
Abstract
Concepts of choice are often drawn upon within sexual health promotion discourses to encourage young people to take “responsibility” for and promote their own sexual health and reproductive control. A systematic literature search using predefined inclusion criteria identified peer-reviewed articles focusing on sexual health interventions for young people. Discourse analysis was used to interrogate how concepts of choice were articulated or inferred within the interventions. Of the eligible studies (n = 30), 16 were based on theories of behavioral change, suggesting a linear pathway between choice and improvements in sexual health. Studies that accounted for contextual factors were a minority (n = 6). Overall, study reports offered a limited account of the “situatedness” of young people’s opportunities to exercise choice. This reliance had a tendency to position young people as passive recipients of interventions which seemed to undermine the more active notion of “making choices” presented within these frameworks.
Introduction
Concepts of choice are often drawn upon within health promotion discourses to encourage people to improve their own health (see for example, Department of Health [DH], 2004; Wight & Abraham, 2000). UK health-related policy Choosing Health (DH, 2004) and, more recently, Equality and Excellence: Liberating the NHS (DH, 2010) draws attention to the notion of “healthy choices” in an effort to support and promote young people’s health.
U.K. sexual and relationship education (SRE) guidance and the Canadian guidelines for sexual health education further outline objectives to increase young people’s informed choices to encourage behavior change, delay sexual activity, and avoid unplanned pregnancy (DfEE, 2000; Public Health Agency of Canada, 2008). The extension of the concept of choice to the realm of young people’s sexual health has been guided by risk-reduction frameworks which draw particular attention toward young people’s “risky” health behaviors and negative health outcomes, including unplanned pregnancy, sexually transmitted infections (STIs), and HIV. Within these frameworks, promoting individual choice is depicted as an effective form of health protection whereby young people enact informed choices to guard against potential health risks stemming from their high-risk behaviors (Kotchick, Shaffer, Forehand, & Miller, 2001; Public Health Agency of Canada, 2008). This emphasis on individual characteristics and behaviors is a classic, and often criticized, public-health approach. Geoffrey Rose (2001) highlighted the limited effectiveness of targeting individual high-risk behaviors as a means to improve overall population health. By positioning individual choice as the key to improved outcomes across this large and heterogeneous group, these frameworks can be seen to enact the individual/population fallacy.
Other theorists have described this individual versus population issue in terms of compositional and contextual factors (see MacIntyre, Ellaway, & Cummins, 2002). Compositional factors capture individual behaviors and characteristics, whereas contextual factors describe the features in the socio-physical environment that work against health (MacIntyre, Ellaway, & Cummins, 2002). Each group of factors has a unique effect on individual and population health outcomes, but also intersect at multiple axes to shape and affect experiences of health. These theories often form the cornerstone of arguments advocating for a greater consideration of the wider social determinants of health within public health interventions.
Choice and its Links to Young People’s Sexual Health
Much recent literature in the field of sexual health promotion depicts an oversimplified and rather linear pathway between young people’s choices and improved sexual health outcomes (DfEE, 2000; DH, 2004). This pathway presents a simple cause–effect relationship between poor choices and negative outcomes (e.g., STIs, unplanned pregnancy). The young person is then situated as “unable” to make healthy choices because she/he has a deficient personality, character or suffers from low self-esteem (Shoveller, Johnson, Langille, & Mitchell, 2004). However, this cause–effect explanation does not account for the potential significance of the wider social contexts and determinants of health within which young people develop and make health-related choices (Aggleton & Campbell, 2000; Goldenberg, Shoveller, Koehoorn, & Ostry, 2008a, 2008b; Shoveller et al., 2004; Tolman, 2003), including the potential ways young people’s “choices” are structurally and socially conditioned and shaped (Fine, 1988; Fine & McClelland, 2006).
