
Abstract
Relative deprivation has been associated with adverse health outcomes, yet the psychological pathways linking perceived socioeconomic disadvantage to health remain insufficiently understood, particularly in the Chinese context. This study therefore examines whether subjective well-being mediates the relationship between relative deprivation and health among Chinese adults. This cross-sectional study analyzed 5604 adults aged ≥ 18 using data from the 2023 Chinese General Social Survey (CGSS) conducted in China. After computing descriptive statistics and correlations, stepwise regression models tested whether subjective well-being mediated the relationship between relative deprivation and health. Indirect effects were estimated using bias-corrected bootstrap procedures (5000 replications). Urban-rural stratification examined geographic heterogeneity in mediation pathways, while robustness checks included ordered logit models and a sensitivity analysis that dichotomized subjective well-being into low and high categories. STATA 18.0 was used throughout. The results indicated that relative deprivation demonstrated a significant negative association with Chinese adults’ health. Furthermore, subjective well-being was independently associated with better health outcomes. Mediation analysis revealed that subjective well-being significantly mediated 20.5% of the total effect between relative deprivation and health. Regional stratification showed that the indirect pathway through subjective well-being did not differ significantly between urban and rural residents, whereas the direct effect of relative deprivation on health was significantly stronger among rural residents. These findings highlight the potential role of subjective well-being as a psychological mechanism linking perceived relative deprivation to health. While this pathway appears comparable across urban and rural contexts, the association between relative deprivation and health is stronger among rural residents. Addressing health disparities therefore requires attention to both psychosocial processes and the broader structural conditions that shape socioeconomic inequality.
Introduction
The widening wealth gap has become a defining challenge of contemporary society, profoundly reshaping public health paradigms across the globe. 1 According to the World Bank, the global Gini coefficient declined from 70 in 1990 to 62 in 2019, yet the COVID-19 pandemic triggered the largest single-year reversal on record, with the coefficient surging to 62.6 in 2020. 2 This disparity is not merely an economic concern but a critical public health issue, as emerging evidence suggests that perceived inequality in addition to absolute poverty is associated with adverse population health outcomes.3 -5 Particularly alarming is the phenomenon of relative deprivation, in which individuals assess their socioeconomic standing through social comparison with others. 6 This perception of disadvantage can lead to subjective well-being and adverse health consequences, even when basic material needs are met. 7 This issue is especially pronounced in rapidly developing economies undergoing dramatic social stratification. 8
In China, the Gini coefficient surged from 0.30 in 1980 to 0.57 in 2020,9,10 and regional disparities in health resources remain stark. This dual burden of economic and healthcare inequality has contributed to widening health gaps across groups. 11 These inequalities not only limit access to resources but also create psychosocial stress through social comparison. 12 Moreover, China’s rapid urbanization and market-oriented reforms have intensified social stratification.13,14 The coexistence of traditional collectivist values emphasizing social harmony with growing income disparities may present a unique psychological context. This perceived inequality has distinctive implications for well-being and health.4,13
In recent decades, China has implemented a range of policies aimed at reducing inequality and improving population health, such as targeted poverty alleviation programs, 15 expanded medical insurance coverage,16,17 and public health service equalization.15,18 Despite these policy efforts, the psychosocial consequences of perceived socioeconomic disadvantage have received comparatively limited attention. Given China’s large and rapidly transforming population, understanding how perceived inequality influences health has become increasingly important for informing public health strategies.
Relative deprivation refers to the subjective perception of disadvantage arising from upward social comparison, wherein individuals evaluate their position relative to others in their reference group. 19 In practice, such reference groups are typically composed of socially proximate others, such as individuals of similar age, socioeconomic position, or living within the same social environment. 20 Empirical research further suggests that age and socioeconomic characteristics are particularly salient dimensions in the construction of comparison groups in well-being research. 21 Relative deprivation as a psychological construct encompasses both cognitive appraisals of unfair disadvantage and affective responses such as resentment, frustration, and hopelessness. 22 Research has demonstrated that individuals experiencing relative deprivation report poorer self-rated health and elevated risks of chronic diseases,23,24 even after controlling for absolute income and other socioeconomic indicators. 25 These effects are theorized to operate through both physiological stress responses and behavioral pathways.24,26
Therefore, understanding the mechanisms through which relative deprivation affects health requires attention to psychological processes. Subjective well-being encompasses individuals’ cognitive and affective evaluations of their lives, including life satisfaction, positive emotions, and psychological comfort.27,28 Extensive evidence demonstrates that higher subjective well-being is associated with better health outcomes, including lower mortality rates and reduced risk of chronic diseases.29 -32 Social comparison theory suggests that relative deprivation erodes subjective well-being by generating feelings of dissatisfaction, resentment, and diminished self-worth.33 -35 Diminished well-being, in turn, may compromise health through chronic stress activation, 36 adoption of unhealthy coping behaviors, 37 and reduced health-promoting activities. 38 Thus, subjective well-being represents a plausible psychological pathway linking relative deprivation to health outcomes.
Despite theoretical support for this mediation model, empirical evidence remains limited. Most studies on the relationship between relative deprivation and health have been conducted in Western contexts. 39 In contrast, China’s rapid socioeconomic transformation, widening income inequality, and institutional arrangements such as the urban–rural divide may intensify social comparison processes and heighten individuals’ sensitivity to relative disadvantage. 40 These structural conditions suggest that relative deprivation may play a salient role in shaping subjective well-being and health outcomes in China. Existing studies in China have largely focused on specific subpopulations, such as rural migrant adolescents or urban residents (eg, Xiong and Johnson 41 and Wood and Gough 42 ), while research based on nationally representative samples remains scarce.
Against this backdrop, this study examines the relationship between relative deprivation and health among Chinese residents using nationally representative data from the Chinese General Social Survey (CGSS 2023). Specifically, the analysis investigates whether relative deprivation impairs health and whether subjective well-being mediates this relationship. The research framework of the study is illustrated in Figure 1. Beyond economic disparities, urban and rural contexts in China differ in social capital, 43 migration experiences shaped by the hukou system, 43 and community norms. 44 These contextual differences may shape social comparison processes and perceptions of relative deprivation. Accordingly, this study further examines potential regional heterogeneity by conducting separate analyses for urban and rural residents. Theoretically, by empirically testing subjective well-being as a mediator, this study advances understanding of the psychosocial mechanisms through which perceived relative deprivation affects health. Practically, these findings would inform whether interventions need to address not only material deprivation but also the psychological consequences of perceived inequality in promoting population health amid widening economic disparities.
