
Abstract
Introduction
Improving hospital care quality while controlling costs has become a major challenge in emerging healthcare systems. This study examines the relationship between hospital operational efficiency (HOE) and operational new quality productivity in hospitals (HONQP) and further investigates whether hospital dean overconfidence (HDO) moderates this relationship.
Methods
This study used panel data from 55 tertiary public hospitals in City A in China, from 2022 to 2025. HONQP was conceptualized as a multidimensional construct reflecsting innovation-driven, technology-enabled, and quality-oriented operational upgrading, and was measured using an entropy-weighted composite index. HOE was measured based on revenue-expenditure structure and cost-control indicators, while HDO was proxied by managerial demographic and positional characteristics. Fixed-effects regression models were employed to test the hypotheses, with additional robustness checks using dependent-variable replacement, random subsample regression, and propensity score matching.
Results
The results show that HOE is significantly and positively associated with HONQP. In addition, HDO significantly strengthens this positive relationship, indicating that managerial characteristics are relevant to the extent to which operational efficiency is associated with hospital operational upgrading. These findings remain robust across multiple alternative specifications and robustness tests. Heterogeneity analyses further show that the strength of the relationship varies across hospital type, affiliation, and regional economic development.
Conclusion
This study provides context-specific evidence that operational efficiency is an important driver of hospital operational upgrading and that HDO functions as a meaningful moderating factor. The findings contribute to hospital governance research and offer practical implications for leadership selection and operational reform in public hospitals.
Keywords
Introduction
In the current global economic system, the development of new quality productivity has emerged as a crucial driver of economic growth. 1 New quality productivity encompasses fields, such as information technology, artificial intelligence, green energy, and high-end manufacturing. These fields share common characteristics: they represent cutting-edge technological progress, 1 are driven by innovation, and exhibit high technology, high efficiency, and high quality, aligning with the advanced productivity of the new development concept. New quality productivity arises from revolutionary technological breakthroughs, innovative configurations of production factors, and profound industry transformations and upgrades. 2 It is based on advancements in workers, labor materials, labor objects, and their optimized combinations, marked by a significant increase in total factor productivity. It is characterized by innovation, driven by quality, and fundamentally represents advanced productivity.1,3
The health sector, as a frontier of scientific and technological innovation,4,5 is closely linked to the enhancement of human health. The development of new quality productivity in the health sector aligns with the ‘health first’ concept, prompting innovative configurations and systematic changes in all health sector factors. This will strongly promote Chinese-style health modernization and global health development. The development of public hospitals, a crucial component of the medical and health care system, is directly related to the vital interests of the population. Since the 18th National Congress of the Communist Party of China, rising living standards have led to increasing demands for advanced medical technology. Hospital operational efficiency, a key indicator of the healthy development of public hospitals, 6 significantly promotes operational new quality productivity in hospitals in areas such as performance reform, service model innovation, informatization, resource allocation, and quality control. However, currently, the operational efficiency of Chinese public hospitals is insufficient, characterized by high potential financial risks, rapid growth in medical expenses, and a weakening public welfare nature. 7 This situation contradicts the goals of public hospital managers, who aim to serve the people and promote the high-quality development of hospitals as mandated by the government. Therefore, studying hospital operational efficiency and operational new quality productivity in hospitals will effectively address this issue.
Growing interest has been garnered in examining the relationship between operational efficiency and new quality productivity in various fields, such as human resources,8,9 sustainable development,10,11 total factor productivity,12,13 operational efficiency and innovation performance,14,15 and green productivity.16,17 However, the literature has largely neglected the impact of operational efficiency and new quality productivity in the medical context. This highlights the novelty of the present study, which is to empirically delve into the relationship between hospital operational efficiency and new quality of hospital productivity. Meanwhile, hospital dean overconfidence (HDO) is anticipated to strengthen this relationship, advancing the body of knowledge by integrating this crucial factor in the proposed model. Although our model highlights dean overconfidence as a moderator, we recognize that hospital performance is a systemic outcome shaped by interdependent factors such as interdisciplinary team dynamics, institutional capacity, patient flow, and health policy frameworks. Therefore, the effect of managerial cognition should be interpreted as one component within a broader performance ecology.
