
Abstract
Youth, particularly urban minority youth, are exposed to high levels of stressful and potentially traumatic life events that have been linked to a wide array of negative outcomes including internalizing and externalizing problems. Youth perceptions of their interpersonal relationship quality with caregivers and friends were examined as potential promotive and protective factors counteracting the link between exposure to stressful and traumatic events and behavior problems. Participants were 85 urban, predominantly African American of age 13–17 years (60% girls). Results supported the hypothesis that youth report of parent trust and communication would serve as a promotive and protective factor, moderating the association between stressful life events and behavior problems. In contrast, peer trust and communication did not appear to counteract the association between stress and behavior problems. Instead, reports of trust and communication with friends appeared to increase the association between stress exposure and internalizing problems.
Stress Exposure is High Among Youth Living in Urban, Low-Income Minority Communities
Internationally, urban communities struggle to overcome adversities such as violence (Schultz et al., 2017), weapons (Luccisano & Macdonald, 2017), poor school systems (Bruce et al., 2019), increased cost of living, poor air and water quality as well as mounting poverty (Lim et al., 2012). Adolescents growing up in low-income urban environments have been found to be exposed to a greater number of adverse childhood events (ACEs) than those in other communities (Bethell et al., 2017; Vera et al., 2011). For instance, one national survey found that 69.3% of all children and adolescents surveyed had been victimized in the previous year, and 79.6% of the 12- to 17-year-olds had been victimized before 18 years of age (Finkelhor et al., 2009). In addition, urban youth and non-White, minority youth report being exposed to violence at higher rates than their more affluent Caucasian counterparts living in suburban or rural settings (Basch, 2011; López et al., 2017). Non-White youth are also exposed to racial discrimination at rates as high as 90%, meaning in addition to having more stressors, they also have distinct stressors from their Caucasian peers (Patcher et al., 2018). In other words, urban, African American youth are a unique sample within the United States with regards to exposure to community violence and other traumas and adversities.
As exposure to number of stressors such as violence increase, so too do symptoms of physical, mental, and behavioral health effects such as anxiety (Gorman-Smith & Tolan, 1998; Rosenthal, 2000), depression (Schwartz et al., 2005; Zinzow et al., 2009), aggression (Fowler et al., 2009; Margolin & Gordis, 2003), and academic impairment (Schwartz et al., 2005). In addition, López and colleagues (2017) found that having more than one type of traumatic event significantly predicted depression symptoms, lifetime delinquency, and substance use. In children as young as 4–6 years old, exposure to community violence is a predictor of higher numbers of health problems (Graham-Bermann & Seng, 2005). A meta-analysis examining the physical effects of exposure to community violence on children and teens found that asthma, immune functioning, hypothalamic–pituitary–adrenal axis functioning, weight, and general health are associated with exposure to violence with the strongest effects for sleep and cardiovascular health (Wright et al., 2017).
Trauma is highly heterogeneous in regard to type, frequency, developmental timing, and perpetrator(s) of the event(s). As such, there is a wide range of potential trauma reactions that vary in emotional and physical severity. For instance, trauma that is ongoing (e.g., years of abuse) versus acute (e.g., being a victim of a crime) will likely be different in terms of impact on the child exposed. There can be trauma involving family members as perpetrators (e.g., child neglect) or victims (e.g., intimate partner violence) as well as events that are “normal” and in some cases expected (e.g., death of a loved one from a chronic degenerative disease) and events that are unusual and unexpected (e.g., earthquake). Some researchers examine the effects of trauma by focusing on one type of trauma (e.g., the effects of child sexual abuse; or the September 11 terrorist attacks on New York). Others, including the current study, view trauma as having potentially cumulative effects on behavior outcomes. Chronic and cumulative trauma exposure has been conceptualized in several well-known theories, including complex trauma (Cook et al., 2017), ACEs (Wade et al., 2014) and polyvictimization (Turner et al., 2017). While these terms differ to a degree in definition and overlap to differing degrees in regard to operationalization, they also share a general common assumption that more stressors and traumas compound and contribute to negative outcomes. In other words, as exposure to traumatic events increases, negative outcomes increase proportionately regardless of the specific type of trauma (Hargreaves et al., 2019; Kerker et al., 2015). For the purpose of the current investigation, the term cumulative stress was used to reflect the number of lifetime stressful events or traumas the participants reported experiencing.
Promotive and Protective Factors, Especially Pertaining to Relationships With Family and Friends may Counterbalance the Effects of Stress
Variables thought to reflect positive processes and predict low probability of negative outcomes have been referred to as promotive factors, which are the antithesis of risk factors (Buckley & Chapman, 2018). Protective factors are those variables that go beyond correlating negatively with negative outcomes, instead, they are those variables that represent positive processes (e.g., social support) that statistically interact with risk factors and appear to buffer the effects of those risk factors (Loeber et al., 2008; Rutter, 1987).
