
Abstract
Healthcare worker burnout is a complex phenomenon that traditional linear models fail to fully explain. This study uses network analysis to map the associative interactions between organizational factors, mental health symptoms, and burnout dimensions in a national sample of Peruvian physicians and nurses. Cross-sectional network analysis using data from the 2016 National Healthcare Worker Survey, comprising 4951 healthcare professionals (2125 physicians, 2826 nurses). Twenty-two variables spanning burnout dimensions (MBI-GS), mental health symptoms, work satisfaction, and organizational factors were analyzed using Gaussian Graphical Models with bootstrap validation (1000 iterations). Expected Influence, Betweenness, Closeness, and Strength centrality indices were calculated. Network invariance testing compared structural differences between professions. The network comprised 22 nodes with 82 non-zero edges (density = 0.355). Health services management satisfaction showed the highest expected influence (EI = 2.14), followed by monthly income (EI = 1.49). Emotional exhaustion showed substantial negative influence (EI = −0.46). Network invariance testing revealed statistically significant structural differences between professions (M = 0.2289, P = .0099), though overall similarity was moderate to high (ρ = 0.685). Nurses showed higher expected influence for job stability (EI = 0.619 vs 0.375), while physicians showed higher expected influence for marital status (EI = 0.659 vs 0.416). Bootstrap stability coefficients exceeded recommended thresholds (CS = 0.67-0.75). Burnout components showed network patterns consistent with complex adaptive systems, with organizational factors (management satisfaction, income) displaying higher expected influence than individual mental health symptoms. Network structures differed statistically between professions, though with moderate-to-high overall similarity. We propose a preliminary exploratory framework (SPIRAL model) identifying 6 network-based patterns that require prospective longitudinal validation before clinical application.
Healthcare worker burnout is widely studied, yet dominant frameworks (JD-R, Maslach’s sequential model, COR theory) rely on linear or latent variable approaches that may not capture the simultaneous, interconnected associations among organizational, psychological, and social factors involved in burnout.
Network analysis of 4,951 Peruvian healthcare workers reveals that organizational factors (management satisfaction, income) show the highest expected influence in the burnout network, while individual mental health symptoms occupy peripheral positions. Network structures differ significantly between nurses and physicians, with profession-specific centrality patterns.
These findings support conceptualizing burnout as a complex adaptive system and suggest that interventions targeting high-centrality organizational nodes may yield greater impact than individually focused approaches. The exploratory SPIRAL framework identifies six network-based patterns for hypothesis generation regarding profession-specific, systems-level interventions.
Introduction
Healthcare worker (HCW) burnout has emerged as a significant threat to global health, with prevalence rates reaching unprecedented levels, compromising both provider well-being and the quality of patient care.1,2 This crisis affects multiple levels: individual providers experience increased mental health symptoms and reduced job satisfaction, while organizations face higher leave rates, absenteeism, and compromised patient safety.3-5
Despite widespread recognition, existing theoretical frameworks offer divergent and sometimes contradictory explanations for burnout development. 6 The Job Demands-Resources (JD-R) model frames burnout as a consequence of imbalanced demands and resources, yet it does not fully account for why individuals exposed to similar demand-resource profiles develop different burnout trajectories.7,8 Maslach’s 3-component framework proposes a sequential progression from emotional exhaustion through cynicism to reduced professional efficacy; however, empirical evidence suggests this linear sequence is not universal across professional contexts. 9 The Conservation of Resources (COR) theory emphasizes resource loss spirals but treats contributing factors in relative isolation, while the Areas of Worklife model identifies 6 organizational domains without providing further explanation of their mutual interactions.6,8 These inconsistencies suggest that traditional approaches, which typically model burnout through latent variables or linear approaches, may inadequately represent the simultaneous, interconnected associations among the multiple factors involved in burnout. 10
Network analysis offers a complementary methodological approach that addresses some of these limitations. 11 Unlike latent variable models, which assume that a single underlying construct causes observed symptoms, network analysis examines the direct pairwise associations among individual variables, allowing researchers to identify which factors occupy central versus peripheral positions within the associative structure.10,12 This approach has been increasingly applied in mental health research to generate hypotheses about which variables may play structurally important roles within symptom networks.13,14 However, it is important to note that cross-sectional network analysis is inherently descriptive and cannot establish causal or temporal relationships among variables. 15 With this in mind, we applied network analysis as a hypothesis-generating tool to map the associative structure among mental health indicators, work-related factors, social support, work satisfaction, and burnout dimensions in a nationally representative sample of 4951 Peruvian healthcare workers, comparing network configurations between nurses and physicians.