For example, work by Goldenberg and colleagues (2008a) points to the particular vulnerabilities experienced by young people as a result of their location within a unique social setting, characterized by high income levels and a transient male workforce. These characteristics coupled with gender, age and other determinants of health, structure young people’s choices in this setting and exposed some of the broader social factors that shape individual choices. Feminist literatures on sexuality and young people and, in particular young women, highlight the more complex nature of young people’s choices, specifically the ways in which choices are embedded within complex social, contextual and cultural meanings of sexuality, masculinities and femininities (Devries & Free, 2010; Fine, 1988; McClelland & Fine, 2008a; Shoveller et al., 2010; Tolman, 2003, 2006). These differing meanings are themselves situated within gendered power relations which come to define not only what choices are available, but also what choices are deemed “acceptable” for young women and men to take up (Connell, 2011; Doull & Sethna, 2011). In contrast, individualistic approaches to sexual health interventions underscore (and often blame) the individual compositional characteristics of young people for their poor outcomes, while failing to account for population level contextual explanations.
Issues of sex and gender provide illustrative examples of both the intersections and unique contributions of contextual and compositional factors. Sex (biological) and gender (social) highlight how compositional characteristics of individuals overlap and intersect with contextual factors of societies. For instance, an individual has a sex (male, female, intersex), yet the expectations of this sex manifest in one’s gender which is structured by the context within which the individual lives. For example, young men have been found to be less likely to present for STI testing because of their sex (compositional) and the discomforts involved in some testing processes, but also because of their gender (contextual) which socially shapes expectations of their behaviors and can physically shape access to testing sites. Furthermore, a young woman may be at greater risk of contracting a STI because of her biological sex and the ways in which her socio-physical context shapes the expectations of her gender in relation to her male peers. Here, both compositional and contextual aspects of sex and gender can be seen to influence the range of choices that are available and acceptable for young women and men. Pressures to conform to rigid norms of heterosexuality have been further linked to negative sexual health outcomes (Holland, Ramazanoglu, Sharpe, & Thomson, 1998; Tolman, 2006; Wingood & DiClemente, 2002). This evidence suggests that young people’s own wishes and desires are often compromised as they attempt to enact more “acceptable” choices that align with these dominant norms (ibid)—contributing to the now growing body of feminist and masculinities literatures that highlight the ways in which heterosexuality structures choices for young men and women (Allen, 2003; Forrest, 2010; Hill, 2006; Jackson & Cram, 2003; Rich, 1980).
Examining these literatures reveals the limited range of possible choices offered to young men and young women and points to the paternalistic intentions embedded in much sexual health promotion. For example, young people’s choices are often proscribed and even denied on the basis of adult assumptions about young people’s (sexual) immaturity and inability to make “healthy” choices (Spencer, Maxwell, & Aggleton, 2008). These protectionist notions are variously applied for young men and women and condition both the range of choices available for young people and the instances when they can be seen as being capable of making informed decisions. Michelle Fine’s (1988) seminal article on the “missing discourse of desire” illustrated how a focus on individualistic factors within sex education may actually exacerbate the vulnerabilities experienced by young people and, more specifically, deny young women’s sexual subjectivity and opportunities to make embodied choices in their sexual lives. Taking these arguments forward, McClelland and Fine (2008b) further emphasize how young people’s sexual health choices (at least within the U.S. context) are constrained by official health discourses and related policy and abstinence-based education programs.
Research by Spencer (2008) also reveals how young people’s opportunities to make choices are often constrained on the basis of concern about young people’s “risky” health behaviors, such as unprotected sex. Here, denying young people choice can be seen to be set within a discourse of caring and concern about young people, while failing to acknowledge that the assumptions embedded here include the notion that young people tend to make “bad” or “wrong” choices. This fails to account for the potential multiple meanings young people give to their health-related practices and how, in turn, choices concerning those practices are themselves socially and structurally conditioned and located (Spencer, 2008, 2011; Tolman, 2006).
Against this background, the aim of the present article is to examine the concept of choice in the literature on sexual health interventions for young people with a close focus on how issues of gender /sex are analyzed, discussed and presented within this body of literature. In particular, the article seeks to unpack how the concept of choice is presented and implied as a mechanism through which to improve young men’s and women’s sexual health outcomes. This analysis brings to the fore some of the assumptions inherent within dominant discourses on young people’s sexual health and how the concept of choice can be seen to contribute to these understandings.
