
Abstract
Adolescent health has a significant influence as individuals transition to adulthood and can have lifelong effects on well-being. In addition to well-established structural determinants of health such as racism and poverty, proximal determinants of adolescent health illuminate on the health effects of the daily circumstances of adolescents. Guided by the proximal determinants of adolescent health theory, we examined the association between adolescents’ self-rated health and multiple domains of proximal determinants, including family relations, peer relationships, school environment, and neighborhood environment. Using data from the Fragile Families and Child Wellbeing Study, we analyzed 3,444 adolescents who were 14 to 15 years old. Results of ordered logistic regression analyses revealed significant associations between proximal determinants and adolescents’ self-rated health even when taking into account all the domains simultaneously. This study highlights the importance of unraveling factors of multiple systems on adolescents’ health and suggests implications for their subsequent transition to adulthood.
Introduction
The social determinants of health framework represent a powerful paradigm that has guided countless research studies aiming to improve population health. According to this approach, health is substantially a function of complex and integrated structural determinants, including social environment, physical environment, health services, and structural and societal factors (Commission on Social Determinants of Health, 2008; Marmot et al., 2008). Social determinants reveal important mechanisms underlying health disparities. There exists a striking social gradient in health disparities, meaning that inequalities in population health status are related to inequalities in social status, including socioeconomic status, racial and ethnic background, and other factors (Marmot, 2015; Marmot & Allen, 2014). Social determinants are pervasive across the life span from birth to old age (Yang et al., 2016).
Although social determinants evolve within the life cycle and manifest themselves differently at various stages, there is a gap in the study of adolescence. Adolescents are frequently aggregated with either younger adults or with older children (Starfield et al., 2002; Viner et al., 2012). Yet adolescence is a period in the life cycle characterized by social conditions and factors that are unique to this developmental stage (Blum et al., 2012). How do social and environmental determinants manifest in various contexts for adolescents? Using a national sample, this study examines the effects of a set of multi-domain factors that are unique to the adolescent population.
An Imperative to Understand and Improve Adolescent Health
Adolescence is arguably among the most critical stages of human development as individuals transit from childhood to adulthood (Patton et al., 2016; Viner et al., 2015). This vibrant yet challenging period is marked with active brain plasticity, rapid pubertal maturation, and dynamic behavioral, relational, and social changes (Arain et al., 2013). Critical developments during adolescence suggest that the adolescent period is a sensitive yet critical stage for individuals’ later health and disease trajectory.
Bio-physiologically, many studies, including several systematic reviews, have revealed that physical well-being during adolescence is a powerful predictor for adulthood wellness in terms of cardiovascular disease (Twig et al., 2016), obesity (Rooney et al., 2011), cardio-metabolic risk (Schmidt et al., 2011), and morbidity and premature mortality in adulthood (Reilly & Kelly, 2011). For example, a longitudinal study (Magnussen et al., 2016) revealed that metabolic syndrome during adolescence significantly predicts adult type 2 diabetes. Similarly, a longitudinal study following 37,674 adults revealed that an evaluated body mass index (BMI) score in adolescence constitutes a substantial risk factor for obesity-related disorders in midlife (Tirosh et al., 2011).
In addition, adolescents’ psychosocial and behavioral health are significant correlates to their health status in adulthood. For example, depression and anxiety during adolescence are significant predictors of subsequent coronary heart disease in adulthood with studies reporting up to 2.17 hazard ratios (Janszky et al., 2010). In addition, low self-esteem during adolescence predicts adult depression two decades later (Steiger et al., 2014). It is important to gain a deeper understanding of adolescent health not only because adolescence is a critical stage during which key developmental milestones are occurring but also because adolescent health is among the most powerful predictors of individuals’ future health trajectory, morbidity, and mortality.