Research framework.
Literature Review
Social Comparison Theory
Social comparison theory, introduced by Festinger, 33 refers to the human tendency to evaluate oneself by comparing with others. Within broader social contexts, individuals often assess their abilities, opinions, and personal attributes in relation to those around them. 45 Such comparisons function as an important mechanism for self-evaluation, enabling individuals to understand their relative position among peers and shaping their perceptions of self-worth. 46 According to social comparison theory, individuals evaluate their circumstances not only based on objective conditions but also relative to the situations of others. When individuals perceive themselves as disadvantaged compared with relevant reference groups, such comparisons may give rise to perceptions of relative deprivation.
Among the various forms of social comparison, individuals frequently engage in comparisons that place themselves at a disadvantage.47 -49 In contemporary societies characterized by extensive digital connectivity and mass communication, opportunities for social comparison have expanded substantially, enabling individuals to compare themselves with others across a wide range of social contexts. 50 Evidence from meta-analytic research indicates that people show a consistent tendency to make such unfavorable comparisons, even when these evaluations may undermine their own self-perceptions. 51 This pattern suggests that social comparison processes can generate feelings of status-related anxiety.52,53
These comparisons may foster feelings of relative deprivation, defined as the perception of being disadvantaged compared with others, particularly in terms of income inequality.54,55 Such perceptions of disadvantage function as psychosocial stressors arising from perceived unfairness. 34 This stress may affect health directly by elevating allostatic load, the accumulated physiological strain associated with chronic stress, or indirectly through maladaptive coping behaviors, including smoking and excessive alcohol use.54,56 Moreover, a growing body of research indicates that relative deprivation is associated with lower subjective well-being and related psychosocial outcomes, including reduced life satisfaction, meaning in life, social relationships, and prosocial orientations across both adult and younger populations.7,57 -59 In this sense, social comparison theory provides a useful framework for understanding how perceived relative disadvantage emerges and how it may influence psychological and health-related outcomes.
Relative Deprivation and Health
Relative deprivation can be conceptualized in both objective and subjective terms. 7 Objective relative deprivation refers to individuals’ position in the income distribution within a relevant reference group, often measured using personal or household income data.60,61 In contrast, subjective relative deprivation reflects individuals’ perceived disadvantage relative to others in social comparison processes.62 -64 The present study focuses on subjective relative deprivation arising from comparisons with peers of similar age, as age plays a key role in shaping reference groups for well-being comparisons. 21
Extensive research has documented the adverse health consequences of relative deprivation across diverse populations and contexts.19,65 -67 Study in America has also shown that individuals perceiving themselves as economically disadvantaged relative to others report poorer self-rated health, independent of their absolute income levels. 64 For instance, Christine et al 68 found that relative deprivation was associated with increased risks of depression and anxiety, even after controlling for household income and other socioeconomic factors. Similarly, longitudinal research has demonstrated that sustained exposure to relative deprivation predicts higher rates of heart failure hospitalization 69 and all-cause mortality. 70 In the Chinese context, emerging studies among specific subgroups such as rural-to-urban migrants and elderly populations have suggested similar patterns, with relative deprivation associated with compromised physical and mental health.71,72 Accordingly, this study proposes hypothesis 1:
Relative Deprivation and Subjective Well-Being
Individuals evaluate their circumstances not in absolute terms but relative to salient reference groups. 33 Upward comparisons, in which individuals perceive themselves as disadvantaged compared to these reference groups, generate negative emotional and cognitive responses.73,74 Studies across diverse societies have shown that relative deprivation is associated with lower life satisfaction, reduced positive affect, and heightened negative affect.7,34,75 These psychological consequences arise from multiple sources: feelings of injustice,71,76 diminished self-esteem, 72 self-efficacy, 77 and heightened anxiety. 78 Similar patterns have also been observed among younger populations, where relative deprivation is related to a reduced sense of meaning in life and weaker prosocial orientations.57 -59 Recent studies among Chinese residents have found that relative deprivation significantly predicts lower life satisfaction and subjective well-being,75,79 suggesting the relevance of this relationship in the Chinese context. Therefore, hypotheses 2 is proposed:
Subjective Well-Being and Health
The positive relationship between subjective well-being and health has been well-established across multiple disciplines. Meta-analytic evidence indicates that individuals with higher subjective well-being exhibit significantly lower mortality rates. 80 Prospective studies have shown that subjective well-being predicts better cardiovascular health, stronger immune function, and faster recovery from illness.30,81,82 Several mechanisms account for these protective effects. Physiologically, positive psychological states are associated with lower levels of inflammatory markers, more favorable cortisol patterns, and enhanced immune response.83,84 Behaviorally, individuals with higher subjective well-being are more likely to engage in health-promoting activities such as regular exercise, balanced nutrition, and preventive healthcare utilization.85,86 In China, research has demonstrated similar associations, with subjective well-being predicting better self-rated health and lower risks of chronic conditions.87,88 Accordingly, hypothesis 3 is proposed:
The experience of relative deprivation is associated with elevated subjective well-being levels and self-reported health decline.6,19 For example, Sharimakin and Ojewumi, 89 using survey data collected from 415 working adults across different occupations in Ondo State, Nigeria, examined the relationships among deprivation, subjective well-being, and health. Their findings indicate that individuals experiencing stronger feelings of deprivation report poorer physical and mental health outcomes, while subjective well-being plays an important role in shaping these health outcomes. These findings highlight the close interconnections between relative deprivation, subjective well-being, and health. Given China’s unique socioeconomic transformation, institutional arrangements, and patterns of social comparison, it remains unclear whether similar mechanisms operate among Chinese residents. To address this issue, the present study examines subjective well-being as a potential mediating mechanism linking relative deprivation and health. Integrating these elements, this study proposes the following hypothesis:
Methods
This study was reported in accordance with the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines 90 for cross-sectional studies.