To establish the relationship between hospital operational efficiency and operational new quality productivity in hospitals, we investigated the operations of 55 tertiary public hospitals in city A in China from 2022 to 2025 and constructed a dataset. City A was selected because it has a relatively complete tertiary public hospital system and provides a policy-relevant setting for examining hospital operational upgrading under ongoing healthcare reform. Our results indicated that hospital operational efficiency is positively related to operational new quality productivity in hospitals.
This study contributes significantly to academic literature in three key areas. First of all, it establishes a comprehensive theoretical framework for hospital operational efficiency and operational new quality productivity in hospitals, thereby strengthening existing research on hospital governance theory. Secondly, it examines the moderating effect of HDO on the relationship between hospital operational efficiency and operational new quality productivity in hospitals, further enhancing hospital governance theory. Finally, by integrating perspectives from psychology, behavioral economics, and hospital management within a context-specific single-city setting, this study advances the understanding of how managerial cognition interacts with operational efficiency to shape hospital operational upgrading, while also providing exploratory evidence for future comparative research across regions and healthcare systems.
Theory and Research Hypotheses
Hospital Operational Efficiency and Operational New Quality Productivity in Hospitals
Hospital operational efficiency refers to the hospital’s ability to efficiently utilize and manage resources such as human resources, materials, funds, time, information, and so forth in delivering medical services. 18 It reflects the hospital’s sophistication and enables scientific management.19,20 It entails the hospital’s effective organization and coordination of resources to achieve high efficiency and optimize medical service outcomes. The level of hospital operational efficiency directly impacts service quality, cost control, patient satisfaction, and overall hospital competitiveness.18,21 Hospital operational efficiency’s comprehensive performance manifests primarily in talent capital, scientific and technological innovation, and workforce outcomes. To begin with, hospitals with higher operational efficiency are more attractive in the talent market, drawing outstanding and high-quality talents to their ranks. These talents enhance hospital efficiency22,23 and elevate clinical and innovative capacities, thereby boosting hospital productivity. 19 Secondly, hospitals demonstrating superior operational efficiency indicators can drive dynamic innovation24,25 through advancements in technological innovation,26,27 service model innovation,28,29 and infrastructure development (e.g., new medical equipment, increased bed capacity, expansion of clinical and technical departments), fostering sustainable advancements in clinical technology. 26 This transformation results in the creation of advanced labor tools, establishing hospitals as crucial in driving operational new quality productivity. Thirdly, the implementation of operational management and the enhancement of operational efficiency in hospitals demonstrate that optimizing overall operational processes significantly enhances the quality and efficiency of hospital services.30,31 This improvement not only meets the evolving medical needs of the Chinese population but also achieves a higher level of balance between medical supply and demand, ultimately enhancing the whole operational productivity.
According to the above description, this study bridges classical and behavioral theories to explain hospital productivity. Specifically, Marxist productivity theory explains how material and human labor evolve to drive systemic productivity, the three core elements of operational new quality productivity in hospitals align with Marxist political economics’ three productivity elements 32 : high-quality talent capital for hospital operations, new quality labor tools through technological innovation (e.g., new infrastructure, enhanced hospital outputs), and the broadened scope of hospital operational objects (e.g., Internet hospitals, strategic industries). These elements interact synergistically to foster operational new quality productivity in hospitals, 32 thereby advancing under the influence of hospital operational efficiency. Based on the above analysis, we propose hypothesis H1.
Hospital operational efficiency positively influences new quality productivity in hospitals.
The Moderating Effect of Hospital Dean Overconfidence (HDO)
Although hospital operational efficiency is closely associated with the development of operational new quality productivity in hospitals (HONQP), the extent to which operational efficiency is translated into innovation-driven, technology-enabled, and quality-oriented operational upgrading may vary according to managerial characteristics. 32 According to upper echelons theory, organizational strategies and outcomes reflect the backgrounds and personal traits of senior managers, especially top leaders. 33 Different backgrounds and traits among top leaders are associated with different strategic orientations and managerial emphases when organizations face similar conditions. 34 In the context of public hospitals, hospital deans are the principal decision-makers responsible for hospital development and governance.6,35 Their personal traits may therefore be relevant to the strength of the relationship between hospital operational efficiency (HOE) and HONQP.