Factors related to relationship quality with family members and friends have been found to reduce negative outcomes as well as the potential link between risk and problems. For example, Chen et al. (2016) found that reports of family warmth were associated negatively with deviant and delinquent behavior in the context of community violence exposure. In addition, Eisman and colleagues (2015) found that reports of violence observation and conflict in the family were associated with increasing depressive symptoms during the high school years, while perceptions of mothers’ support were associated with decreasing depressive symptoms across high school. Raja et al. (1992) found that teens’ perceptions of their attachment to parents were associated negatively with scores for conduct disorder and inattention as well as levels of negative life events and reported stress, and quality of family relationships also appeared to serve as a protective factor in the context of exposure to violence. Gorman-Smith and Tolan (1998) found that the family characteristics of structure and family cohesion appeared to buffer or reduce the association between exposure to community violence and aggression and anxiety/depression symptoms.
Although researchers have found that an adolescent’s relationship with their parents can be crucial in predicting the effects of trauma (Ozer et al., 2017), adolescence is also a time in development when peer relationships are gaining a new prominence in a youth’s life (Markiewicz et al., 2006). A meta-analysis showed small to medium effect sizes for an overall positive effect of having friendships on youth’s cognitive abilities and academic outcomes (Wentzel et al., 2018). The research on peer relationships as a promotive or protective factor is not consistent, however, as not all research regarding adolescent peers finds significant associations (e.g., Eisman et al., 2015). Raja and colleagues (1992) found that many of the youth who reported positive peer relationships also reported positive parental relationships, further muddying the waters of examining adolescent peer relationships as a promotive or a risk factor.
The Current Study Examines Relationship Quality as a Potential Promotive and Protective Factor
At any point in life, exposure to trauma and stressful life events can be detrimental to health; however, during adolescence, when many changes are taking place in terms of growth and development, exposure to stressful life events may have a particularly far-reaching impact (Casey et al., 2010; Graber & Brooks-Gunn, 1996; Vanes et al., 2019). This exposure can have negative effects, such as internalizing problems (Heleniak et al., 2018), externalizing problems (Fleckman et al., 2016), suicide attempts (Zatti et al., 2017), poor educational outcomes (Fry et al., 2018), and delinquent behavior (Chen et al., 2016). Although stress and trauma exposure are linked to these adverse effects, there are protective factors, including positive relationships that are associated with lower levels of negative outcomes (Ozer et al., 2017).
The present study aimed to assess trauma-exposure among urban adolescents, their perceptions of the quality of their parent and peer relationships as promotive and protective factors in the association between stressful life events and behavior problems. Hypotheses for the current study are as follows:
Method
Participants
The 85 participants of this study were urban youth aged 13−17 years (M = 15, SD = 1.42) and their primary caregivers recruited from an integrated behavioral health primary care clinic in a large, Midwestern city with a high rate of family poverty. The sample included 72 families; 13 families had a second child participating who were included in analyses making up the sample size of 85 children. Most of the youth (60.0%) were girls and the majority of the sample identified as African American (78.8%) and Christian (76.2%). Table 1 shows mean scores and standard deviations on other caregiver and family demographics. Given the health care setting provided therapeutic services, the sample was expected to have higher rates of utilization of mental health services than the general population. As anticipated, 44.7% of the sample reported using mental health services in the past, and 29.4% reported that they were currently receiving mental health services.