Method
A systematic literature search was conducted to identify articles detailing interventions designed to improve young people’s sexual health outcomes. Studies were eligible for inclusion if they focused on young people between the ages of 12 to 24 years and assessed behavior change interventions (for example, behavior, knowledge or attitudinal change) to improve sexual health outcomes. Sexual health outcomes included, but were not limited to, issues of sexually transmitted infections (STIs), abstinence, pregnancy (unplanned), and HIV infection. The search focused on articles indexed in the following electronic databases: Medline, HealthStar, Cumulative Index to Nursing and Allied Health Literature (CINAHL), PUBMED, EMBASE, and PsycINFO. The following terms, and their various derivatives, were included in the search strategy and modified to suit each database: choice, sexual behavior, behavior change, sex education, interventions, adolescent. MeSH headings for key terms such as adolescent, young adult and sexually transmitted infections were used, as were Boolean operators (e.g., or/and) to combine derivatives of concepts (e.g., choice behavior or behavior change). Search results were limited to articles published in English between 2000-2010. To determine study inclusion, titles and abstracts of retrieved articles were assessed by two authors (Spencer & Doull). Studies that did not describe an intervention or assessed baseline knowledge or behaviors were excluded, as were those that focused on adult populations.
Method of Analysis
Information on study purpose, design, population, the intervention, outcome measures, and context was extracted and summarized for all included studies. Studies were grouped according to similarities in approach or intervention for comparison. The information on each study was detailed and guided the discourse analysis of reviewed articles. Discourse analysis is a method of analyzing text through recognizing the social constructed and situated meanings of that text (Bryman, 2004). These socially constructed meanings reveal the processes through which knowledge is effectively constituted as being “truth.” The approach to discourse analysis in this article sought to uncover the ways in which text produces and reproduces a particular set of gendered meanings, knowledge, and beliefs concerning men and women and their health-related practices. Feminist theorists (see Martin, 1991) have highlighted the ways in which the public-health literature creates and reinforces dominant stereotypes of women and men, which, in turn, produce and reproduce the socially constructed expectations of young women and young men (Braun & Gavey, 1999). This literature reveals why discourse analysis is an important tool to bring to the fore many of the gender-based assumptions that circulate and which are often perpetuated in the research literature itself. These assumptions are often implicit, but act to create meaning and, in the case of young people, often unfairly position them as risky and reckless individuals. This approach to the analysis further helps to uncover the potentially multiple meanings attached to concepts of choice, providing a more nuanced analysis of the normative assumptions about sex and gender that come to be produced and reproduced through discourse. For transparency, the results that follow indicate how often, and in what forms, the notion of choice(s) are used and implied in the articles.