Proximal Social Determinants of Adolescents’ Health
To guide our investigative effort, we used the theoretical framework of the proximal social determinants of health proposed by Viner and colleagues (2012). Viner and colleagues (2012) conceptualized social determinants of adolescent health from two aspects: structural determinants and proximal determinants. Structural determinants refer to nationwide fundamental circumstances that create social stratification, such as national income inequality, educational disparity, racism, and sexual or gender norms that are universal for individuals of all ages. In contrast, proximal determinants of health are circumstances of daily life generated in family, peer, school, and neighborhood environments and establish individual differences in exposure and vulnerability to factors that compromise health among adolescents. While the category of proximal determinants of health may still apply to individuals at other developmental stages, adolescents are uniquely affected by these proximal social determinants that are distinct from their pediatric and adult counterparts (Currie et al., 2012; Herrenkohl et al., 2000). Those unique proximal determinants of adolescent health include family relations, school environment, peer relationships, and neighborhoods.
Family relations
Family, especially relationship with parents, is a well-established determinant of adolescent health (Berge et al., 2010). Although relationship with parents is important across an individual’s developmental spectrum, it affects adolescent health in a couple of ways. Effective parenting has a positive association with adolescent physical activity (Kirby et al., 2011), substance use behaviors (Luk et al., 2010), mental well-being (Branje et al., 2010), and the formation of social relationships (Pallini et al., 2014). In addition, relationship with parents is a salient protective factor for risky behaviors, like risky sexual behaviors (Deptula et al., 2010) and violent romantic relationships (Olsen et al., 2010). In addition, according to theories of parent–adolescent relationships, interactions between parents and adolescents include important tasks of psychosocial maturation: identity development and separation-individuation. In other words, critical identity development milestones are significantly influenced by transactions between parents and children, suggesting parent–child relationship during adolescence has far reaching and paramount implications for concurrent and long-term outcomes across developmental domains (Koepke & Denissen, 2012).
School environment
School is the primary social venue for adolescents and its significance to adolescent health is compelling. Many aspects of school environment, such as a sense of belonging, leadership development, and safety, affect adolescents’ health both directly (by changing the environment) and indirectly (by affecting their individual outcomes; Pittman & Richmond, 2007; Zhang et al., 2019). For example, studies have documented that school connectedness is predictive of adolescents’ adjustment, mental health, and life satisfaction (Loukas et al., 2009; You et al., 2008). In addition, school connectedness has been identified as a strong predictor of late teenage substance use, mental health status, and academic outcomes, all of which have significant implications for adolescents’ general health status (Bond et al., 2007).
Peer relationships
The emergence of strong peer relationships is one of the essential developmental features of adolescence and plays a vital role in adolescent health (Jaccard et al., 2005; Zhang et al., 2017). Positive peer relationships, like peer support, have been identified as a key indicator of adolescents’ physical activity which, in turn, promotes their general health status (Fitzgerald et al., 2012). In the same way, negative peer relationships, such as bullying, negatively affect adolescents’ physical and mental health well-being (Hager & Leadbeater, 2016; Sigurdson et al., 2015).
Neighborhood environment
As adolescents venture outside the home, the importance of neighborhood environment for their health increases (Viner et al., 2012). While a rich neighborhood environment provides opportunities to thrive, a lack of a supportive neighborhood environment has significant ramifications. Neighborhood deprivation has been associated with poor academic achievement (Nieuwenhuis & Hooimeijer, 2016), teenage pregnancy (Gaias et al., 2018), dissatisfactory mental well-being (Wickrama & Bryant, 2003), and increased violence among adolescents (Haynie et al., 2006). Adolescents residing in poor neighborhoods face severe health risks due to the lack of public infrastructure, poor living environment, and high level of violence, all of which are detrimental to their health status (Hurd et al., 2013; Ivert & Levander, 2014).
Gap in the Literature and the Present Study
Existing studies have examined proximal social determinants but typically separately, and few studies have evaluated these determinants simultaneously on the national scale specifically for adolescents. Lacking such investigation prevents a comprehensive evaluation of the ecology of proximal determinants of adolescents’ health. As a result, some important questions remain unanswered, such as “when all these proximal determinants are included in the same model, will their impact on adolescents’ health change?” To this end, using data from the Fragile Families and Child Wellbeing Study, we examined the association between proximal social determinants of health, including family support, school connection, peer relationship, neighborhood environment, and self-rated health among 14- and 15-year-old adolescents.