Participants
This study draws on the 2023 Chinese General Social Survey (CGSS 2023), a nationally representative social science dataset jointly administered by Renmin University of China and partner institutions, which employed stratified multi-stage probability proportional sampling across all 31 provincial-level regions to collect 11 326 respondents. The analysis focused exclusively on adults aged 18 and above with complete measures of self-rated health, subjective well-being, and relative deprivation, applying listwise deletion to exclude cases with missing data on these key variables or control measures.
Measures
Dependent Variable: Health
This study employed self-rated health as the dependent variable to assess health outcomes among Chinese adults, following established practices in prior research. 91 Self-rated health was measured on a five-point Likert scale (1 = “Very unhealthy” to 5 = “Very healthy”) in CGSS 2023. After appropriate coding (so that higher scores indicate better health status), the variable ranged from 1 to 5. Self-rated health has been widely validated as a robust predictor of mortality and morbidity in population studies. 92
Independent Variable: Relative Deprivation
Relative deprivation was measured using a self-reported item from the CGSS 2023: “Compared with people of your age, how would you rate your socioeconomic status?” Responses were recorded on a four-point scale: 1 = “Higher,” 2 = “About the same,” 3 = “Lower,” and 9 = “Hard to say.” In the CGSS, this item captures respondents’ perceived socioeconomic standing relative to others of the same age. Age peers are often considered a meaningful comparison group, as such comparisons capture individuals’ subjective evaluation of their relative social standing and are consistent with the cognitive comparison processes emphasized in social comparison theory.20,33 In total, 621 respondents selected “Hard to say” and were excluded from the analysis because this category does not indicate a clear relative comparison. The remaining responses were recoded so that higher values indicate greater perceived relative deprivation, resulting in a three-point ordinal scale ranging from 1 (low deprivation) to 3 (high deprivation).
Mediating Variable: Subjective Well-Being
Following established practices by Qin and Li 93 in subjective well-being research, this study assessed subjective well-being using a single-item measure from the CGSS 2023: “Overall, do you feel your life is happy?” Response options were captured on a 5-point Likert scale: 1 = “Very unhappy”; 2 = “Relatively unhappy”; 3 = “Neither happy nor unhappy”; 4 = “Relatively happy”; 5 = “Very happy”, with higher scores indicating greater subjective well-being. To examine the robustness of the findings to alternative operationalizations, sensitivity analyses were conducted using a dichotomous classification of subjective well-being (low vs high well-being).
Control Variables
Gender is coded as a binary variable (0 = male, 1 = female). Age is treated as a continuous variable measured in years. Following common practice in Chinese social research, urban–rural status was defined based on respondents’ current place of residence. Individuals living in city centers or urban fringe areas were categorized as urban, whereas those living in towns or rural villages were classified as rural. Residence was coded as 0 for rural and 1 for urban. Because social comparison processes are embedded in individuals’ immediate living environments, 94 residence-based classification provides a relevant contextual indicator. Marital status is categorized into 4 groups: 1 for unmarried, 2 for married/cohabiting, 3 for divorced/separated, and 4 for widowed. Educational attainment is measured on an ordinal scale: 1 for junior high school or below, 2 for high school/vocational, 3 for junior college, 4 for bachelor’s degree, and 5 for postgraduate degree. Household income is log-transformed (ln (Income)) to account for its skewed distribution and treated as a continuous variable.
Statistical Analyses
Data analysis utilized the 2023 Chinese General Social Survey (CGSS 2023), yielding a final sample of 5604 adults aged 18 and above. Prior to analysis, we implemented comprehensive data cleaning procedures to identify outliers, missing values, and invalid responses, with incomplete cases excluded via listwise deletion to ensure internal consistency.
The analysis proceeded in 3 stages. First, descriptive statistics (means, standard deviations, frequencies, and percentages) were computed to characterize the sample and examine variable distributions, followed by Pearson correlation analysis to assess bivariate associations among key constructs. Second, stepwise multiple linear regression tested whether subjective well-being mediated the relationship between relative deprivation and self-rated health. Indirect effects were estimated using bias-corrected bootstrap procedures with 5000 replications in STATA 18.0, generating confidence intervals for mediation pathways. Third, regional heterogeneity by introducing interaction terms and conducting stratified analyses for urban versus rural subsamples were evaluated. To examine the robustness of the main findings, ordered logit models were estimated given the ordinal nature of subjective well-being and self-rated health, and sensitivity analyses were conducted by dichotomizing subjective well-being into low (very unhappy to neutral) and high (relatively happy and very happy) categories to assess the robustness of the results to alternative operationalizations of the mediator.
Results
Descriptive Statistics
Table 1 presents the descriptive statistics of the key variables and sample characteristics in this study. Health (M = 3.38, SD = 1.10, scale 1-5) was at a moderate level; Subjective well-being (M = 3.90, SD = 0.84, scale 1-5) indicated relatively high levels of well-being; relative deprivation (M = 2.31, SD = 0.55, scale 1-3) was concentrated at the middle-to-upper range of the scale. The sample had a mean age of 52.90 years (SD = 16.20), indicating a wide age span; the gender distribution was relatively balanced (50.93% female). Socioeconomic characteristics revealed substantial heterogeneity in household income (log income: M = 10.86, SD = 1.26), while educational attainment was generally low, with the majority of participants having completed junior high school or below (57.19%) and the remainder distributed across higher education levels. In terms of family and residential characteristics, most respondents were married or cohabiting (75.02%), and the proportion of rural residents (52.09%) slightly exceeded that of urban residents (47.91%).
Descriptive Statistics and Sample Characteristics (N = 5604).