Results
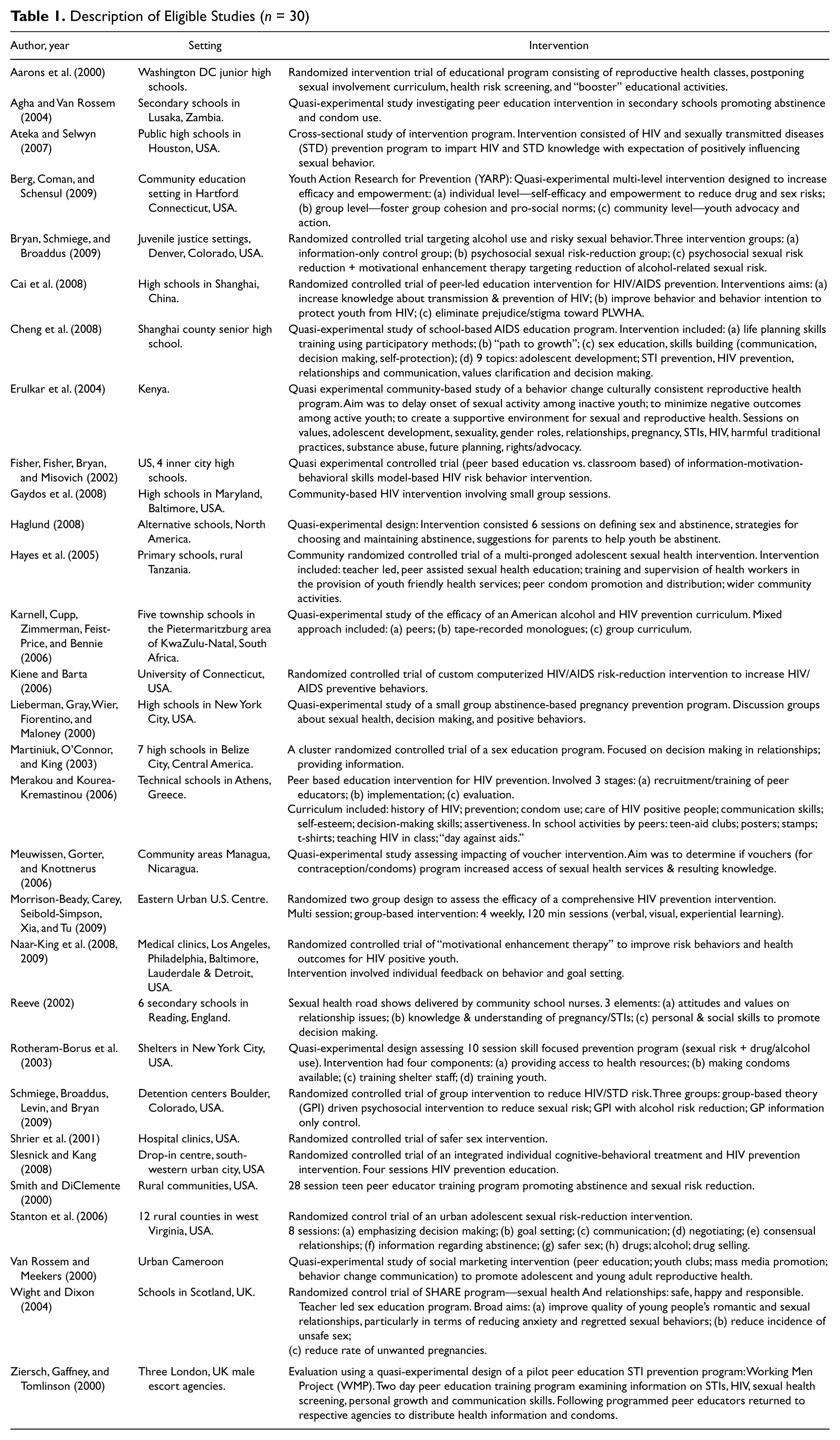
A total of 30 studies met the inclusion criteria for the review and were analyzed in detail. Table 1 provides a summary of each study intervention. The majority (n = 22) of studies reviewed did not explicitly refer to the term choice (exceptions included Haglund, 2008; Karnell, Cupp, Zimmerman, Feist-Price, & Bennie, 2006; Lieberman, Gray, Wier, Fiorentino, & Maloney, 2000; Morrison-Beedy, Carey, Seibold-Simpson, Xia, and Tu 2009; Naar-King et al., 2009; Schmiege, Broaddus, Levin, & Bryan, 2009; Stanton et al., 2006; Ziersch, Gaffney, & Tomlinson, 2000). Studies explicitly referring to the concept of choice relied on discourses that linked increased knowledge of sexual health to young people’s abilities to enact healthy sexual decision-making—implying a linear pathway between knowledge and healthy choices. These explanatory linear pathways are common in public-health literatures that draw upon positivist epistemologies and methods of enquiry (for example, measurable phenomena, randomized trials) and have been routinely criticized for their lack of attention to contextual factors (Glass & McAtee, 2006; Raphael & Bryant, 2002). For example, as illustrated in the excerpts below, interventions often underscore the importance of imparting knowledge, something that is easy to measure and track across time, without due consideration of the context in which such knowledge is created and enacted. Choosing abstinence, for example, is not just dependent upon awareness of this option but is complicated by personal, relational, and social factors (Ott, Pfeiffer, & Fortenberry, 2006).
Description of Eligible Studies (n = 30)
The data indicate that girls in the intervention group intended to limit their sexual behaviors to choices less risky than intercourse, whereas girls in the control group indicated they were less likely to limit such behaviors. These responses reflect a benefit of the abstinence plus approach, that is, teaching harm-reduction strategies to use when faced with potential sexual behavior (Morrison-Beady et al., 2009, p. 579). The curriculum was developed to change negative perceptions and to help participants view abstinence as a reasonable and positive way to reduce sexual risks (Haglund, 2008, p. 654).
16 studies were informed by theories of behavioral change, in particular the trans-theoretical stages of change model (Prochaska & DiClemente, 1983) and the theory of reasoned action (Fishbein & Ajzen, 1973). These studies focused on healthy sexual behaviors defined and constructed as being abstinence, secondary abstinence, and increased intention to use condoms. Implicit within these discourses, and their choice of behavioral outcomes of interest, was the underlying assumption of young people as risky and “in need” of protection. Little account of young people’s own parameters and meanings of healthy or risky choices were given in the articles reviewed and, instead, heavily relied on traditional developmental frameworks.