Methods
Study Design and Sources
We conducted a cross-sectional analytical study following the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines 16 and psychological network reporting standards 15 using secondary data from the 2016 National Healthcare Satisfaction Survey (ENSUSALUD). ENSUSALUD employed stratified 2-stage cluster sampling with 183 health facilities across all Peruvian departments, ensuring national representativeness of Peru’s fragmented healthcare system. 17 Although data collection preceded the COVID-19 pandemic, this pre-pandemic dataset provides a baseline for examining burnout network structures under routine working conditions, independent of pandemic-related confounders that substantially altered healthcare workforce dynamics globally.
The survey was conducted between April and July 2016 by the National Institute of Statistics and Informatics under the coordination of the National Health Superintendence and the Ministry of Health, using standardized questionnaires administered to healthcare professionals. The anonymized dataset was accessed through the official SUSALUD portal (https://portal.susalud.gob.pe/blog/base-de-datos-2016/) on May 3, 2024, downloaded, and imported into RStudio for analysis.
Participants
Healthcare professionals (physicians and nurses) employed in Peru’s Ministry of Health facilities were eligible for inclusion. Inclusion criteria were: (1) active clinical practice at the time of survey administration, (2) completion of ≥80% of survey items, and (3) provision of informed consent. Exclusion criteria were: (1) administrative-only positions without direct patient care, (2) incomplete burnout dimension measures (missing ≥ 2 of 3 MBI-GS subscales), and (3) duplicate submissions identified by timestamp and IP address matching. The final analytical sample comprised 4951 participants (2125 physicians and 2826 nurses) after applying these criteria.
The sample comprised 4951 healthcare workers (2125 physicians, 2826 nurses) aged 23 to 76 years (M = 45.08, SD = 11.27). Most were female (62.88%), had work stability (69.84%), and worked outside Lima (77.60%). One-third were married (33.61%), with the majority earning 3001 to 7500 new soles monthly (57.24%), equivalent to approximately 1000 to 2000 USD. Power analysis indicated an adequate sample size (recommended n = 3000 for a network density of 0.40 with 22 nodes)
Variables
Twenty-two variables were organized into 6 conceptual domains (Life and Support, Burnout, Mental Health, Work Satisfaction, Work Conditions, and Exposures) for descriptive purposes only to facilitate the presentation and interpretation fo results. This was informed by burnout and occupational health literature,6,8,9 and the thematic structure of the assessed constructs.
Sleep-related measures were classified under Mental Health because they were assessed through symptom-based instruments. 18 Work Conditions and Exposures were distinguished based on their temporal nature: Work Conditions encompasses chronic structural employment characteristics, whereas Exposures refers to discrete adverse events (workplace violence incidents) experienced within a defined recall period, consistent with occupational health frameworks distinguishing chronic conditions from acute incidents.6,9 All scales and subscales entered the network as summary scores (1 node per scale), not as individual items. Included variables were as follows:
Life and Support: Marital status (binary: single vs partnered) and family living arrangement (binary: alone vs with family support).
Burnout: Three Maslach Burnout Inventory subscales on 7-point frequency scales - emotional exhaustion (9 items), cynicism/depersonalization (5 items), and self-efficacy (8 items). 19
Mental Health: Sleep hours (continuous daily average), sleep problems (4-item Jenkins Scale, 6-point frequency scale, range 4-24), work-life balance (single 5-point Likert item), and depressive symptoms (PHQ-2, two items scored 1-4, total range 2-8). 18
Work Satisfaction: Four 5-point satisfaction scales from ENSUSALUD survey—work safety (6 items, range 6-30), general profession satisfaction (6 items, range 6-30), health services management satisfaction (8 items, range 8-40), and working conditions satisfaction (16 items, range 16-80). 20
Work Conditions: Years of practice (continuous, time since graduation), weekly hours (continuous total worked), job stability (binary: stable vs non-stable contract), monthly income (ordinal, 6 brackets from S/. 750-1500 to >S/. 10 000), and care level (categorical: primary/secondary/tertiary complexity). 17
Exposures: Four binary workplace violence variables over the previous 12 months (threats/intimidation, insults/verbal abuse, sexual harassment, physical aggression), coded as No = 0, Yes = 1.