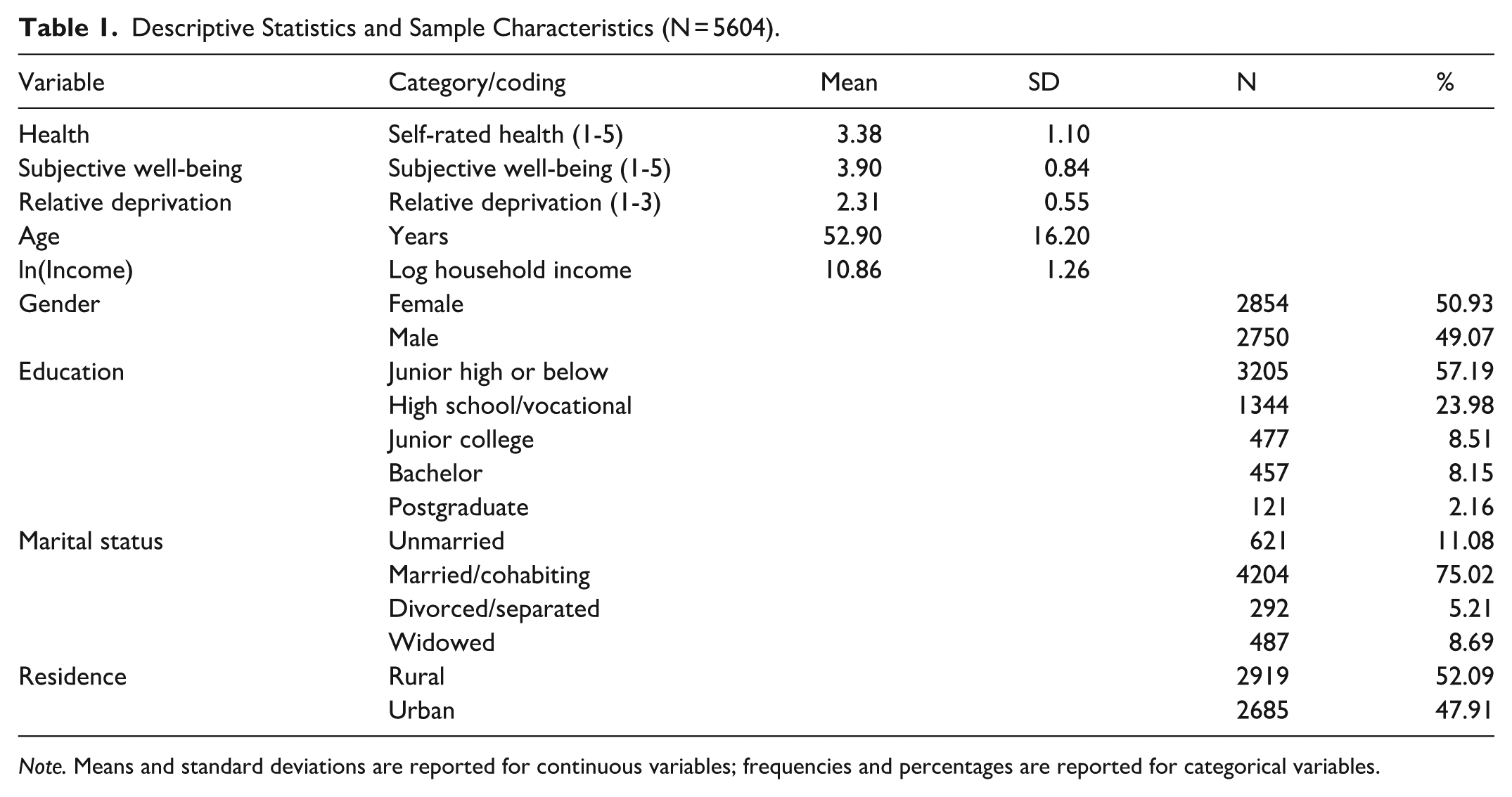
Note. Means and standard deviations are reported for continuous variables; frequencies and percentages are reported for categorical variables.
Correlation Analysis
Pearson’s correlation coefficients between the core variables are shown in Table 2. There was a negative correlation between relative deprivation and health level (r = −.223, P < .001), indicating that higher relative deprivation is associated with poorer health. Subjective well-being was statistically positively correlated with health level (r = .224, P < .001), consistent with the protective role of psychological well-being in health outcomes. In addition, relative deprivation was negatively associated with subjective well-being (r = −.242, P < .001), suggesting that individuals experiencing relative deprivation are more likely to perceive lower subjective well-being, which in turn may contribute to deteriorated health outcomes.
Correlation Analysis of Health, Relative Deprivation and Subjective Well-Being (N = 5604).

p < 0.01.
Test of the Mediating Effect of Subjective Well-Being Between Relative Deprivation and Health
In order to verify the mediating role of subjective well-being between relative deprivation and the health of adults, the 3-step stepwise regression method proposed by WEN and YE was used in this study 95 (see Table 3). Model 1 showed that, after controlling for variables such as gender, age, education, marital status, urban residence, and household income, a 1 standard deviation increase in relative deprivation was significantly associated with a 0.366-unit decrease in the health level of adults (β = −.366, P < .001), indicating a significant total association and supporting Hypothesis 1. Model 2 indicated a significant negative association between relative deprivation and subjective well-being among adults (β = −.316, P < .001), satisfying the prerequisite that the mediator must be statistically related to the independent variable.
Regression Analysis of Relative Deprivation and Subjective Well-Being on Health (N = 5604).