STAND (Students Together Against Negative Decisions) is also designed to be consistent with our knowledge of the developmental characteristics of teenagers, including perceived unique invulnerability, limited abstract reasoning ability, and a predilection to focus on present rewards over long term consequences (Smith & DiClemente, 2000, p. 442).
Although many studies (n = 18) reported increases in participants’ knowledge of sexual health, the effectiveness of these interventions to change sexual health practices of young people was reported to be limited. In accounting for the limited effectiveness of interventions, articles focused on limitations of study design (n = 7), sampling limitations (n = 11), difficulties of long-term follow-up of behavior change (n = 10), and young people’s (in)abilities to respond to health-related messages conveyed in the intervention (n = 10) and in particular, their assumed susceptibility to peer influence (n = 5).
No evidence was found of an increased use of abstinence in regular partnerships or of changes in condom use. This may reflect weaknesses in the design of the intervention: active learning methods were not used to teach adolescents’ negotiation skills for abstinence or condom use (Agha & Van Rossem, 2004, p. 451). Furthermore, the lack of significant outcomes among the students who were already or who became sexually active suggests that these students are an especially challenging group, whose needs may not be met within the context of an abstinence-focused, school-based program (Lieberman et al., 2000, p. 244).
A fifth of studies (6/30) included reference to structural or contextual explanations for the success or failure of the intervention. These exceptions alluded to potential effects of socioeconomic factors and gender relations. However, these articles emphasized the compositional or individual nature of these factors, rather than their contextual or population level impacts. Issues of gender, when present, focused on methodological “techniques,” most often issues of randomization, quantifying the gender composition of study samples (to indicate sample representativeness for purposes of generalizability), and/or confounder control. These articles treat gender as a categorical, rather than relational unit of analyses (see Connell, 2011, p.1). For example, gender was primarily mentioned in reference to the equivalency between groups after randomization. The term gender seemed to be used in place of the term sex—often in inappropriate ways. For example, studies reported gender-disaggregated analyses when they reported outcomes separately for males and females. This approach effectively equates gender with the statistical differences between the categories of male and female (Connell, 2011).
In other studies, female participants were often absent as authors’ discussed progress according to the “standard” male subject and by reporting participants as “percentage male.” Other studies presented gender as a contextual factor, citing literature which has shown differential effects related to societal gender norms as justification for sex-disaggregated data (n = 5). However, the subsequent analysis was not accompanied by discussion of the significance of gender to study findings, except for the occasional call for “gender-specific” interventions (see Aarons et al., 2000; Martiniuk, O’Connor, & King, 2003; Slesnick & Kang, 2008).
In some cases (for example, Shrier et al., 2001), the concept of choice was implicitly contextualized by gender. For example, young women were asked about condom use negotiation, rather than condom use alone. This example emphasizes the contextual and relational nature of gender and the ways in which context intersects with gender to shape the choices available to young men and women. Contextual discussion of gender relations was rare; more often positivist discourses described gender as a confounder—a factor that interrupts the linear pathway thereby necessitating control.
Study descriptions appeared to position young people in two main ways. First, some studies (n = 7) identified “at risk” or “risky” groups of young people, including special populations such as young men who have sex with men, drug users, haemophiliacs and young people living in the care or youth in the justice system. These “special” populations were identified as being at particular risk for negative sexual health outcomes and/or likely to make (predefined) ill-informed decisions and thus, characterized as being “in need” of intervention to correct their problematic behaviors.
Interventions among criminally involved adolescents are critical because of high-levels of sexual and alcohol behaviour . . . intervention can be effective in promoting behaviour change (Bryan, Schmiege, & Broaddus, 2009, p. 1186).
Second, reviewed studies often constructed young people as being passive recipients of sexual health related knowledge. Young people’s lack of knowledge and awareness of the consequences of unprotected sex were highlighted, emphasizing particular deficits in participants’ knowledge and behaviors to enact healthy decision-making. Young people’s own knowledge of, and the meanings they ascribe to, sexual health—including the factors they themselves see as contributing to their sexual health practices and outcomes were not reported in study designs or integrated into the interventions.