Method
Data Source
The Fragile Families Study is a national longitudinal, birth cohort study that uses a stratified random sample of all U.S. cities with 200,000 or more people and was initiated in 1998–2000. The sample was stratified in the first wave by 75% unmarried and 25% married families to obtain better understandings of unwed parents, especially unwed fathers and their children at the national level (Reichman et al., 2001). The study was a joint effort by Princeton University’s Center for Research on Child Wellbeing and the Columbia University Population Research Center. For our analyses, we drew on data from the 15th year follow-up (2014–2017). A total of 3,444 participants completed the Teen Survey, which represents 74% of the eligible participants in Year 15 and 70% of the participants at baseline. The detailed research methodology and sampling strategies for the Fragile Families Study have been reported elsewhere (Reichman et al., 2001). Our analytical sample included all 3,444 participants.
Measurement
Self-rated health
To determine self-rated health, adolescents were asked, “In general, how is your health?” based on a 5-point Likert-type scale ranging from poor = 1 to excellent = 5, with a higher score indicating better general health status (Lima-Costa et al., 2012; Miilunpalo et al., 1997). Using self-rated health as a measure of general health status has been recommended by the World Health Organization (Subramanian et al., 2010) and used in many empirical investigations (Assari, 2018; Zhang et al., 2019). Most importantly, in comparison with other single measure of physical health status like physician-rated health or body mass index, self-rated health has greater predictive validity in predicting individuals’ future disease trajectory and mortality (Schnittker & Bacak, 2014).
Studies suggest that self-rated health is a highly valid measure of an individual’s general health status for several reasons: (a) It is an inclusive measure which integrates individuals’ objective health characteristics and their subjective illness perceptions (Karademas et al., 2011), (b) it provides an informative evaluation that is based on the continuous monitoring of one’s health and illness history that is largely unavailable to a physician or other single health measures (Benyamini, 2011), and (c) it offers a dynamic assessment which reflects resources, including education, socioeconomic status, social relational support, all of which are validated correlates of an individual’s morbidity and mortality (Ruthig et al., 2011).
Family relations
Family relations were measured based on adolescents’ closeness with their father and mother. An adolescent’s closeness to their father was measured by their responses to the question, “How close do you feel to your dad?” Similarly, an adolescent’s closeness to their mother was measured by their response to the question “How close do you feel to your mom?” Responses to both questions were rated on a 4-point Likert-type scale ranging from not very close = 1 to extremely close = 4, with a higher score representing a higher level of closeness with the mother.
Peer relationships (operationalized by bullying)
The proxy measure for peer relationships that we used was the extent to which the adolescents experience bullying. Bullying was measured by how often in the past month they had encountered the following behaviors from peers in their school or neighborhood: (a) “picked on them or said mean things to them,” (b) “hit them,” (c) “took their things,” or (d) “purposely left them out of activities.” An adolescent reported from “never = 0” to “about every day = 4” for each of the four forms of bullying. The responses were added to form an index of bullying ranging from 0 to 16. This measure demonstrated satisfactory internal consistency with α = .99 for the study sample.
School environment
School environment was assessed with a 10-item scale reflecting adolescents’ perceptions of their teachers and peers’ emotional support. Adolescents responded to questions such as “The teachers in this school treat the students with respect” and “Kids in this school behave the way the teachers want them to” on a 4-point Likert-type scale ranging from strongly agree = 1 to strongly disagree = 4. The responses were reversely coded and then summed to form an index of overall school climate, ranging from 10 to 40, with a higher score representing a more positive school environment. This measure indicated satisfactory internal consistency α = .91.