Correlation Matrix for Potential Covariates.
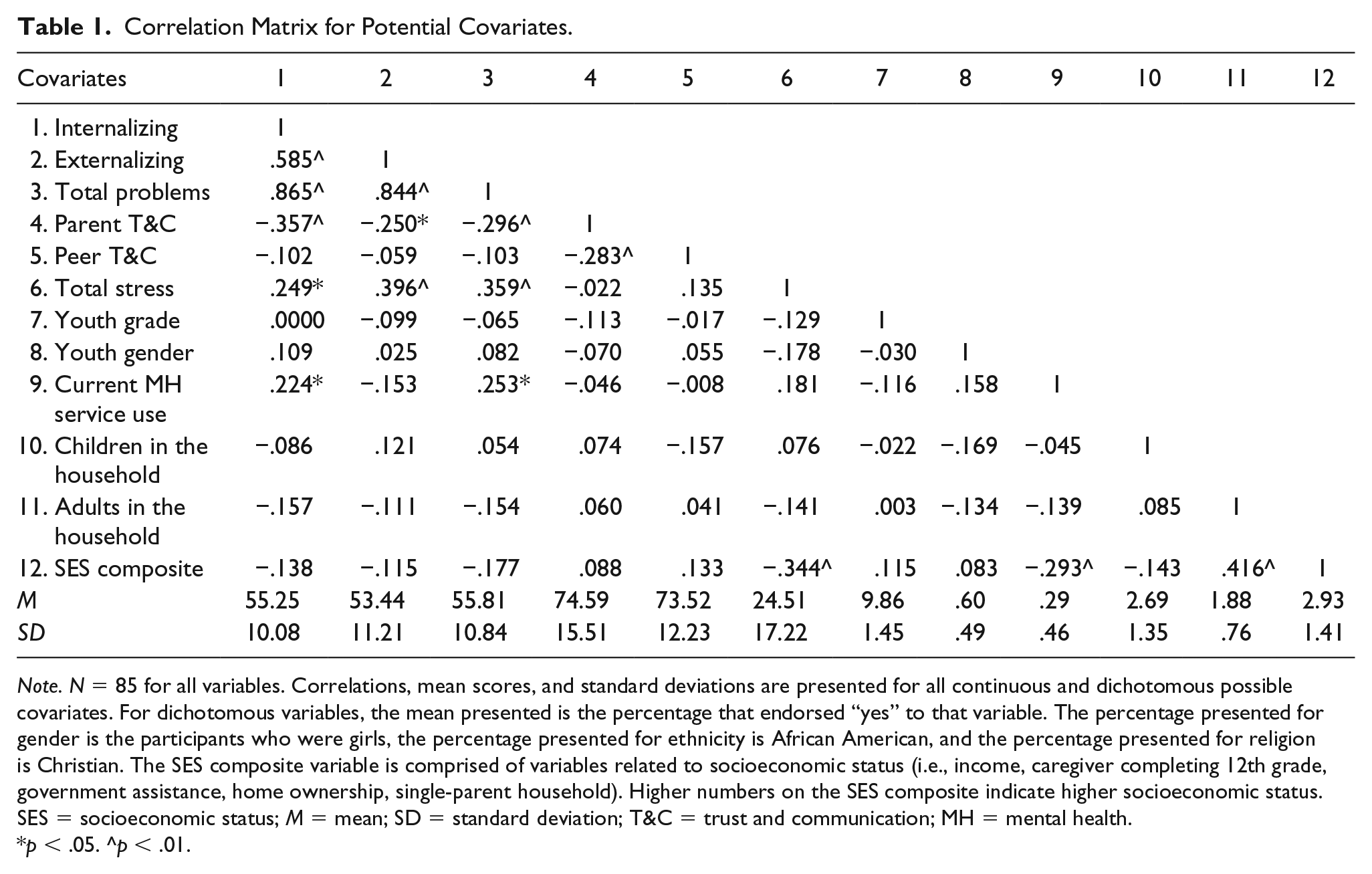
Note. N = 85 for all variables. Correlations, mean scores, and standard deviations are presented for all continuous and dichotomous possible covariates. For dichotomous variables, the mean presented is the percentage that endorsed “yes” to that variable. The percentage presented for gender is the participants who were girls, the percentage presented for ethnicity is African American, and the percentage presented for religion is Christian. The SES composite variable is comprised of variables related to socioeconomic status (i.e., income, caregiver completing 12th grade, government assistance, home ownership, single-parent household). Higher numbers on the SES composite indicate higher socioeconomic status. SES = socioeconomic status; M = mean; SD = standard deviation; T&C = trust and communication; MH = mental health.
p < .05. ^p < .01.
Procedure
All procedures were approved by the participating University and Hospital Institutional Review Boards. All participants were recruited for a study on adolescent health from the waiting room of a children’s hospital outpatient integrated care clinic in a large, Midwestern city. They learned about the study through flyers and medical staff at the clinic, who informed the child and caregiver that the study aimed, “to learn more about [urban] teenagers’ thoughts and opinions about their lives, including things like their strengths, what they find challenging, what their families are like, and what they think about therapy and counseling for teenagers.” In many cases, parents were approached in the waiting area by trained research staff to inform them about the study. The majority of interviews were scheduled to be completed at a later date at the researchers’ offices. After parental consent, youth and their primary caregivers participated in separate interviews lasting roughly an hour and a half. Youth assented prior to starting their individual interview when their parental figure was out of the room. Both the caregiver and adolescent each received US$20 cash at the completion of the interview.
Measures
Demographics
Youth and parents each completed an interview to collect general background information. Youth provided information about gender, school, ethnic background, religion, and prominent caregivers in their life. Information collected in the caregiver demographic interview included confirmation of primary caregiver role, relationship to the youth participating, number of children and adults in the home, and factors related to the family’s socioeconomic status.
Exposure to stressful life events
Exposure to stressful life events was measured using two youth-reported trauma measures: The Things I’ve Seen and Heard (TISH; Richters & Martinez, 1990) and the Stressful Life Events (SLE) questionnaires (Work et al., 1990). TISH is a 20-item survey from which three positively keyed items were removed because they asked about perceptions, such as feeling safe, rather than actual exposure to violence. The SLE has 22 items, however, the item “I have used drugs or alcohol” was dropped because it overlapped with an item on the Youth Self-Report described below. The items in both questionnaires detail events of exposure to family violence, community violence, and other stressors, such as a death in the family. On both measures, respondents indicated how many times in their life they have ever been exposed to the event on a 5-point scale (0 = never to 4 = four or more times). Example items from the TISH include: “Grown-ups in my home hit each other,” “I have seen a dead body outside,” and “Somebody threatened to shoot me.” Example items from the SLE include: “Parent has spent time in jail,” and “You have been in foster care.” The combined measure used in analyses consisted of a total score calculated from the number of times reported (0–4) from the items in both surveys. In the current sample, the measure showed good internal consistency, yielding a Cronbach’s alpha of .891 for total cumulative stress.