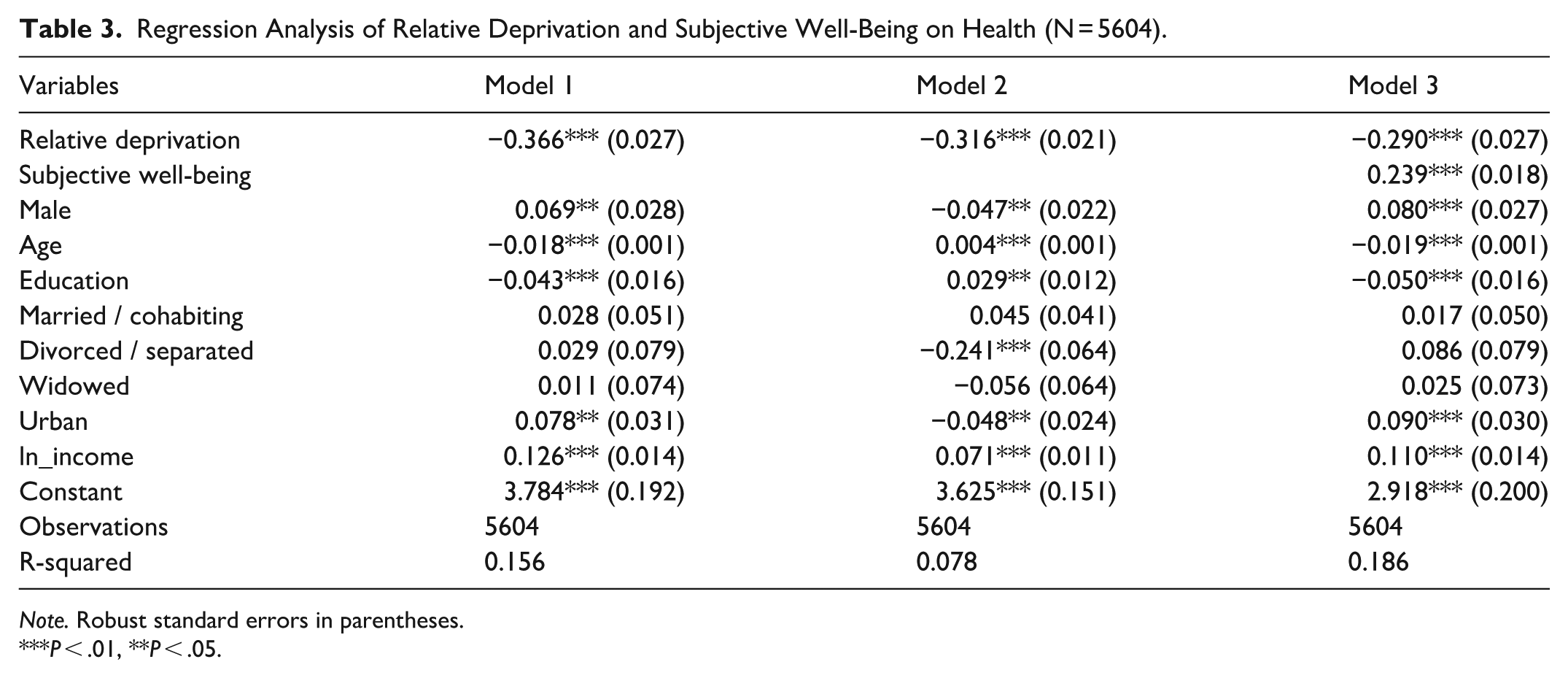
Note. Robust standard errors in parentheses.
P < .01, **P < .05.
Model 3 incorporates both relative deprivation and subjective well-being. Results showed that subjective well-being was significantly associated with higher health levels among adults (β = .239, P < .001), supporting Hypothesis 3. The direct association between relative deprivation and health level was reduced to −0.290 (P < .001), representing a 20.8% reduction ((0.366-0.290)/0.366), while remaining statistically significant. This pattern is consistent with the characteristics of partial mediation, suggesting that subjective well-being play a mediating role in the relationship between relative deprivation and health. The indirect association through subjective well-being was estimated at β = (−.316) × .239 = −.075, providing support for Hypothesis 2 and Hypothesis 4. To more intuitively illustrate the mediating role of subjective well-being, Figure 2 presents a path diagram.
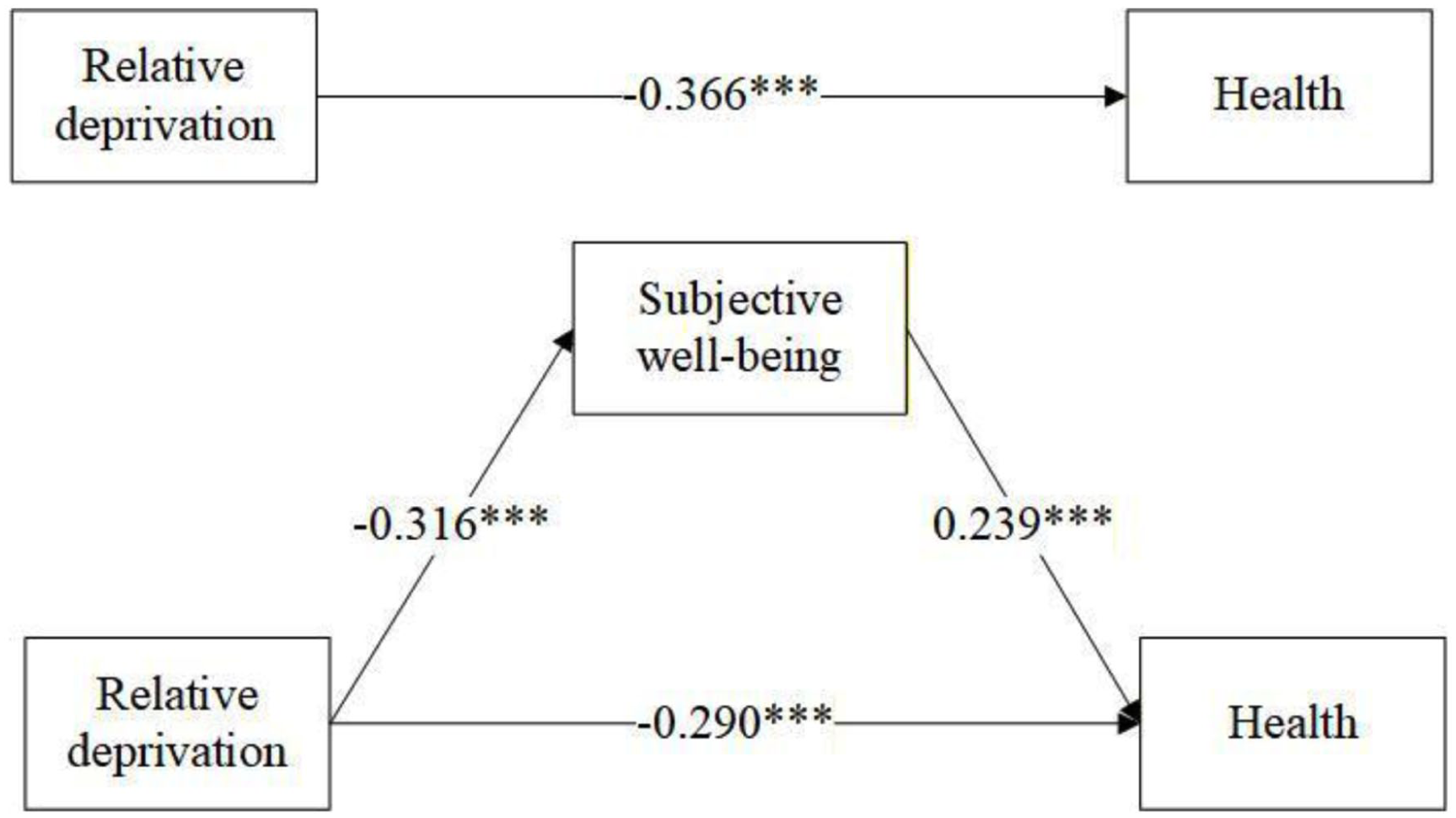
Path diagram of the mediated impact of subjective well-being between relative deprivation and health.