Overconfidence is a managerial trait characterized by an inflated assessment of one’s own abilities, judgment, or future prospects. 36 In upper echelons research, overconfidence is commonly regarded as a salient cognitive characteristic that is associated with more assertive strategic orientation and stronger emphasis on development, expansion, and innovation-related agendas.36-39 Within the context of this study, hospital dean overconfidence (HDO) is viewed not as an independent mechanism, but as a managerial characteristic that may shape the extent to which hospital operational efficiency is associated with the three dimensions of HONQP. Specifically, under conditions of higher HDO, hospital operational efficiency may be more strongly associated with high-quality talent capital, innovative productive resources, and expanded operational service capacity, which together constitute HONQP.40-43 In this sense, HDO is expected to strengthen the positive relationship between HOE and the multidimensional operational upgrading reflected in HONQP. Based on this rationale, we propose hypothesis H2.
HDO strengthens the positive relationship between hospital operational efficiency and new quality productivity in hospitals.
Building upon this foundation, the study developed a theoretical framework to explore the relationship between hospital operational efficiency and operational new quality productivity in hospitals, moderated by hospital dean overconfidence (see Appendix 6).
Methodology
Data, Sample Selection, and Analysis Tool
This study is designed as a context-specific observational panel study of tertiary public hospitals in city A, China (The city name is anonymized due to data access and institutional confidentiality requirements attached to the official records used in this study). In accordance with reporting standards for observational research, this study follows the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines, 44 and a completed STROBE checklist has been provided as a supplementary file. It examines the relationship between hospital operational efficiency and operational new quality productivity in hospitals using actual hospital-level data from 2022 to 2025.
The sample size was determined by the total number of tertiary public hospitals in the study setting that met the predefined inclusion criteria during the observation period. Specifically, this study adopted a context-specific full-sample approach rather than sample-based sampling, because the number of eligible tertiary public hospitals in city A was limited and institutionally bounded. Therefore, all hospitals that satisfied the inclusion criteria were included to maximize sample coverage and improve the representativeness of the local study setting. The inclusion criteria were as follows: (1) the hospital was classified as a tertiary public hospital in the relevant year; (2) complete economic operation data were available for the study period; and (3) information on the hospital dean was publicly available. The sample selection criteria were stringent, as we excluded hospitals with missing or incomplete data, those without information on hospital deans, and those affected by recent mergers due to medical reform. Furthermore, hospitals not rated as tertiary for the year were excluded to ensure consistency in hospital classification. To address outliers, extreme values of continuous variables were Winsorized at the 1st and 99th percentiles. After meticulous screening, data from 55 tertiary public hospitals were included in the analysis. Because this study used the full set of eligible hospitals within one city, a formal a priori sample size or statistical power analysis was not performed. Data were sourced from the actual economic operation index report files maintained by the Health Commission of City A and from official survey information disclosed on the websites of hospitals in City A. Data management and empirical estimation were conducted using Excel 2019, SPSSAU, and Stata 18.0.
Measures
Operational New Quality Productivity in Hospitals (HONQP)
The dependent variable in this study is operational new quality productivity in hospitals (HONQP), defined as a multidimensional construct capturing hospitals’ capability to achieve innovation-driven, technology-enabled, and quality-oriented operational upgrading. Unlike traditional measures of hospital efficiency or productivity that primarily focus on input–output performance, 45 HONQP emphasizes the qualitative transformation of hospital operations, including innovation capacity, digital and technological advancement, and the expansion of modern healthcare service functions.
The concept of HONQP is grounded in the three-factor productivity theory in Marxist political economics, which conceptualizes productivity as the combined result of labor, labor materials, and production conditions. 32 To situate this construct within the broader literature, the study further incorporates insights from research on Total Factor Productivity (TFP), which emphasizes efficiency in resource allocation,43,46,47 Green Productivity, which highlights sustainable and innovation-oriented development,42,48 and smart healthcare transformation, which focuses on the role of digitalization and technological innovation in healthcare systems.40,41,49 Through this integration, HONQP extends existing productivity and innovation frameworks by providing a context-specific perspective on hospital operational upgrading.