Behavior problems
Behavior problems were measured using the youth-reported Achenbach Youth Self Report (YSR; Achenbach, 1991). The YSR is a 112-item questionnaire covering a wide range of symptoms including both internalizing symptoms and externalizing symptoms. The YSR measure is coded on a 3-point Likert-type scale (0 = not true or rarely true to 2 = very true or often true). Based on responses to the YSR, the Achenbach’s System of Empirically Based Assessment (ASEBA) was used to obtain t scores for internalizing, externalizing, and total problems by comparing the participants to normative findings for youth their age and gender. The internalizing problems domain included problems related to depression, anxiety, and somatization. The externalizing problems domain included problems related to acting out, delinquency, and aggression. The total behavior problems domain provided a global representation of all internalizing and externalizing problems as well as social problems, attention problems, and thought problems. Examples from the internalizing symptoms scale include: “I worry a lot,” and “I feel that no one loves me.” Examples from the externalizing symptoms scale include: “I get in many fights,” and “I disobey at school.” Higher t scores indicated higher levels of symptoms, with t scores over 64 indicating clinical levels of symptoms. Since the t scores were generated using ASEBA rather than individual item responses, an alpha for this sample was not calculated. However, previous research on the reliability of the total problems composite has found a high internal consistency with a Cronbach’s alpha of .95 (Steinhausen & Metzke, 1998).
Relationship quality (trust and communication) with primary caregiver and peers
Adolescents’ relationship quality with parents and friends was measured by the youth-reported trust and communication subscales of the Inventory of Parent and Peer Attachment (IPPA: Armsden & Greenberg, 1987). Youth completed a version of the subscales for parent relationships and a version of the subscales for peers. There are 19 items on the measure assessing trust and communication with the primary caregiver, and there are 18 items on the measure assessing trust and communication with peers. Both the parent and peer questionnaires coded on a 5-point Likert-type scale (1 = almost never or never true to 5 = almost always or always true). Sample items from the parent composite include: “My caregiver respects my feelings,” and “I like to get my caregiver’s point of view on things I’m concerned about.” Sample items from the peer composite include: “My friends understand me,” and “My friends can tell when I’m upset about something.” Higher scores reflect higher levels of trust and communication in the relationship. In this sample, the IPPA showed good internal consistency, yielding a Cronbach’s alpha of .947 for the parent measure and .945 for the peer measure.
Results
First, data were analyzed for univariate outliers and normality. The peer relationship quality, total stress, and externalizing problems variables each had one univariate outlier based on z scores that exceeded 3.29 (p <.001; Tabachnick & Fidell, 2013). All three univariate outliers were Winsorized, meaning the values were replaced with the next closest value. Two variables with significant skew, parent relationship quality and total stress, were transformed to achieve a normal distribution. The parent relationship quality variable had significant negative skew, which was corrected using a centered square-root transformation (Howell, 2007; Tabachnick & Fidell, 2013). The total stress variable had significant positive skew, which was corrected using a square root transformation (Howell, 2007; Tabachnick & Fidell, 2013). One multivariate outlier was identified using Mahalanobis distance, χ2 (8) = 26.95, p < .001; Tabachnick & Fidell, 2013. Analyses were performed with and without the participant that contained this outlier (Tabachnick & Fidell, 2013), and there was no change to significance or direction of the findings. Final analyses reported in Table 2 includes this outlier as well as the Winsorized univariate outliers and the transformed variables.
