these places, it may be more difficult to disseminate authoritative information to the public than it is in China. Therefore, the ‘Wuhan experience’ of COVID-19 is an important reference point for urban governance, but it should not be simply replicated in other cities because each city will have to consider a variety of local factors. Finally, we propose a future research agenda on urban epidemic governance that might be more fruitful for incorporating both the coordination mechanism of multilevel organisations (as explored by this article) and individuals’ attributions and emotional responses to the pandemic (see e.g. Eberly et al., 2013; Greening et al., 2002).
Supplemental Material
sj-docx-1-usj-10.1177_00420980211064136 – Supplemental material for Urban epidemic governance:An event system analysisof the outbreak and controlof COVID-19 in Wuhan, China
Supplemental material, sj-docx-1-usj-10.1177_00420980211064136 for Urban epidemic governance:An event system analysisof the outbreak and controlof COVID-19 in Wuhan, China by Jinliao He and Yuan Zhang in Urban Studies
Footnotes
Acknowledgements
We wish to express our sincere acknowledgement to the anonymous reviewers and the editors of this Urban Studies special issue on COVID-19.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research was financially supported by National Natural Science Foundation of China (NSFC, No. 42171214), Fundamental Research Funds for the Central Universities (2019ECNU-HWFW003), and Youth Foundation of Social Science and Humanity, China Ministry of Education (20YJC790182).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.