Mediating Pathway Analysis of Relative Deprivation, Subjective Well-Being and Health
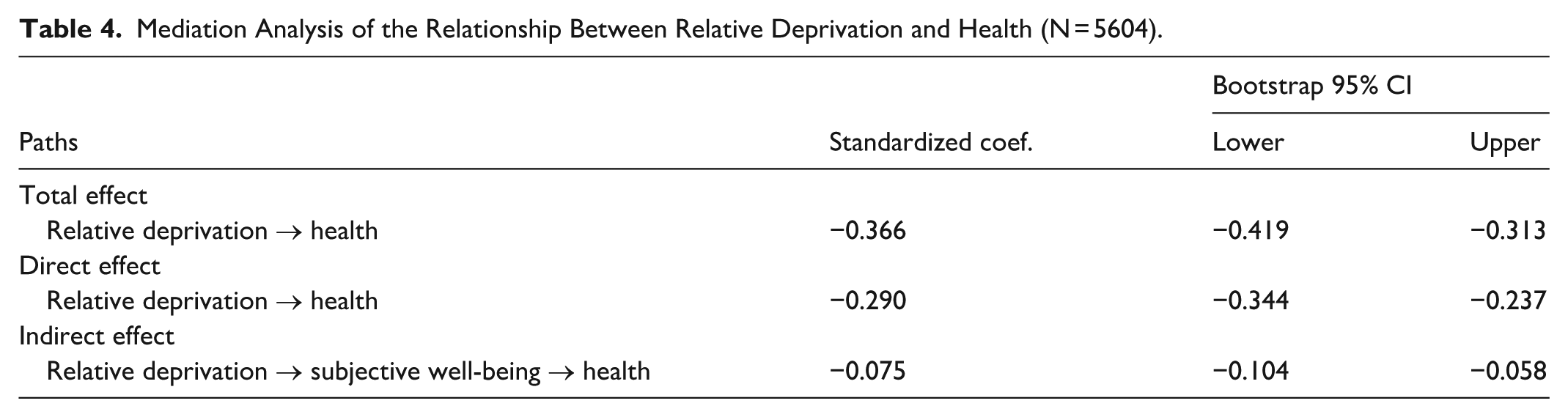
The mediating pathway was quantified using bias-corrected bootstrap procedures with 5000 replications. Results suggest that higher levels of relative deprivation are associated with lower levels of adult health (Table 4). Specifically, the standardized coefficient for the total effect was −0.366 (95% CI [−0.419, −0.313]), indicating that for each standard deviation increase in relative deprivation, the health of adults decreased by 0.366 standard deviation units on average; this effect can be decomposed into a direct effect (β = −.290, 95% CI [−0.344, −0.237]) and an indirect effect (β = −.075, 95% CI [−0.104, −0.058]), which accounted for 79.2% and 20.5% of the total effect, respectively, which further validated the robustness of the mediating pathway.
Mediation Analysis of the Relationship Between Relative Deprivation and Health (N = 5604).
Differences Between Groups by Region
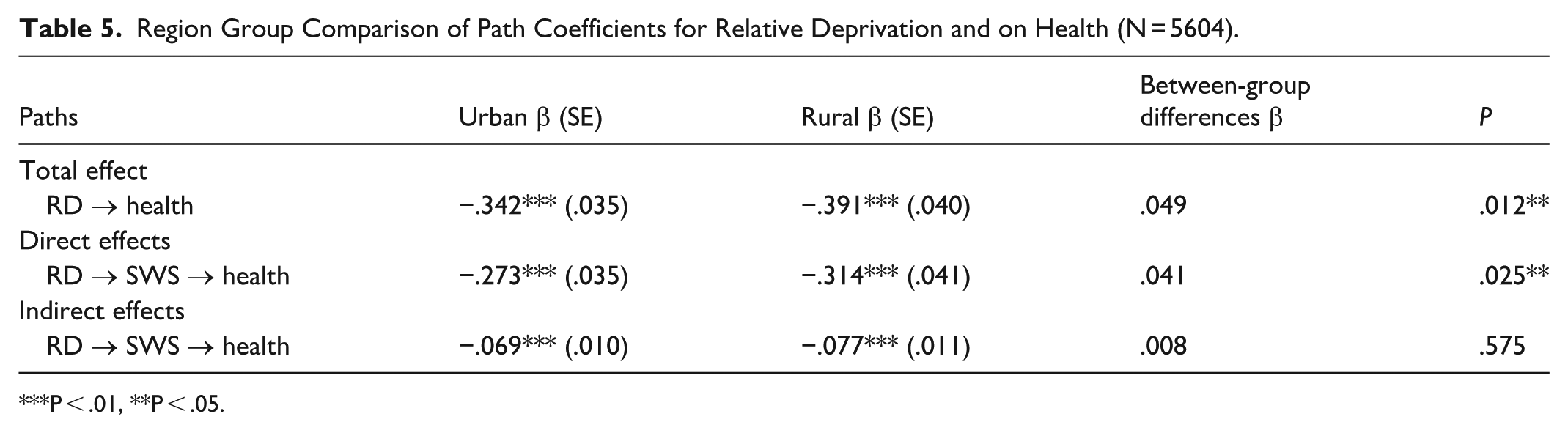
Given that health level and subjective well-being among adults may vary by region, subgroup analyses were conducted (urban vs rural; see Table 5). The grouping results showed that the total effect (β = −.342, SE = 0.035, P < .001) and direct effect (β = −.273, SE = 0.035, P < .001) were lower in absolute magnitude in the urban group than in the rural group (total effect β = −.391, SE = 0.040, P < .001; direct effect β = −.314, SE = 0.041, P < .001), and the differences between groups reached statistical significance (Δβ = .049, P = .012; Δβ = .041, P = .025). The key differences were centered on the direct effect pathway, with the strength of direct impact of relative deprivation on health being significantly stronger in rural than urban residents (β = −.314 vs −0.273, Δβ = .041, P = .025). In contrast, the indirect effect through subjective well-being showed similar magnitudes across regions (β = −.069 vs −.077, Δβ = .008, P = .575), suggesting that while the direct mechanisms of relative deprivation on health are region heterogeneous, the mediating pathway through subjective well-being appears to be similar across urban and rural contexts.