Traumatic Events Predicting Youth-Reported Behavior Problems.
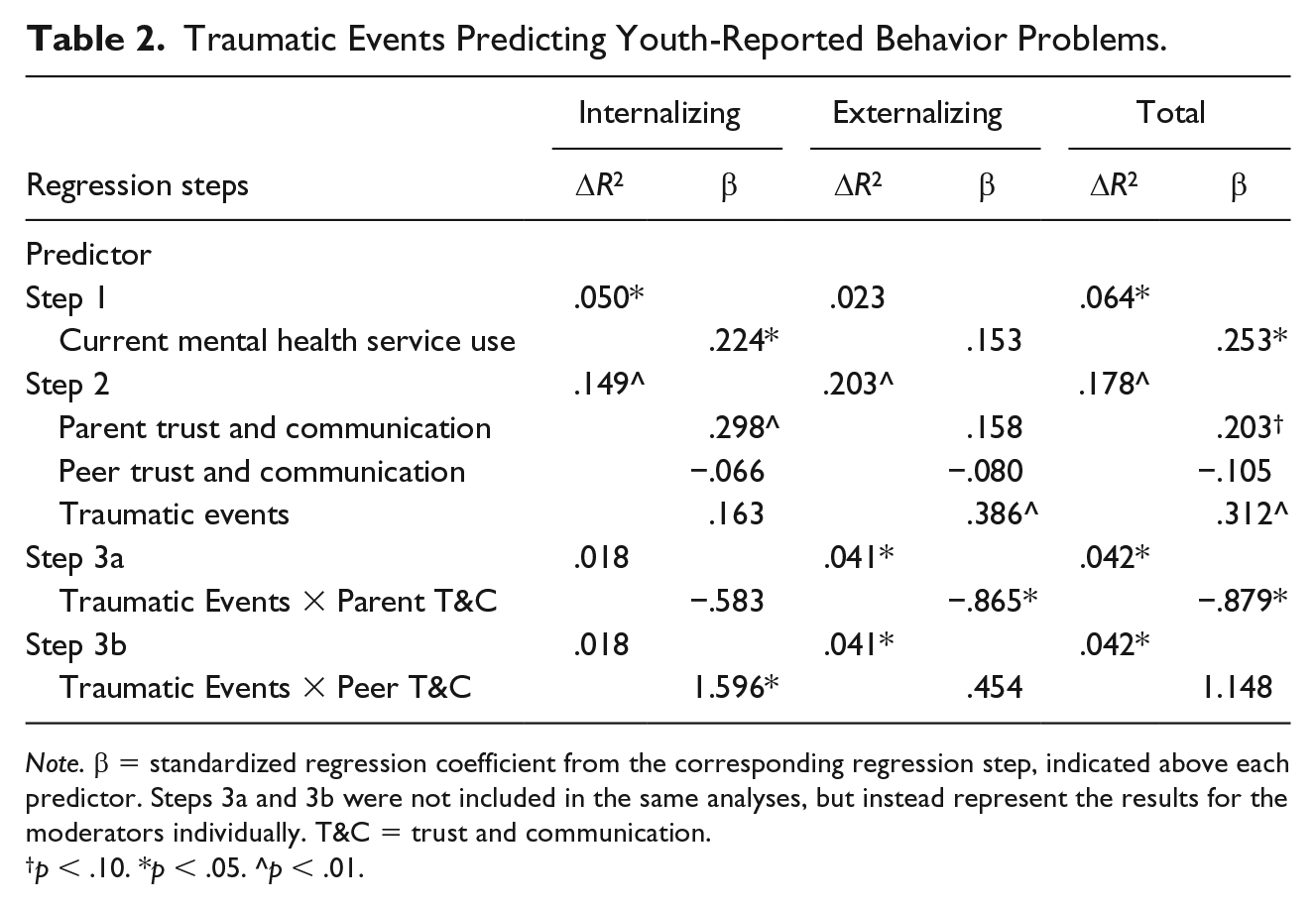
Note. β = standardized regression coefficient from the corresponding regression step, indicated above each predictor. Steps 3a and 3b were not included in the same analyses, but instead represent the results for the moderators individually. T&C = trust and communication.
p < .10. *p < .05. ^p < .01.
Second, several demographic variables were examined as possible covariates of the three outcome variables of total behavior problems, internalizing problems, and externalizing problems. Specifically, youth grade, youth gender, ethnicity (dichotomized as African American or other), religion (dichotomized as Christian or other), current mental health service use, number of children in the household, number of adults in the household, family income, caregiver highest grade completed, number of parents in the household, utilization of government assistance, and home ownership were assessed as potential confounding factors using correlation analyses (see Table 1). Ethnicity and religion were dichotomized due to the disproportionate number of participants who identified as African American and Christian. Analyses were also run on the nondichotomized version of these variables, and there were no significant group differences in any of the three outcomes. Socioeconomic variables were examined as a composite to look at cumulative differences between families. Of the variables examined, only current mental health service use was found to be correlated significantly with reporting more total behavior problems (r = .253, p < .05) and internalizing problems (r = .224, p < .05), and therefore, it was included as a covariate in all multivariate analyses.
In the current sample, the presence of 13 sibling participants reporting on the same primary caregiver violates the statistical assumption of independent observations. Consequently, the analyses were rerun excluding younger siblings, using only the 72 unique families. The removal of the siblings did not change the direction or significance of the findings, consequently, this manuscript and tables report analyses for the entire sample.
Total stressful events to which youth were exposed (M = 24.51, SD = 17.22, see Table 1) was utilized in analyses. This total number includes multiple instances of the same event, so an additional metric was calculated to represent the number of different, unique kinds of events to which youth were exposed, and participants averaged nearly 11 different stressful events (M = 10.85, SD = 6.69); Table 3 reports on the percentage reporting each type of event. Regarding total behavior problems, t scores on the YSR ranged from 29 to 80. Scores of 64 (92nd percentile) or higher are considered clinically significant (Achenbach, 1991), and 27.9% of the sample fell above that cutoff on total behavior problems. For internalizing problems, scores ranged from 32 to 87 with 21.4% falling above the clinical cutoff. In terms of externalizing problems, scores ranged from 29 to 87, and 15.5% fell above the clinical cutoff.
Endorsed Stressful Life Events.