All multi-item instruments used in this study have been previously validated. The MBI-HSS has been validated in Peruvian healthcare population. 19 The PHQ-2 has demonstrated adequate psychometric properties in clinical population in Peru. 21 The Jenkins Sleep Scale has been validated in Spanish-speaking samples. 18 The 4 satisfaction scales were developed and validated specifically for Peruvian healthcare workers within the ENSUSALUD framework. 20 The complete survey instruments are provided as Supplemental File 1.
Data Analysis
Prior to network estimation, we examined the measurement properties of the 22 study variables. The dataset comprised continuous variables (sleep hours, years of practice, weekly hours worked), ordinal scales (3 burnout subscales, 4 satisfaction subscales, sleep problems, depressive symptoms, work-life balance, monthly income), and binary indicators (marital status, family living arrangement, job stability, and 4 workplace violence exposure items). Care level was treated as ordinal, reflecting ascending facility complexity from primary through tertiary care. 22 All variables entered the analysis in their original metric without transformations.
Network analyses were conducted in R (version 4.1.2) following established network psychometrics guidelines. 12 We estimated the network structure using the bootnet package (version 1.5) with Gaussian Graphical Model selection (ggmModSelect), which employs regularization to identify non-zero associations while controlling for all other variables in the network. Given the mixed measurement levels in our dataset, we computed pairwise associations using Spearman rank-order correlations, which accommodate ordinal and non-normal continuous variables by evaluating monotonic relationships based on rank ordering rather than assuming linearity or interval-level measurement.12,15
To characterize each variable’s structural importance within the network, we calculated 4 centrality indices: Expected Influence (EI), Betweenness, Closeness, and Strength. We prioritized EI for interpretation because it accounts for both positive and negative edge weights, making it more appropriate than Strength for networks with mixed-sign associations. 23 Betweenness quantifies how often a node lies on the shortest path between other nodes, Closeness captures average distance to all other nodes, and Strength represents the sum of absolute edge weights connected to a node. 24
We assessed network stability and accuracy through non-parametric bootstrap procedures with 1000 iterations. Stability of centrality indices was evaluated using case-dropping bootstrap, yielding Correlation Stability (CS) coefficients; CS values above .50 indicate that centrality order remains stable after dropping subsets of the data. Accuracy of edge weights was evaluated by generating 95% confidence intervals around each pairwise association. To compare network structures between nurses and physicians, we used the NetworkComparisonTest package with permutation-based hypothesis testing (1000 replications, α = .05), testing for network invariance (M statistic, assessing overall structural differences) and global strength invariance (S statistic, assessing total connectivity).
Results
Global Network Properties and Central Indices
Figure 1 shows the estimated network comprising 22 nodes with 82 non-zero edges from 231 possible connections (density = 0.355). The strongest relationships included working conditions satisfaction and health services management satisfaction (r = .58), as well as emotional exhaustion and cynicism (r = .39), and weekly hours and monthly income (r = .43). The strongest negative relationship occurred between emotional exhaustion and self-efficacy (r = −.22).