Region Group Comparison of Path Coefficients for Relative Deprivation and on Health (N = 5604).
P < .01, **P < .05.
Robustness Tests and Sensitivity Analyses
To examine the robustness of the main findings, ordered logit models were estimated given the ordinal nature of both subjective well-being and health. As shown in Table 6, the results remain substantively consistent with the baseline regressions. Relative deprivation is significantly negatively associated with subjective well-being (β = −.758, P < .001) and self-rated health (β = −.653, P < .001). After subjective well-being is included, the coefficient for relative deprivation decreases to −0.520 (P < .001), while subjective well-being remains positively associated with health (β = .449, P < .001), further supporting the mediating mechanism identified in the main analysis. The consistency of these findings across estimation methods indicates that the main results are robust to alternative model specifications.
Robustness Checks Using Ordered Logit Models (N = 5604).
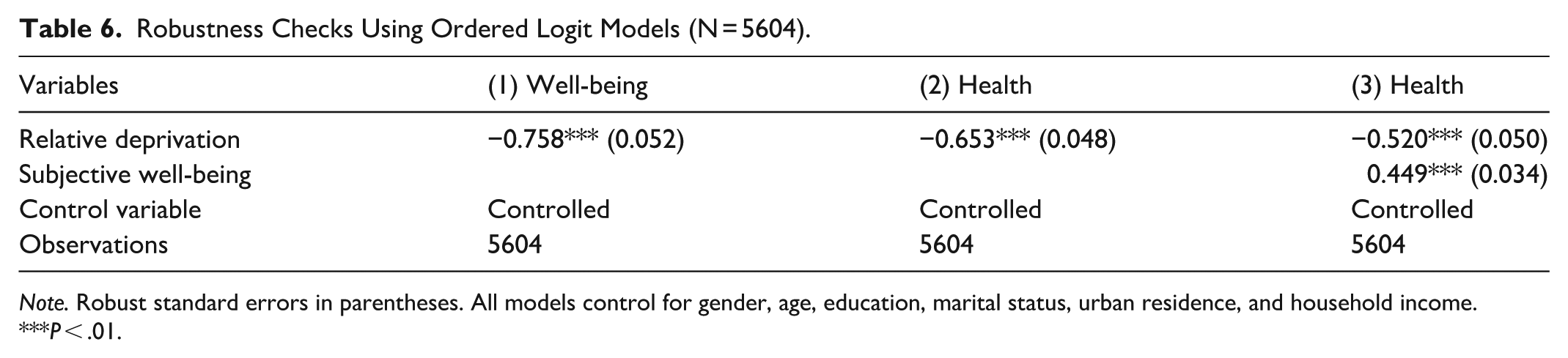
Note. Robust standard errors in parentheses. All models control for gender, age, education, marital status, urban residence, and household income.
P < .01.
In addition, a sensitivity analysis was conducted by dichotomizing subjective well-being into low (very unhappy to neutral) and high (relatively happy and very happy) categories to examine whether the results were sensitive to alternative operationalizations of the mediator. As shown in Table 7, relative deprivation remains significantly negatively associated with health (β = −.366, P < .001). When subjective well-being is included in the model, the coefficient for relative deprivation decreases to −.331 (P < .001), while subjective well-being shows a significant positive association with health (β = .533, P < .001). These results suggest the presence of a partial mediating role of subjective well-being and remain consistent with the baseline findings.
Sensitivity Analysis: Relative Deprivation and Health (N = 5604).
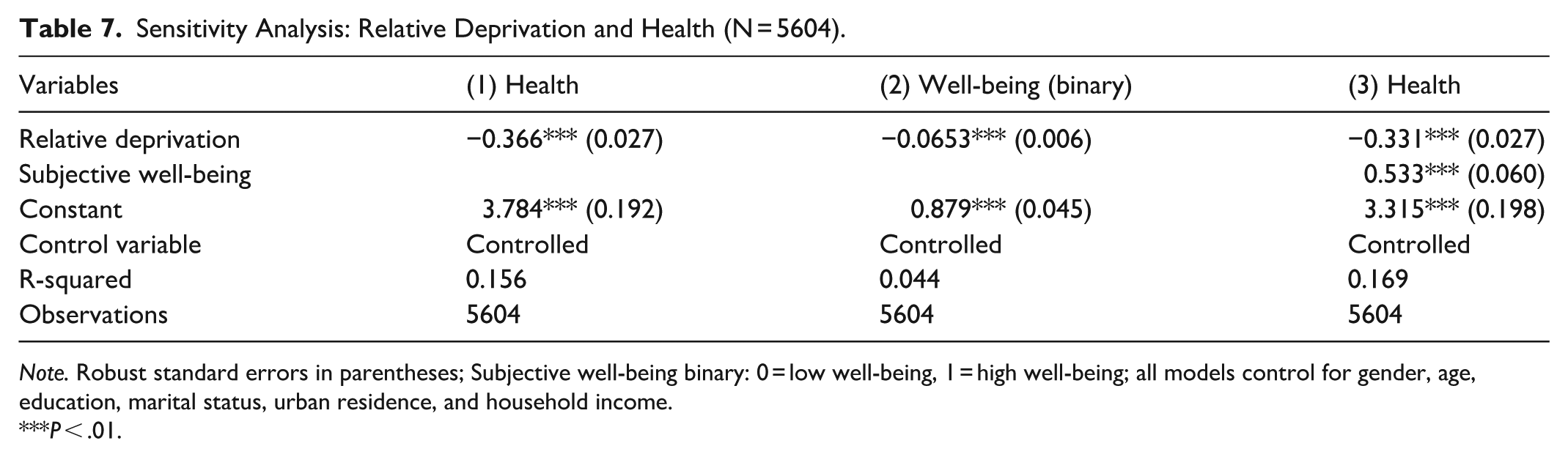
Note. Robust standard errors in parentheses; Subjective well-being binary: 0 = low well-being, 1 = high well-being; all models control for gender, age, education, marital status, urban residence, and household income.