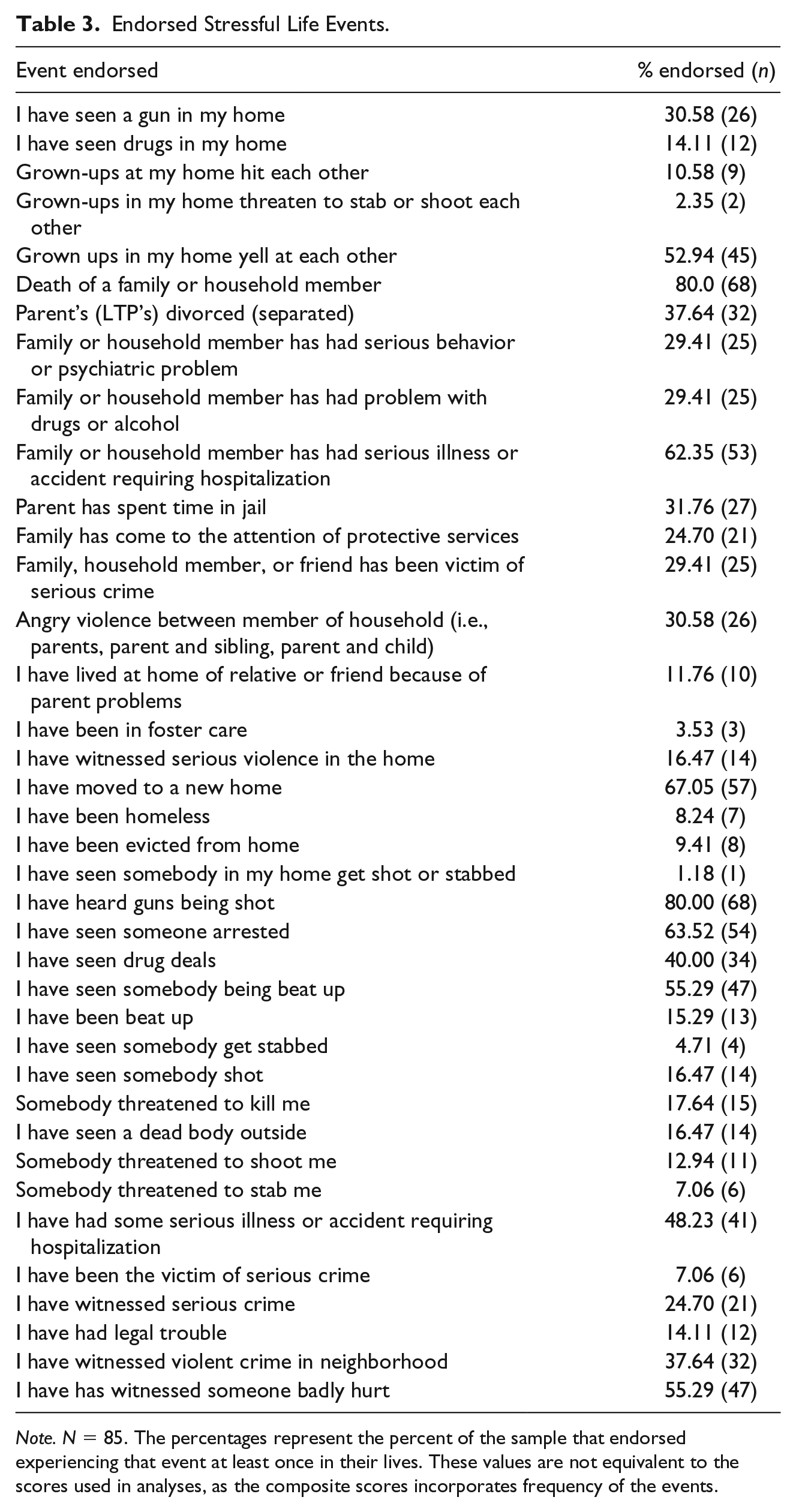
Note. N = 85. The percentages represent the percent of the sample that endorsed experiencing that event at least once in their lives. These values are not equivalent to the scores used in analyses, as the composite scores incorporates frequency of the events.
Direct Effects
In the first step of the model, current mental health care service use was entered as the covariate. It was significant in predicting total behavior problems, ΔF(1, 83) = 5.70 p = .019; ΔR2 = .064; t(83) = 2.386, p = .019, and internalizing problems, ΔF(1, 83) = 4.373, p = .040; ΔR2 = .039; t(83) = 2.091, p = .040. Behavior problems increased as a function of current mental health service use. All regression results can be found in Table 2.
In the second step of the model, total stressful life events, parent trust and communication, and peer trust and communication were added to current mental health care service use. This model predicted behavior problems above and beyond mental health care service use for total behavior problems, ΔF(3, 80) = 6.270, p = .001; ΔR2 = .178, internalizing problems, ΔF(3, 80) = 7.004, p < .001; ΔR2 = .203, and externalizing problems, ΔF(3, 80) = 4.949, p = .003; ΔR2 = .149.
Within these models, several direct effects were found to be significant. Results showed that both total behavior problems and externalizing problems increased as a function of stressful life events, t(80) = 2.974, p = .004 and t(80) = 3.639, p <.001, respectively. Results also showed that internalizing problems decreased as a function of parent trust and communication, t(80) = 2.791, p = .007, while there was a near significant trend toward decreased total behavior problems as a function of parent trust and communication, t(80) = 1.953, p = .054.
Moderation Analyses
The final steps of the models examined relationship quality as moderators. The first set of analyses examined the interaction between parent trust and communication and total stressful life events as a predictor, and results showed this third model was able to predict total behavior problems, ΔF (1, 79) = 4.629, p = .034; ΔR2 = .042, and externalizing problems, ΔF (1, 79) = 4.383, p = .039; ΔR2 = .041, above and beyond the prior model, which included parent trust and communication, total stressful life events, and current mental health service use. The interactions for externalizing and total behavior problems were graphed and indicated that parent trust and communication buffered the association between exposure to stressful life events and externalizing and total behavior problems. The total behavior problems graph is presented on the left side of Figure 1.