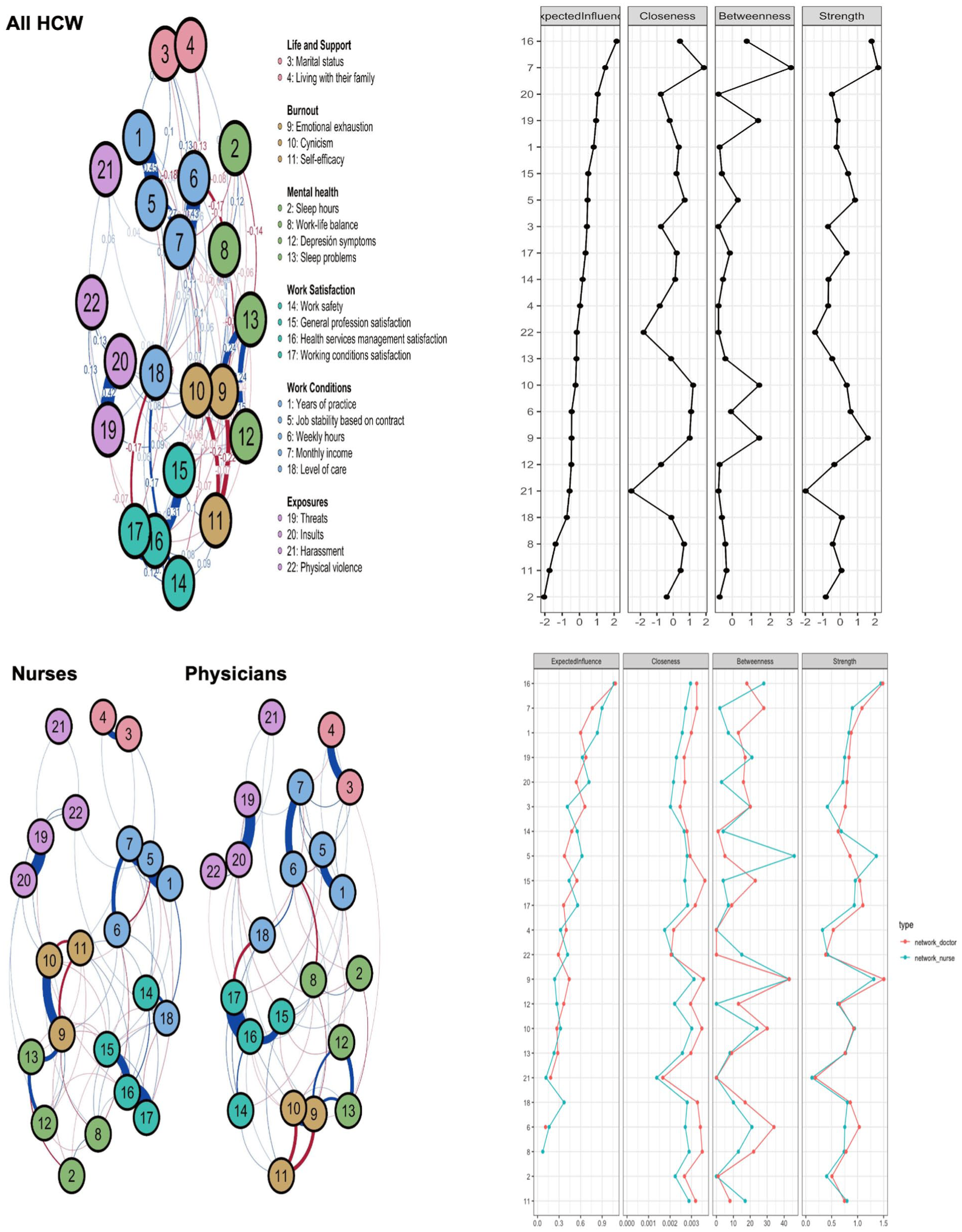
Network estimation and centrality indices for all samples and subgroups (physicians and nurses).
Health services management satisfaction showed the highest expected influence (EI = 2.14), followed by monthly income (EI = 1.49). In contrast, emotional exhaustion showed a substantial negative influence (EI = −0.46). Monthly income showed the highest centrality across multiple measures (betweenness = 3.07, closeness = 1.86, strength = 2.18). Lastly, bootstrap analysis with 1000 iterations yielded robust stability coefficients (0.67-0.75) exceeding recommended thresholds.
Professional Network Differences
Network invariance testing revealed statistically significant structural differences between professions (M = 0.2289, P = .0099); however, overall network similarity was moderate to high (ρ = 0.685). Within this context of general similarity, we observed specific differences in centrality indices and edge weights. Nurses showed higher expected influence for job stability (EI = 0.619 vs 0.375 in physicians, Δ = +0.244) and a stronger job stability-monthly income association (r = .390 vs r = .161, Δ = +0.229). Physicians showed higher expected influence for marital status (EI = 0.659 vs 0.416 in nurses, Δ = +0.243).