Based on this integrated framework, HONQP is operationalized through three dimensions. High-quality talent capital represents the labor component and reflects the extent to which hospitals possess advanced human capital for innovation and high-quality service delivery, measured by indicators such as the proportion of senior professionals, academic qualifications, and key specialties. Innovative productive resources correspond to the material component and capture the technological and infrastructural basis of operational upgrading, including intelligent medical equipment, digital platforms, technological outputs, and patent activity. Expanded operational service capacity reflects changes in production conditions and denotes the hospital’s ability to extend and reconfigure service boundaries through initiatives such as internet hospitals, strategic service units, and participation in regional medical alliances.
To ensure empirical validity, the study conducted a reliability and validity analysis of the HONQP measurement scale. The Cronbach’s alpha coefficients for each dimension exceeded 0.7, indicating good internal consistency. Factor loadings were mostly above 0.6, and communality values ranged from 0.59 to 0.78. No cross-loadings or negative loadings were observed, suggesting strong construct validity. Quantitatively, HONQP is calculated using the entropy weighting method,50,51 which assigns indicator weights based on their informational contribution (see Appendix 1). These weighted scores are then aggregated to compute the overall HONQP index. It is important to note that HONQP is not proposed as a theoretical innovation, but rather as a context-specific operationalization of productivity theory, tailored to the transformation goals of China’s healthcare reform. It provides a structured, empirically grounded framework for evaluating hospital innovation capacity under a socialist market healthcare system.
Hospital Operational Efficiency (HOE)
The independent variable in this study is hospital operational efficiency (HOE). According to the “Opinions on Strengthening the Performance Assessment of Tertiary Public Hospitals” issued by the General Office of the State Council of China in 2019, hospital operational efficiency indicators encompass resource efficiency, revenue and expenditure structure, cost control, and economic management, comprising 19 indicators. 6 This study focuses on the revenue and expenditure structure, and cost control indicators to define hospital operational efficiency,6,52 using a combined assignment method for measurement. Initially, the APH hierarchical method computes weights for the three-level indicators, followed by the entropy method for the second-level indicators. 53 Ultimately, hospital operational efficiency is computed through weighted summation using the combined assignment method. Detailed indicator values can be found in Appendix 2.
Hospital Dean Overconfidence (HDO)
The moderating variable in this study is Hospital Dean Overconfidence (HDO). Overconfidence, as a key psychological trait in managerial behavior, has been extensively studied in organizational and behavioral research. Scholars have developed multiple approaches to measure managerial overconfidence, including:Personality scale measurements54,55; Media-based evaluations, such as press coverage and tone analysis56,57; Relative salary comparisons, where CEO pay relative to peers is taken as a sign of perceived superiority58,59; Scientific knowledge reserves 60 ; Personal characteristics, including gender, age, educational attainment, and role accumulation61,62; Discrepancies between subjective and objective outcomes, such as forecast errors. 63
However, in the Chinese nonprofit context—particularly in public hospitals—many of these measurement approaches face significant limitations. Personality scales and media sentiment analysis may be subject to stakeholder influence and political sensitivities. Salary-based methods rely on narrow, single-dimensional indicators, and behavioral measures such as investment or financial risk-taking are often inapplicable due to the sector’s non-market nature.
To ensure objectivity and scientific rigor under these constraints, this study adopts the managerial personal characteristics method to assess HDO, following prior research.61,62 This approach is widely accepted in the literature, especially in large-sample studies where direct psychological data is unavailable. Specifically, the following four indicators are used to proxy hospital dean overconfidence, as detailed in Appendix 3: Gender – Male leaders have been consistently found to exhibit greater overconfidence in decision-making contexts 61 ; Age – Older managers are more prone to cognitive rigidity and reliance on experience, which may increase susceptibility to overconfident judgments 64 ; Educational Attainment – Higher levels of education are associated with stronger self-efficacy and perceived competence, leading to inflated confidence in decision-making 58 ; Dual-Role Status – Serving simultaneously as both Party Secretary and Dean signals centralized authority and power, which is positively correlated with overconfidence. 65
This method is particularly suitable for nonprofit settings, such as hospitals, where managerial overconfidence is more likely to manifest through symbolic power and demographic traits rather than through quantifiable financial or strategic behavior. 66 Thus, demographic and positional indicators offer a valid, practical, and theoretically grounded approach to operationalizing HDO in large-scale empirical studies.