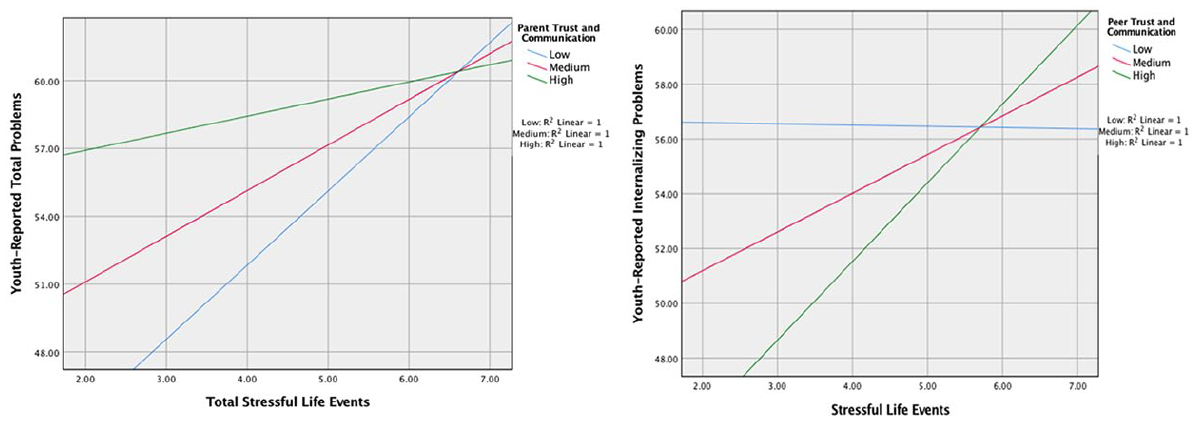
Parent trust and communication (left) as moderator in the relationship between exposure to stressful events and total behavior problems, and peer trust and communication (right) as a moderator in the relationship between exposure to stressful events and internalizing problems. Both graphs use data points from Hayes (2017) PROCESS Macro.
A second set of moderation analyses examined the interaction between peer trust and communication and stressful life events in predicting behavior problems. Results showed this model was able to predict internalizing behavior problems, ΔF (1, 79) = 5.047, p = .027; ΔR2 = .048, above and beyond the model including current mental health service use, parent trust and communication, peer trust and communication, and total stressful life events. The interaction was graphed in Figure 1 (right side), indicating that peer trust and communication appears to moderate the relationship between exposure to stressful community events and internalizing problems; however not in the expected buffering fashion. Rather, youth with higher levels of peer trust and communication showed a stronger positive relation between cumulative stress and behavioral problems than youth who reported lower levels of peer trust and communication.
Discussion
The Challenge for Youth From Low-Income, Urban Communities
For too many, especially low-income families, living in an urban environment brings numerous health risks. Recruiting from an urban primary care clinic at a children’s hospital resulted in a sample of adolescents who had been exposed to substantial economic, neighborhood, and family stressors; and who reported higher levels of clinically significant behavior problems than in “normative” samples. The primary care setting offered integrated behavioral health services, which likely explains why more than 44% of the sample had received or were receiving mental health services. On the contrary, because the children who were and were not in treatment had similar levels of stressful life events, the recruitment location did not appear to explain the high numbers of stressful event exposure. Those currently receiving mental health services reported higher internalizing and total problems, which presumably was part of the reason they were obtaining help (Tsang et al., 2020). It is important to consider that the goals of mental health treatment include diminishing behavior problems, and therefore this could potentially reduce the connection between stress exposure and behavior problems among those in treatment in this sample. To statistically account for this possibility, current mental health treatment was used as a covariate in analyses.
Using a list of events that have been identified as objectively stressful—in contrast to a measure of perceived stress—was a methodological strength of this study, increasing its rigor. Objective events without attention to the perceived effect of those events creates a construct that is conceptually and operationally distinct from perceived stress and stress symptoms (e.g., anxiety, insecurity). For example, questionnaires that assess perceived stressful impact of events can confound the measure of exposure with the measure of symptoms (Monroe, 2008). Therefore, using the objective stress measure is a strength. However, self-report objective stress measures come with challenges of their own, as discussed in the limitations. Furthermore, the current study was successful in demonstrating the association between these events and behavior problems independent from socioeconomic risk factors such as family income and parental education. In other words, living in a low-income urban area appeared to result in substantial exposure to stressful events and thereby contributed to youth behavior problems, rather than living in the low-income community directly causing the behavioral effects. This supports the hypothesis that exposure to stressful events accounts for a significant portion of the health effects of poverty, in contrast to poverty, per se.
Having a Parent Whom You can Trust In and Communicate With Appears to Matter Especially When There Are Many Stressors
The findings regarding youth perceived trust and communication in their relationship with their primary caregiver appearing to serve both a promotive and protective process is generally commensurate with the literature (e.g., Eisman et al., 2015; Gorman-Smith & Tolan, 1998 ; Raja et al., 1992). Results of the current investigation serve as a contemporaneous (data gathered in 2017–2018) replication, as parent trust and communication predicted behavior problems as well as partially buffered teens from the effects of exposure to stressful life events. These results highlight the continued positive effect of supportive family relationships into adolescence and underscore the positive health impact of caregivers maintaining close, open, and supportive relationships with adolescent children (Maiuolo et al., 2019; Wills et al., 2019).
How or why youth who report greater trust and communication with their parent also report fewer behavior problems is not clear from these data. One possible explanation can be found within the literature regarding adolescent attachment, mainly the element that posits that parents act as a secure base from which the teen can explore the world around them (Allen & Tan, 2016). If teens have trust and communication forming a secure base, they may feel more comfortable interacting with the world, leading to better behavioral adjustment and fewer behavioral problems (Richardson et al., 2019). Intervention research has supported the idea that improving communication between adolescents and their parents is a significant component of reducing adolescent internalizing symptoms and suicide risk, especially for African Americans (Zisk et al., 2019).