Neighborhood environment
Neighborhood environment was measured using neighborhood collective efficacy, which is an eight-item scale reflecting adolescents’ perceptions of their neighborhood environment. The measure was developed by Sampson and colleagues (1997) and the Fragile Families Study team replaced one original item “people in this neighborhood can be trusted” with modified language: “people in this neighborhood generally don’t get along with each other.” Adolescents responded to a set of questions about informal social control, social cohesion, and trust in the neighborhood, including “People around here are willing to help their neighbors” and “This is a close-knit neighborhood.” The questions were presented on a 4-point Likert-type scale ranging from strongly agree = 1 to strongly disagree = 4. Six of the eight questions were reverse coded and then summed to form an index of neighborhood collective efficacy, ranging from 8 to 32, with a higher score representing higher neighborhood collective efficacy. This scale reported acceptable internal reliability with Cronbach’s alpha = .77.
Covariates
Five covariates were incorporated to estimate the base model, including adolescents’ sex (male = 0, female = 1), adolescent-reported race/ethnicity (African American, Hispanic, other non-Hispanic White or multi-racial, with non-Hispanic White used as the reference category), household income per member (US$20,000–US$39,999, US$40,000–US$74,999, US$75,000 or higher, with less than US$20,000 as the reference category), and primary caregiver’s education level (high school or equivalent, some college, and college or graduate degree, with less than high school as the reference category). A measure of adolescents’ physical health conditions was also included using a seven-item measure counting the occurrence of seven diseases, such as digestive allergy, eczema allergy, diarrhea, and so on. Adolescents responded yes = 1 or no = 0 to the statements such as “Youth had food/digestive allergy in the past year” and “Youth had eczema/skin allergy in the past year.” The responses were added to form an index ranging from 0 to 7, in which a higher score indicated a greater occurrence of physical health conditions.
Statistical Analysis
We used descriptive statistics to summarize the sample characteristics, with mean and standard deviation for continuous variables and frequency and percentage for categorical variables. We used order logistic regression modeling to evaluate the association between different proximal social determinants and adolescents’ self-rated health. Most variables had a minimal missing rate of 2.5% or lower except for adolescent-reported race (5.4%), relationship with father (17.6%), and neighborhood collective efficacy (7.9%). The result of Little’s MCAR test, χ2(325) = 363.87, p = .068, indicated missing completely at random. To address potential biases caused by missing data, we used multiple imputation with chained equations for all the variables in the study (Royston & White, 2011). Considering that some cities do not have weights and that no corresponding weights to address attrition were available in Year 15, we followed other published studies (Parkes et al., 2019; Pilarz et al., 2019; Schroeder et al., 2020) and controlled for variables that were used to create survey weights rather than apply the survey weights to the analyses.