Discussion
Summary of Findings
Here, we conducted a cross-sectional network analysis involving 4951 Peruvian healthcare workers (2125 physicians and 2826 nurses) to examine the associations between mental health symptoms, work-related factors, social support, work satisfaction, and burnout components. Our major findings are as follows: (1) Burnout components showed strong associations within the network, with emotional exhaustion showing strong connections to cynicism (r = .39) and negative associations with self-efficacy (r = −.22); (2) Health services management satisfaction (EI = 2.14) and monthly income (EI = 2.18) showed the highest expected influence in the network; (3) Multiple variables showed associations with burnout components: workplace violence variables (threats-insults r = .42) were associated with emotional exhaustion, work-life imbalance (r = −.14) was negatively associated with emotional resources, sleep problems were associated with burnout dimensions (r = .24), while satisfaction domains showed negative associations with burnout; (4) Network structures differed significantly between professions (M = 0.2289, P = .0099), though overall similarity was moderate to high (ρ = 0.685). Nurses showed higher expected influence for job stability, while physicians showed higher expected influence for marital status.
Limitations and Strengths
Several methodological constraints should be considered. The cross-sectional design prevents causal inference, precluding any conclusions about temporal sequences or directional relationships among variables. Data collection occurred in 2016, predating the COVID-19 pandemic, which may limit applicability to current healthcare contexts where burnout dynamics may have shifted. Peru’s healthcare system specificity may limit generalizability to other cultural contexts, particularly developed regions with different resource constraints. Variable selection was constrained by the original survey design, potentially omitting important components such as organizational climate or colleague support. Comparisons were limited to physicians and nurses, excluding other healthcare workers. The SPIRAL model proposed in this study is exploratory and hypothesis-generating, requiring prospective validation before clinical or policy application.
Despite limitations, this study demonstrates notable strengths. The large, nationally representative sample (4951) provides comprehensive population-level insights, contrasting with convenience sampling approaches in most burnout research. Network analysis methodology, reinforced by robust stability procedures (CS = 0.75), ensures reliable identification of central nodes and association patterns consistent with burnout’s complex adaptive nature.
Interpretations of Findings
Through our network analysis, burnout components showed patterns of association consistent with complex interactions, which may challenge traditional linear conceptualizations. 9 This is consistent with the theory of complex adaptive systems, which posits that mental phenomena may emerge from self-organized interactions between individuals and their environment, rather than sequential symptom progression. 25 Organizational dimensions (income, management satisfaction) showed the highest expected influence and positioned centrally. In contrast, mental health symptoms were positioned peripherally, which is consistent with the notion that burnout may represent maladaptive responses to systemic rather than individual processes. 26 This pattern is consistent with findings that organizational interventions show minimal effects when they do not address central nodes such as income. 27
We observed network differences between nurses and physicians, which suggests potential profession-specific patterns in burnout-related associations.2,9 Nurses showed higher centrality for job stability and management satisfaction, while physicians showed higher centrality for income and personal factors (marital status, companionship). Network associations with violence exposure also differed between professions. Among nurses, violence exposure showed stronger associations with work dissatisfaction variables, while among physicians, violence exposure was more strongly associated with cynicism dimensions, consistent with documented avoidant coping styles. 28 These observed differences are consistent with the possibility that generic interventions may be ineffective due to profession-specific network structures, suggesting potential value in profession-specific interventions based on network structure, though this requires empirical testing.
Lastly, our network structure findings are consistent with burnout as an equifinality phenomenon, wherein multiple network configurations may associate with similar outcomes. The network showed multiple structural patterns associated with each core burnout dimension, which is consistent with critiques of linear models that position cynicism as the initial stage. 6 Violence exposure showed strong associations with cynicism nodes, organizational dysfunction was associated with emotional exhaustion, and inadequate support was associated with reduced self-efficacy. These distinct network profiles are consistent with the hypothesis that different burnout routes may exist,29,30 and suggest that interventions may benefit from targeting the specific network structures most relevant to each pattern. The identification of multiple network configurations supports a framework acknowledging diverse structural patterns in burnout, expanding conceptualization beyond linear progression toward pattern-specific intervention approaches.
Implications
Based on observed associations in our cross-sectional network data, we propose a preliminary, hypothesis-generating framework: the SPIRAL model. It comprises 6 theoretically informed network configurations that emerged from our analysis (Table 1). We emphasize that these patterns are exploratory observations requiring longitudinal validation. They should not be interpreted as confirmed pathways or causal mechanisms, but rather as potential areas for future investigation.