Control Variables
We draw upon existing research literature32,57,67-71 and identify average length of stay for discharged patients (In days)(
Model Design
To test research hypotheses H1 and H2, this study constructed the following regression model (1):

In model (1),
Statistical Analysis
Statistical analysis was conducted in several steps. First, descriptive statistics, including the mean, median, and standard deviation, were used to summarize the distributional characteristics of the main variables. 73 Second, Pearson correlation analysis was performed to examine the bivariate relationships among the key variables. 74 To assess potential multicollinearity, variance inflation factor (VIF) tests were conducted for all explanatory variables 75 ; a Pearson correlation coefficient above 0.8 or a VIF value above 10 was considered indicative of possible multicollinearity. 76 Third, the hypotheses were tested using regression analysis. Fixed-effects regression models were estimated to examine the relationship between hospital operational efficiency (HOE) and operational new quality productivity in hospitals (HONQP), while the moderating effect of hospital dean overconfidence (HDO) was tested by including the interaction term (HDO × HOE) in the regression model. Control variables were included in the empirical models to reduce omitted variable bias, and different model specifications with and without controls and fixed effects were compared. Fourth, to assess the robustness of the findings and address potential endogeneity, three additional analyses were conducted: instrumental variable approach through replacement of the dependent variable, subsample regression based on a random 60% subsample, and propensity score matching (PSM).77-80 Finally, heterogeneity analyses were performed by grouping the sample according to hospital institutional type, hospital affiliation, and regional economic development.81-83 Statistical significance was assessed at the 0.10, 0.05, and 0.01 levels.
Results
Descriptive Statistics
Appendix 4 lists the descriptive statistics of the main variables.
73
From the analysis results in Appendix 4, it can be seen that the mean of HONQP is 7.6347, the median is 2.3114, and the SD is 11.9190, indicating that there are significant differences in operational new quality productivity in hospitals among different tertiary public hospitals. The mean of HOE is 6.9175, the median is 7.1200, and the standard deviation is 0.8916, indicating that there is no significant difference in operational efficiency among most tertiary public hospitals, which indirectly explains the phenomenon that hospital operational efficiency is increasingly valued by tertiary public hospitals. The descriptive statistics of the control variables show that the mean, median and SD of Number_OEA are 6.2633, 6.3578 and 0.5198, indicating that there is no significant difference in the Number of emergency department patients per employee (Person-time) among different tertiary public hospitals. The standard deviations of other control variables, such as Average length of stay for discharged patients (In days)(
Correlation Analysis
This study primarily examined the impact of hospital operational efficiency on operational new quality productivity in hospitals. To determine the correlation between hospital operational efficiency and operational new quality productivity in hospitals, as well as potential collinearity between variables, Pearson correlation analysis was performed on key variables. 74 The results are presented in Appendix 5.
The correlation analysis results in Appendix 5 indicate a significant positive correlation between hospital operational efficiency (HOE) and operational new quality productivity in hospitals (HONQP) at the 0.01 level, supporting the expectations of this study and preliminarily verifying Hypothesis H1. To further verify the presence of multicollinearity, the variance inflation factor (VIF) test was conducted on all variables. 75 Multicollinearity is suspected if the Pearson correlation coefficient between variables exceeds 0.8. 76 A VIF value exceeding 10 indicates multicollinearity. 76 The VIF test results showed that all variable values ranged from 1.226 to 4.124, well below the critical value of 10, confirming that the constructed model does not suffer from serious multicollinearity.