Based on our regression model, we found that the assumption of proportionality of odds across response categories was violated, χ2(47) = 95.51,p < .001. To address this violation, we combined “poor,” “fair,” and “good” into one category and created a three-level variable (poor/fair/good, very good, and excellent). Applying the new variable in the model, we found that the assumption of proportionality of odds across response categories was satisfied, χ2(16) = 23.05, p = .11. All parameters from the ordered logistic regression were estimated based on 10 sets of imputed data using Stata 15 SE.
Results
Sample Characteristics
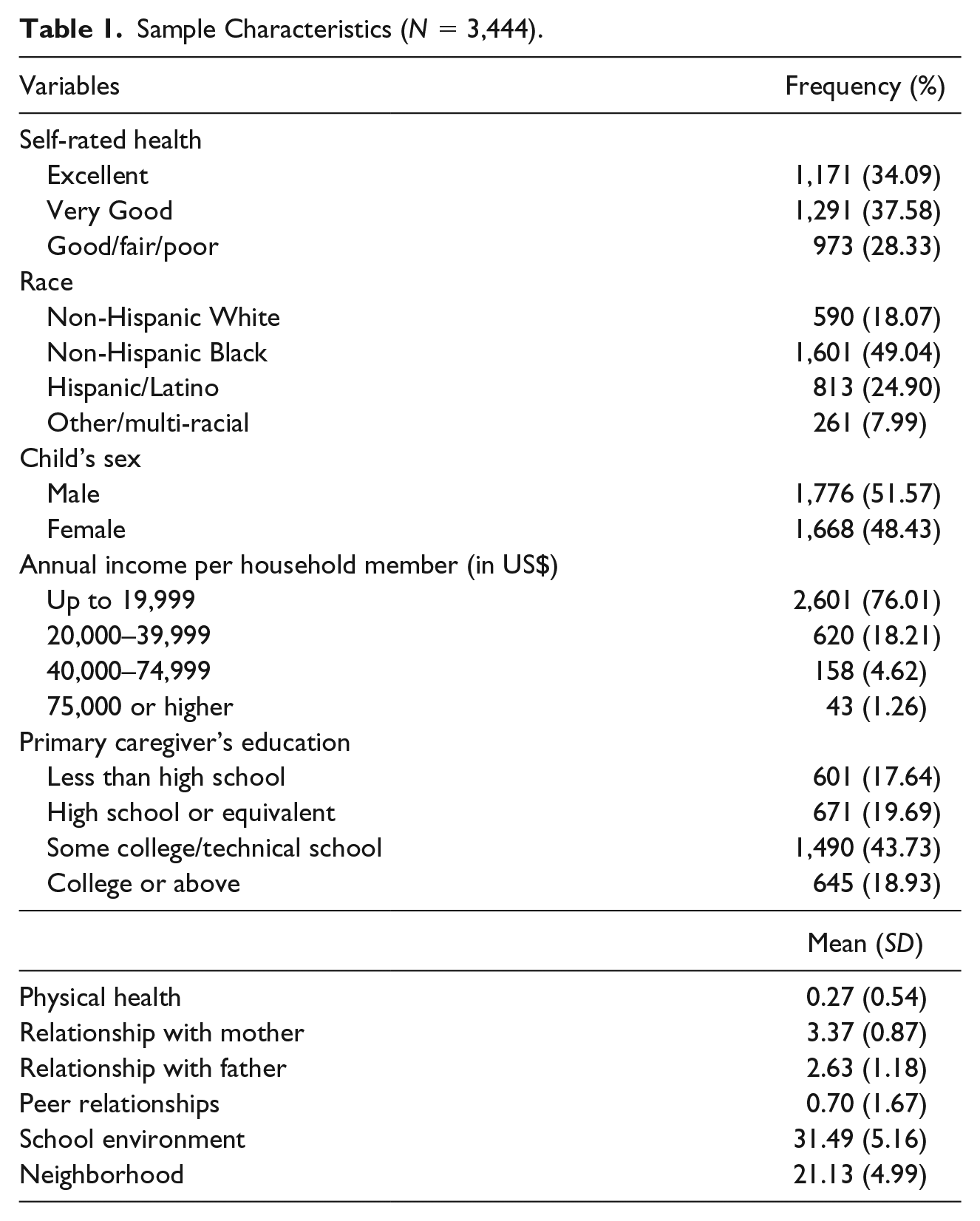
Table 1 presents sample descriptive statistics. Non-Hispanic Blacks and Hispanic adolescents, respectively, accounted for 49.04% and 24.90% of the sample. Females were slightly underrepresented (48.43%) relative to males. More than a quarter of households (76.01%) had a per-capita income below US$19,999. Among the primary caregivers, 43.73% had some college education or had earned a technical school degree and 18.93% had received a college degree or above. Those with less than high school and high school or equivalent made up 37.33% of the sample. The average number of adolescents’ physical health conditions was 0.27 (SD = 0.54). The mean of adolescents’ relationships with their mothers and fathers were, respectively, 3.37 (SD = 0.87) and 2.63 (SD = 1.18). The reported average of peer relationships was 0.70 (SD = 1.67). In terms of the perceived school climate, the adolescents indicated 31.39 on average out of 40 (SD = 5.16). The mean of reported neighborhood collective efficacy is 21.13 (SD = 4.99).
Sample Characteristics (N = 3,444).
Ordered Logistic Regression
Table 2 presents findings from the models estimating adolescents’ self-rated health as a function of all proximal social determinants of health in the model simultaneously. Results of the model suggest that female adolescents were less likely to report better self-rated health than were male counterparts (odds ratio [OR] = 0.65, p < .001). Other or multi-racial adolescents reported significantly better health than did non-Hispanic Whites (OR = 1.43, p < .01). Adolescents whose households had a per-capita income of US$20,000 to US$39,000 (OR = 1.22, p < .01) were more likely to report better self-rated health than did the lowest income group (<US$20,000). Finally, a greater number of physical health conditions was associated with a decreased self-rated health rating (OR = 0.82, p < .001).