The SPIRAL Model of Burnout (Exploratory Framework Based on Observed Cross-Sectional Associations).

Note.Arrows (→) indicate proposed directional relationships not demonstrated in this cross-sectional analysis.
Hypothetical cascades represent theoretical temporal sequences requiring prospective longitudinal validation.
The Social isolation pattern is characterized by co-occurring associations between weak social connections, compromised work-life balance, diminished self-efficacy, and burnout components. The Personal vulnerability pattern showed strong associations between underlying mental health indicators (depressive symptoms, sleep problems) and emotional exhaustion. The Income deprivation pattern, particularly prominent among early-career healthcare workers, showed associations among job instability, low monthly income, increased workload demands, and burnout symptoms.
The Resource and organizational dysfunction pattern showed associations between perceived organizational failures and management dissatisfaction, which further associated with general professional dissatisfaction, reduced self-efficacy, and emotional exhaustion. The Assault and violence pattern showed workplace violence exposure associating most strongly with cynicism dimensions, which in turn were associated with broader burnout syndrome components. The Leadership trap pattern is characterized by associations among career advancement, increased responsibility, excessive working hours, disrupted sleep patterns, compromised work-life balance, and emotional exhaustion.
Conclusions
This network analysis of 4951 Peruvian healthcare workers examined burnout as a complex adaptive system wherein organizational factors (management satisfaction, income) showed highest expected influence, while individual mental health symptoms occupied peripheral positions. Network structures differed statistically across professions, with observed differences in centrality patterns between nurses and physicians. We propose a preliminary SPIRAL framework identifying 6 network-based patterns as potential areas for hypothesis generation regarding burnout development. These findings are consistent with critiques of traditional linear burnout conceptualizations and provide preliminary observations for hypothesis generation regarding targeted, systems-based interventions. Prospective longitudinal research is needed to validate temporal sequences and establish causal relationships among the variables and patterns identified in this cross-sectional analysis.
Supplemental Material
sj-doc-1-inq-10.1177_00469580261433856 – Supplemental material for Network Analysis of Healthcare Worker Burnout: Organizational Factors Show Highest Centrality
Supplemental material, sj-doc-1-inq-10.1177_00469580261433856 for Network Analysis of Healthcare Worker Burnout: Organizational Factors Show Highest Centrality by Javier A. Flores-Cohaila, Brayan Miranda-Chávez and Cesar Copaja-Corzo in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-docx-1-inq-10.1177_00469580261433856 – Supplemental material for Network Analysis of Healthcare Worker Burnout: Organizational Factors Show Highest Centrality
Supplemental material, sj-docx-1-inq-10.1177_00469580261433856 for Network Analysis of Healthcare Worker Burnout: Organizational Factors Show Highest Centrality by Javier A. Flores-Cohaila, Brayan Miranda-Chávez and Cesar Copaja-Corzo in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-pdf-1-inq-10.1177_00469580261433856 – Supplemental material for Network Analysis of Healthcare Worker Burnout: Organizational Factors Show Highest Centrality
Supplemental material, sj-pdf-1-inq-10.1177_00469580261433856 for Network Analysis of Healthcare Worker Burnout: Organizational Factors Show Highest Centrality by Javier A. Flores-Cohaila, Brayan Miranda-Chávez and Cesar Copaja-Corzo in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Author Contributions
JAFC: Conceptualization, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing—original draft, Writing—review & editing. BMC: Supervision, Visualization, Writing—original draft, Writing—review & editing. CCC: Funding acquisition, Supervision, Writing—original draft, Writing—review & editing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Universidad San Ignacio de Loyola financed the article processing charge (Code: USIL-2025). Funding Acquisition was by authors C.C.C. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The dataset analyzed in this study is publicly available through Peru’s Ministry of Health National Healthcare Worker Survey database (ENSUSALUD: ![]() ). Individual-level data supporting the findings of this study are available from the corresponding author upon reasonable request, subject to institutional data sharing agreements.
). Individual-level data supporting the findings of this study are available from the corresponding author upon reasonable request, subject to institutional data sharing agreements.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.