P < .01.
Discussion
Against the backdrop of rising income inequality in China, this study provides empirical evidence that relative deprivation is negatively associated with self-rated health among Chinese adults, and that subjective well-being constitutes an important pathway linking perceived social disadvantage to health. By integrating insights from social comparison theory with nationally representative data, the findings highlight the relevance of psychosocial mechanisms in shaping health outcomes beyond objective socioeconomic conditions. These results contribute to a growing body of literature emphasizing that health inequalities are not only materially grounded but also socially and psychologically constructed.
First, relative deprivation significantly predicts poorer self-rated health among Chinese adults. This extends previous findings64,68,69 to the Chinese context and supports the theoretical proposition that subjective social standing matters beyond objective socioeconomic indicators. The results confirm similar patterns in China, suggesting that relative deprivation operates as a critical health determinant across diverse societal contexts. This challenges purely material-based explanations of health inequalities and highlights the need for interventions addressing perceived social disadvantage in rapidly developing economies. 64
Second, subjective well-being emerges as a predictor of health outcomes. Consistent with meta-analytic evidence, 80 the findings demonstrate that higher subjective well-being is associated with better self-rated health among Chinese adults. These findings align with prior research in China87,88 and underscore the importance of psychological well-being in public health strategies. This finding further highlights the close linkage between individuals’ subjective evaluations of life and their perceived health status.
Third, subjective well-being mediates the relationship between relative deprivation and health. While social comparison theory posits that upward social comparisons generate negative psychological responses, the empirical analysis demonstrates the specific pathway through which these responses translate into health outcomes. This mediation mechanism suggests that the health costs of income inequality operate not merely through material deprivation but also through psychological pathways. 25 Unlike absolute poverty, which primarily constrains access to material resources, relative deprivation may influence health through psychological well-being.
In addition, regional heterogeneity analysis further revealed that the mechanisms through which relative deprivation influences health outcomes operate similarly across urban and rural contexts. The indirect effect through subjective well-being showed no regional difference, suggesting that while the overall impact and direct pathway vary by regional conditions, the psychological mediation pathway operates uniformly across contexts. The psychological burden of perceived socioeconomic disadvantage appears to be a fundamental human response that transcends urban-rural differences. However, the stronger association observed in rural areas may reflect structural constraints and more localized social comparison processes, where limited economic opportunities and closely knit reference groups may amplify the consequences of perceived deprivation for health. 96
Implication and Limitation
This study makes several important contributions with both theoretical and practical implications. Theoretically, this study extends social comparison theory to the Chinese context by highlighting the potential role of subjective well-being as a psychological pathway linking perceived socioeconomic disadvantage to health. By showing that perceptions of relative standing are associated with health through psychosocial processes, the findings underscore the importance of considering subjective experiences of inequality rather than focusing solely on objective socioeconomic conditions when examining health disparities. From a practical perspective, the results suggest that efforts to reduce health inequalities should address not only material deprivation but also the psychological consequences of perceived disadvantage. Interventions that enhance subjective well-being, including improved access to mental health services and stronger community support, may complement broader structural efforts to reduce socioeconomic disparities.
However, several limitations should be acknowledged. First, the cross-sectional design precludes causal inference and does not establish the temporal ordering between relative deprivation, subjective well-being, and health, leaving open the possibility of reverse associations. Second, the use of single-item measures for subjective well-being and relative deprivation may not fully capture the multidimensional nature of these constructs. Third, the measure of relative deprivation focuses on comparisons with age peers and may not reflect other salient reference groups in everyday social comparisons, such as colleagues, neighbors, or community members. Fourth, the analysis is based on data from China, and cultural contexts may shape how individuals interpret status differences and perceive relative deprivation, which may limit the generalizability of the findings to other societies. Future research using longitudinal data, more comprehensive measures, and cross-cultural comparisons would help to further clarify these relationships.
Conclusion
This study highlights the potential role of subjective well-being as a psychological pathway linking perceived socioeconomic disadvantage to health among Chinese adults. The findings underscore the importance of considering subjective experiences of inequality when examining health disparities, suggesting that relative deprivation may represent an important dimension of health inequality beyond absolute poverty. Addressing health disparities therefore requires attention not only to material conditions but also to the psychosocial consequences of perceived disadvantage. As income inequalities continue to widen globally, understanding how perceptions of relative standing relate to health outcomes remains an important challenge for promoting population well-being.
Supplemental Material
sj-pdf-1-inq-10.1177_00469580261444668 – Supplemental material for Relative Deprivation and Health Among Chinese Adults: The Mediating Role of Subjective Well-Being
Supplemental material, sj-pdf-1-inq-10.1177_00469580261444668 for Relative Deprivation and Health Among Chinese Adults: The Mediating Role of Subjective Well-Being by Yingying Cai in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-xls-2-inq-10.1177_00469580261444668 – Supplemental material for Relative Deprivation and Health Among Chinese Adults: The Mediating Role of Subjective Well-Being
Supplemental material, sj-xls-2-inq-10.1177_00469580261444668 for Relative Deprivation and Health Among Chinese Adults: The Mediating Role of Subjective Well-Being by Yingying Cai in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Ethical Considerations
Ethical review and approval were not required for this study in accordance with local legislation and institutional requirements. The study used publicly available data from the Chinese General Social Survey (CGSS), for which ethical approval and written informed consent were obtained at the time of data collection.
Author contributions
CYY conceptualized and designed the study, conducted the data analysis, interpreted the results, drafted the manuscript, revised it critically for important intellectual content, and approved the final version to be published. The author read and approved the final manuscript and takes responsibility for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets analyzed during the current study are available in the Supplemental Information files.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.