Adolescent Self-Rated Health as a Function of Proximal Social Determinants of Health (N = 3,444).

p < .05. **p < .01. ***p < .001.
For proximal determinants of health, adolescents who have better relationships with mothers (OR = 1.29, p < .001) and fathers (OR = 1.14, p < .001) had increased odds of better self-rated health. For each unit increase in the quality of their relationship with mother and with father, the adolescent was 29% and 14% more likely to report a higher rank of self-rated health, respectively. In addition, experiencing peer bullying was associated with decreased odds of better self-rated health (OR = 0.92, p < .001). For each unit increase in being bullied, an adolescent was 8% less likely to report a higher rank of self-rated health.
With the school environment domain variable, a more favorable school climate was associated with increased odds of adolescents’ better self-rated health (OR = 1.04, p < .001). For each unit increase in perceived school climate, the adolescent is 4% more likely to report a higher rank of self-rated health.
Finally, a more favorable neighborhood collective efficacy perception was associated with odds of adolescents’ better self-rated health (OR = 1.02, p < .001). And notably, all proximal determinants of health were statistically significant, suggesting the robustness of each determinants’ unique contribution to adolescent health controlling for other determinants.
Discussion
Building on a robust body of literature on adult populations, our study showed how social and environmental determinants of health manifest themselves in contexts specific to adolescents. Our multi-domain analyses yielded significant correlates of all aspects of 14- and 15-year-old adolescents’ daily life on self-rated health. This suggests that each aspect of the adolescent’s social environment—namely, relationship with mother and father, peer relationships, school climate, and neighborhood collective efficacy—has a unique association with his or her health.
Highly distinctive from their pediatric or adult counterparts, adolescents face challenges that are unique to this critical developmental stage. Drawing on Viner and colleagues’ (2012) proximal social determinants of health theory, we entered correlates from each domain in the same model to evaluate the association between domain-specific determinants and adolescents’ general health. All these correlates were either exclusively relevant to adolescents, for example, school environment, or had a much higher relevance to adolescent health than to the health of individuals in other developmental stages, for example, relationship with parents. As expected, we found compelling evidence that each individual domain of proximal determinants all resulted in a significant association with adolescents’ self-rated health. This is after controlling for known structural social determinants of health, like race and ethnicity, gender, and socioeconomic status, which further articulated the additional and unique impact on general health caused by proximal determinants that are part of adolescent daily life. Similarly, although research shows that self-rated health is affected by the existence of diseases or other health conditions, we found, as has been shown in previous studies, that the effects of social and environmental context on health prevailed (Bircher & Kuruvilla, 2014; Schulz & Northridge, 2004).
Our findings echoed what Viner and colleagues (2012) concluded: “. . . safe and supportive families, safe and supportive schools, together with positive and supportive peers are crucial in helping young people develop to their full potential and attain the best health in the transition to adulthood” (p. 1649). In addition, our findings also added to a wealth of literature on neighborhood environment as a powerful determinant of adolescent health. Studies of neighborhood environment have examined outcomes that are related to adolescent health, like educational attainment (Boyle et al., 2007), risky pregnancy (Harding, 2003), and adolescent mental health (Aneshensel & Sucoff, 1996). By linking neighborhood environment directly to adolescent general health outcomes, we further consolidate the health consequences of neighborhood environment on adolescents.
When entered into the model simultaneously, all proximal determinants demonstrated statistical significance, suggesting the unique significance of all determinants across domains. One of the key features that distinguish adolescence from other developmental stages is adolescents’ paramount need to socialize with their proximal environments, including family members, peers, school environment, and neighborhood (Miller-Slough & Dunsmore, 2016). This unique feature heightens the significant influence of these daily life circumstances on adolescent health. The results from this study highlighted the complex nature and various pathways proximal social determinants affect adolescent health.