Discussion
The explicit and implied uses of the concept of choice in articles reviewed can be seen to contribute to the construction and reproduction of dominant discourses surrounding young people’s sexual health. In particular, this review of sexual health interventions for young people revealed the primacy of theories of behavioral change approaches, with limited account of some of the structural and contextual factors that have been shown to effect sexual health outcomes for young men and women (Goldenberg et al., 2008a, 2008b; Marston & King, 2006; Shoveller et al., 2004; Singh et al., 2001). Implicit within these behavioral change frameworks is the assumption that increases in knowledge lead to behavioral and attitudinal change and thus, depict a relatively linear pathway from choice to positive sexual health decision-making and healthy outcomes. These articles often implied a single notion of choice, thereby downplaying the potentially multiple meanings and choices available to young people. The absence of attention toward issues of structure and context in the design and related discussion of such interventions raise a number of implications for sexual health promotion for young people.
First, absence of structural and contextual factors in the design, implementation, and discussion of results had a tendency to locate the limited effectiveness of interventions within young people’s assumed deficiencies and their lack of ability to respond to health-related messages. Not only does this absence of context fail to acknowledge the potential ways in which factors such as socioeconomic position and gender condition young people’s experiences of sexual health, such approaches appear to render young people to a position of incompetence and incapability. In this way, these interventions can be seen to contribute to and reinforce traditional (negative) developmental discourses about young people.
This deficit approach fails to acknowledge the ways in which social context and gender differentially shape and determine various choices available to young men and young women and their opportunities to implement these choices. This approach is reminiscent of the much criticized “victim-blaming” discourse (Ryan, 1976) that has been prevalent in the health promotion and public-health literature for decades. The protectionist discourses present in the interventions reviewed appeared to magnify this blame the victim discourse by positioning young people as passive, yet actively at risk.
For example, interventions typically presented young people as passive recipients of sexual health knowledge and, in doing so, downplayed the saliency of young people’s own understandings and experiences of sex and relationships in guiding their sexual health practices (cf. Fine, 1988; McClelland & Fine, 2008a, 2000b). Rendering young people as passive recipients of knowledge, with little account of how young people themselves define and understand their own sexual health, is arguably set against the stated intentions of many interventions which suggest young people should actively make sexual health choices. Although intervention studies appeared to construct young people as passive recipients of knowledge, studies simultaneously charged young people with the responsibility to act as active agents when exercising choice. This somewhat contradictory position inherent within these types of interventions gives little room for young people to assert their own choices (or indeed, indicate any potential ambivalence toward “making choices,” cf. Tolman, 2003) and arguably positions them as blameworthy when interventions fail.
The articles included in the present review also position sex as a variable that can be controlled and measured. Dispersed through the articles was the term gender, which was often used incorrectly in place of sex; for example, analyses were referred to as gender disaggregated. Without any contextualized discussion of gender, or the sociocultural distinctions between men and women, it is inappropriate to refer to this type of analysis as gender-based (Spitzer, 2007). This example points to the ways in which more contextualized terms are taken up without changes to the underlying discourse, which remains compositional in nature. In these cases, the term gender is used in place of sex and the underlying assumptions about sex as a homogenous factor that can be measured and randomized remain. Connell (2011) points to the fallacy in this categorical thinking about gender which focuses simply on differences between men and women and points to the need to understand gender as a relational construct which may provide a more nuanced appreciation of the complex ways in which gender comes to define and shape health practices and outcomes—and the multiple choices these gendered norms come to produce and validate as being “acceptable” social truths.
In contrast, some articles accounted for gender and the norms that accompany gender in a more meaningful way. For example, these articles recognized that gendered power dynamics in heterosexual relationships render the outcome of condom use somewhat less meaningful for young women than young men and that condom use negotiation was a more appropriate outcome to address young women’s unique gendered roles in relationships. These two distinct outcomes are highly meaningful and work to shift discourses of individual responsibility which often stem from the poor performance by young women or young men on gender-specific outcomes.