Main Regression
Main Regression
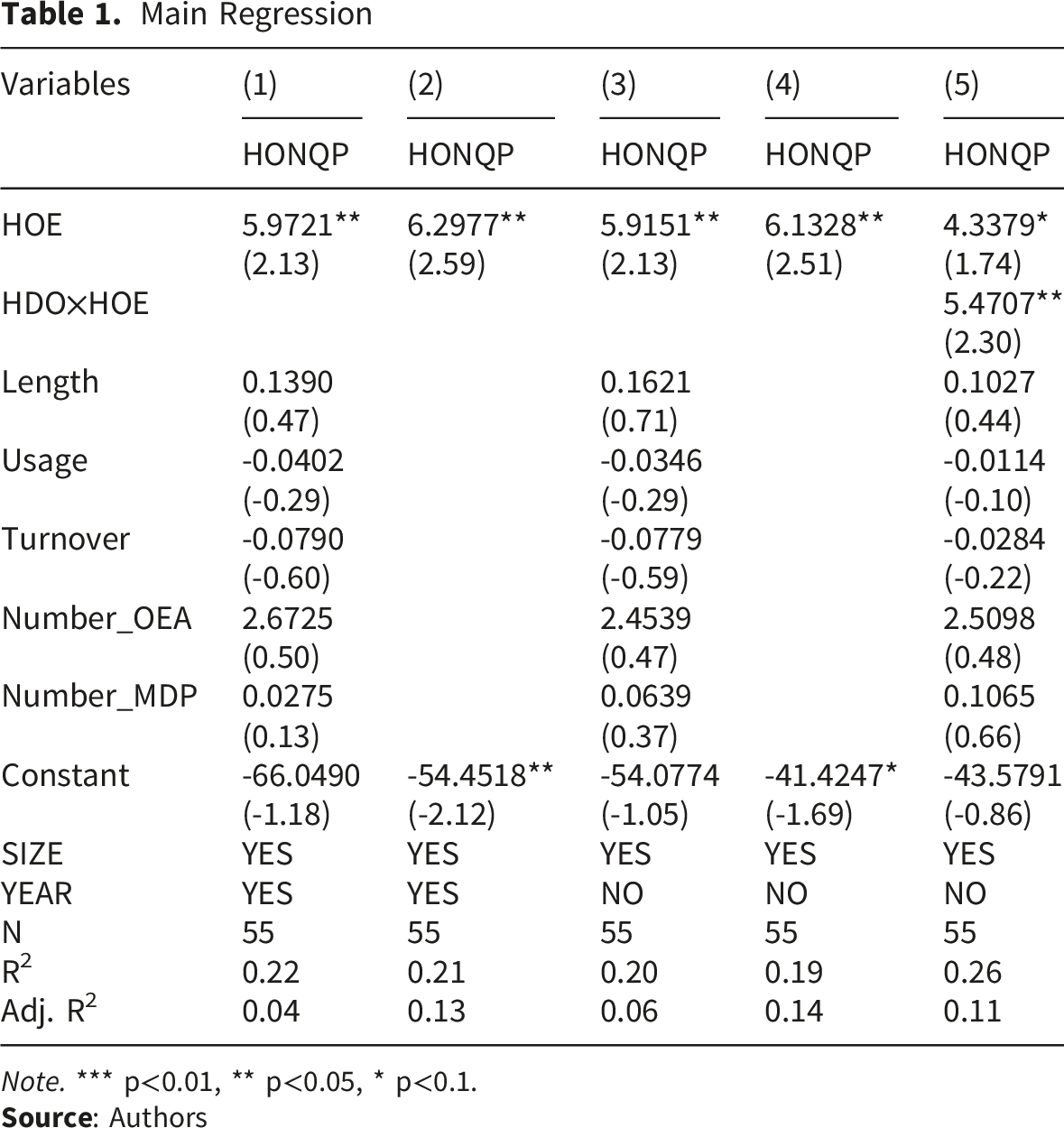
Note. *** p<0.01, ** p<0.05, * p<0.1.
The results in columns (1) to (4) of Table 1 show a significant positive correlation between hospital operational efficiency (HOE) and operational new quality productivity in hospitals (HONQP) at the 0.05 level, confirming that hospital operational efficiency positively impacts operational new quality productivity in hospitals, thus verifying hypothesis H1 of this research. This positive impact is primarily due to city A’s tertiary public hospitals’ emphasis on operational efficiency, achieved through positive measures such as talent acquisition, technological innovation, performance reform, infrastructure enhancement, and others.