Based on these findings, it appears that when the environment contains greater dangers as appears to be the case in the inner city neighborhoods of the current participants, close relationships with regard to trust and communication with caregivers appear to be especially protective or buffering from stress. Referencing attachment theory and research, Van der Kolk (1987) wrote, “Trauma occurs when one loses the sense of having a safe place to retreat within or outside oneself to deal with frightening emotions or experiences” (p. 31). In other words, youth who maintain trust and communication with their primary caregiver may maintain their psychological sense of security, trust, and safety when faced with significant stressful events that are associated greatly with internalizing and total problems when youth report having less stress and communication with their caregiver (Gobin & Freyd, 2014; Goodman et al., 1991). Interestingly, there was not a significant association between youth report of trust and communication with their caregiver and the number of stressors youth reported experiencing. Apparently, in these urban neighborhoods, trust and communication does not appear to prevent youth from being exposed to them physically, however, this relationship appears to buffer them psychologically.
Having Friends Whom You can Trust and Communicate With did not Appear to Shield Youth From the Effects of Stress
Findings regarding whether friendships during adolescence serve as protective or as risk factors have been variable in the literature (Sentse et al., 2010). Often, these studies have been conducted using low-risk samples, and findings are dependent on aspects of the friends about whom the participant is responding. For example, elements not encompassed in the measure of relationships quality, such as relational aggression, popularity, and prosocial and antisocial behaviors, have differential impacts on outcomes such as mental health symptoms, academic success, and substance use (e.g., Deković, 1999; La Greca & Harrison, 2005). Similarly, it is possible that the impact of high quality friendships on behavior problems varies based on the characteristics of the individuals involved in the friendship. For example, teens reporting high quality relationships with friends who engage in antisocial behavior, rumination, or problematic coping skills may experience higher levels of behavior problems. Conversely, teens reporting high quality relationships with friends who engage in prosocial behavior, activities, or positive coping skills may experience lower levels of behavior problems. Unfortunately, the current study’s measure of peer trust and communication did not tap into these characteristics and does not allow for further exploration in this area.
In most studies, positive parental relationships are typically associated positively with peer relationships. Surprisingly, caregiver and peer trust and communication were significantly, negatively associated with one another in the current study. This suggests that for African American youth in our sample, high quality relationships with one’s caregivers was associated with lower quality relationships with one’s peers. There are several possible explanations for this finding. Caregivers raising youth in disadvantaged neighborhoods may have more restrictive rules regarding peer relationships due to concerns about safety. Furthermore, these youth may have more home-based responsibilities in terms of caring for younger siblings and housekeeping tasks due to caregiver workloads or schedules. Finally, there is evidence that African American caregivers may convey different messages about peer relationships than White caregivers. A study by Way et al. (2007) found that non-White youth report that their caregivers express wariness about trusting peers and concerns that peers may serve as negative influences. Thus, these caregivers discourage peer relationships and do not place a high value on developing these relationships. Taken together, these issues might explain why caregiver and peer trust and communication were not positively associated in this predominately African American, low-income sample.
Implications, Limitations, and Future Directions
The current study suffers numerous shortcomings including being cross sectional, relying heavily on self-reports from a single informant, and relatively small sample size. Because the study is correlational, caution is encouraged regarding the implicit assumptions about causation and the direction of the effects. However, experimental, intervention, and longitudinal studies in the literature generally support the assumptions that stress contributes to adverse health effects and that relationships with caregivers may counteract those probable effects (Collins et al., 2000). The large amount of accumulated data also highlights the bidirectional or reciprocal influences among stress, genes, and experience within families (Sapolsky, 2017). It is safe to say that numerous unidentified and unmeasured biopsychosocial factors are missing from the implied models analyzed herein.
Another limitation was the study’s heavy reliance on self-report measures from a single informant. Consequently, the responses were contingent on the youth’s perspectives, level of insight into each of those areas of their lives, and willingness to report that information truthfully. Specifically related to the stress measure, objective self-report measures of stress can be psychometrically unreliable, though the current study found good internal consistency (Monroe, 2008). Although the construct of parent and peer trust and communication is described as youth perception of those aspects of their relationships, research (e.g., Harmon-Walker & Kaiser, 2015 ; Ridenour et al., 2006) has linked the IPPA to other types of attachment measures, including more cognitively based self-reports of attachment and projective measures of attachment. Future studies are encouraged to incorporate other measures of the constructs examined herein, that don’t rely solely on self-report.
We also hope researchers will examine whether humans have a greater vulnerability to stressful events during adolescence than other developmental periods. In these types of future investigations, the current results may be useful in developing interventions to ameliorate some of the deleterious effects of stressful life events. For example, interventions for teens involving parents have been found to produce improvements over treatment as usual options (Sibley et al., 2013). In addition, based on these results, clinicians may incorporate parents and relationship quality into their treatment of adolescents.
Finally, in researching the characteristics of developing in an urban setting, future studies would benefit from continuing to incorporate promotive and protective factors, such as family strengths and resilience. Although there are high levels of documented stress in youth living in disadvantaged neighborhoods, urban areas do offer opportunities, such as venues for culture, learning, and services, that are not available in rural areas. These, along with individual strengths of youth and families, may promote positive outcomes in the face of stress and trauma.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.