Furthermore, an oversimplified linear pathway from choice to health says little about the potentially different kinds of choices available to young men and women. For instance, opportunities for young women to assert choice might be heavily guided by dominant norms of femininity which have a tendency to promote the passivity of women in sexual relationships and correspondingly construct assertive women as sexually promiscuous (Curtin, Ward, Merriwether, & Caruthers, 2011; Doull & Sethna, 2011). Submitting to their partners’ choices might be the only “choice” available to some women, illustrating how the notion of choice within the context of sexual relations is set within complex gendered power relations (Holland et al., 1998). Like gender, concepts of choice must therefore be understood as relational and context specific which opens up possibilities for how interventions might be developed to challenge and subvert gendered power relations and dominant discourses surrounding young people’s sexual health. If choice is understood as a singular, individualized and decontextualized pathway from knowledge to action, young people will continue to be positioned as personally responsible for their failure to choose effectively.
Shifting discourses of individual responsibility is essential given the noted trend of attributing the limited effectiveness of interventions to young people’s failure to respond to health messages and act accordingly. This attribution of blame highlights the distinction studies implicitly made between choice as a noun and that of a verb—both of which were effective in downplaying the “situatedness” of young people’s opportunities to exercise choice and effectively positioned young people as passive in their sexual relationships. For example, in predefining positive sexual health choices as abstinence, delayed sexual activity or condom use, studies constructed a set of pre-given choices which effectively limited the possible range of choices available to young people and devalued alternate choices. The construction of choice as a noun implies a realist ontology, thereby limiting exploration of the potentially diverse and highly gendered meanings young people might actively give to multiple choices and the ways in which young people construct their own and potentially differing understandings of choice in their sexual relationships.
Similarly, although exercising choice might implicitly suggest and support the agency of young people, the emphasis on young people’s inabilities to act in particular prescribed healthy ways again located the limited effectiveness of interventions in young people’s failure to succeed in the context of the intervention. Through constructing choice as a verb, studies reviewed effectively individualized and decontextualized the pathway from choice to health, with a tendency to further problematize, rather than promote, young people’s sexual health.
Conclusion
A review of sexual health interventions aimed at promoting sexual health for young people revealed how notions of choice are drawn upon (or implied) to reproduce a set of dominant gendered discourses about young people’s sexual health. When continually repeated, discourses begin to become codified and act to create, structure, and reinforce reality. In sexual health intervention research and practice, discourses influence what questions are asked, what methods are used, and what populations and outcomes are targeted. Importantly, discourses are context specific and are imbued with historical meanings.
Despite the emergent discourses uncovered in this review, it is important to highlight a number of limitations to the analysis and consider their bearing on the overall quality of the review. First, this review focused only on the peer-reviewed literature. Examining other publications (e.g., grey literature) may have uncovered differing perspectives. In part, this could be attributed to the search employed, including the inclusion/exclusion criteria, in addition to potential differences in electronic indexing. Likewise, study reports themselves often differed in their accounts, with some articles excluded on the basis of limited reporting. These exclusions may have illuminated a different perspective on young people’s sexual health.
The systematic approach taken in this review sought to comprehensively identify how the notion of choice was constructed and produced within the articles included in our review, thereby illuminating how varying discourses of choice were produced and reproduced (and how those discourses are embedded in particular ontological orientations). Conducting a review of this kind reveals some of the theoretical and methodological challenges that emanate from interdisciplinary scholarship and provides an illustration of how various paradigmatic approaches can be combined to strengthen these forms of analyses.
Furthermore, unearthing and challenging these discourses allows researchers to further understand the relative successes and challenges of interventions and may offer opportunities to reshape knowledge around a particular issue or population. Importantly, research suggests that young people themselves begin to take up and embody discourses that position them as risky and unhealthy (Shoveller et al., 2004; Shoveller & Johnson, 2006; Spencer, 2011). In this way, a cycle is created wherein research and intervention in sexual health reinforce and reinscribe perceptions that “bad things” (STIs, unplanned pregnancies) “happen to bad people” (Shoveller et al., 2004, p.484). To move forward, research and practice in sexual health promotion needs to acknowledge the wider contextual factors that affect young people’s opportunities to exercise so-called healthy sexual choices. By doing so, future interventions should tap into young people’s own experiences and perspectives on sexual health to better support young people negotiate their relationships within the structural and contextual realities of their everyday lives.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr Doull is supported by a Postdoctoral Research Fellowship from the Canadian Institutes of Health Research.