A key factor in the social determinants of health is the presence of a social gradient. Although in our analysis we do not explicitly test for a gradient effect, we did find some evidence that the association between the adolescents’ environment and their health remains significant after controlling for social status. Even when accounting for all other variables, females tend to rate their health as significantly poorer than do males. In these data, however, the results did not show a gradient effect based on race and ethnicity; health outcomes among Hispanic and non-Hispanic Black adolescents did not differ significantly from those of non-Hispanic White adolescents. The results based on education and income were mixed. Adolescents whose households had a per-capita income of US$20,000 to US$39,000 had better self-rated health than did the lowest income group. When accounting for other demographic variables, parent’s education had no significant association with adolescents’ health. It is possible that the specific configuration of this sample, which was made up of adolescents born mostly to unmarried mothers, may explain these findings.
Our data suggest implications on two levels. First, even as the effects of proximal environments on health among adolescents can be cumulative, each domain acts independently, indicating that each domain uniquely contributes to the variation of adolescents’ general health status. This suggests that experiences in negative environments can be counterbalanced by more positive ones in others, thus informing our understanding of adolescent life chances more holistically. Second, all the key variables in our study were drawn from interviews with adolescents themselves, suggesting that the way they perceive their everyday encounters with family, peers, school, and neighborhood has a direct effect on their health. Research shows, however, that adolescents’ positive or negative perceptions of their environment are affected by their mental well-being and personality traits. For example, a recent study showed that experiences of anxiety, anger, and depressed moods associated with neuroticism lead teenagers to perceive family relationships as negative (Millikan et al., 2002). Thus, it is important to investigate personality factors that may moderate the relationship between social environments and health.
On a broader level, a critical implication of this study is what the results mean for understanding social determinants across the life span. Namely, the study raises the question of how adolescents navigate from environments of adolescence into environments of adulthood and how a trajectory of health outcomes is determined. In previous research (Zhang, Padilla, & Kim, 2017) in which we analyzed the same Fragile Families cohort from an earlier wave, at age 9, we showed that the effects of their social environments on health are evident at very young ages and operate in expected ways. In the current study, we analyzed social determinants at age 15. A study post high school can provide a view of yet another stage taking into account key turning points, such as educational attainment, incarceration, and childbearing. Although analyses have been extensively conducted at each phase, extensions of this research can involve breaking down the cumulative effects of social environments on health as individuals transition across the stages of the life cycle, from childhood to a adolescence to adulthood (Blane, 2006).
Limitations
A couple of limitations should be noted for this study. We used a cross-sectional design which prevents us from establishing causality. While the dataset is based on a longitudinal study, some of the key variables were not included in previous waves. As a result, we chose to conduct this current study using a cross-sectional design. Second, we were not able to include health behaviors, a key proximal social determinant, due to the unavailability of that variable. When available, future studies should include health behaviors in the model to evaluate how they interact with proximal environments to affect health. Third, the Fragile Families and Child Wellbeing Study contains only those who are 14- and 15-year-old adolescents. This only reflects a subgroup of adolescents. Future studies should include a wider age range, for example, 10 to 19 years old. Fourth, participants had a 25% attribution in Year 15 compared with baseline, which may contribute to attrition bias in this study. Finally, while we used a powerful and validated measure of general health, adolescent self-rated health, as a proxy measure of their general health, including biomarker outcomes in future studies can provide a deeper understanding of the effects on diseases, infections, or environmental exposures.
Conclusion
Despite the limitations mentioned above, to our knowledge, this study is among the few that evaluates multi-domain social determinants of health simultaneously in an adolescent population. It brings together strong lines of both research articulating the powerful effects of social determinants of health and research on the predictors of health in adolescence. We highlight the importance of attending to multiple determinants of health, especially those circumstances of adolescents’ everyday life. In so doing, we begin to unravel some of the mechanisms behind the life chances of adolescents from a more comprehensive perspective.
Footnotes
Authors’ Note
Kaipeng Wang is now affilIated with University of Denver, Denver, USA.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.