The results in column (5) of Table 1 show that after adding the interaction term (HDO×HOE) to the model, the interaction term is significantly positive at the 0.05 level, and the HOE coefficient is significantly positive at the 0.1 level, indicating that hospital dean overconfidence (HDO) positively moderates the relationship between hospital operational efficiency (HOE) and operational new quality productivity in hospitals (HONQP). This confirms hypothesis H2 of this study. This may be explained by the fact that dean overconfidence in city A’s tertiary public hospitals is associated with a stronger strategic orientation toward innovation-driven, technology-enabled, and quality-oriented operational upgrading, thereby reinforcing the positive relationship between HOE and HONQP. This reflects the personal characteristics of hospital leaders in city A and aligns with the personality traits of this city’s residents. At the same time, we need to note that the observed positive moderation by overconfidence should be interpreted cautiously, as it does not discount the substantial contributions of hospital structure, technological infrastructure, external regulation, and team-based culture. Operational efficiency and productivity are emergent outcomes from multifactorial interactions, and the overemphasis on individual-level traits may obscure this complexity.
Robustness Checks
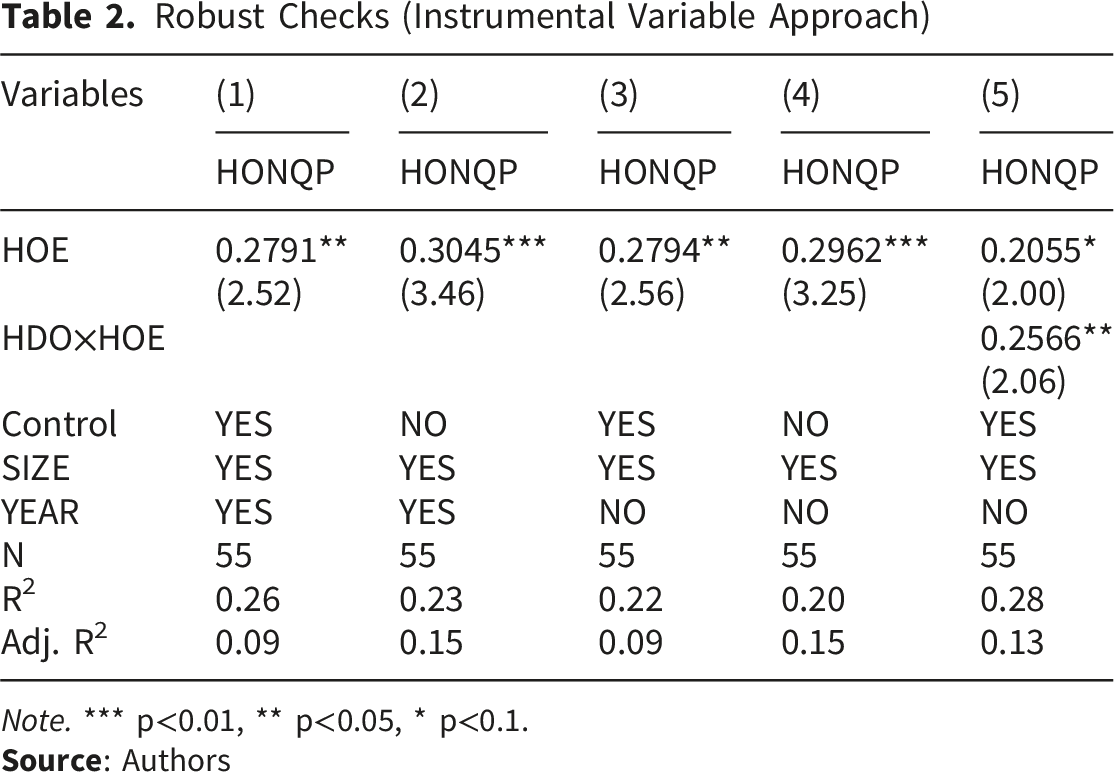
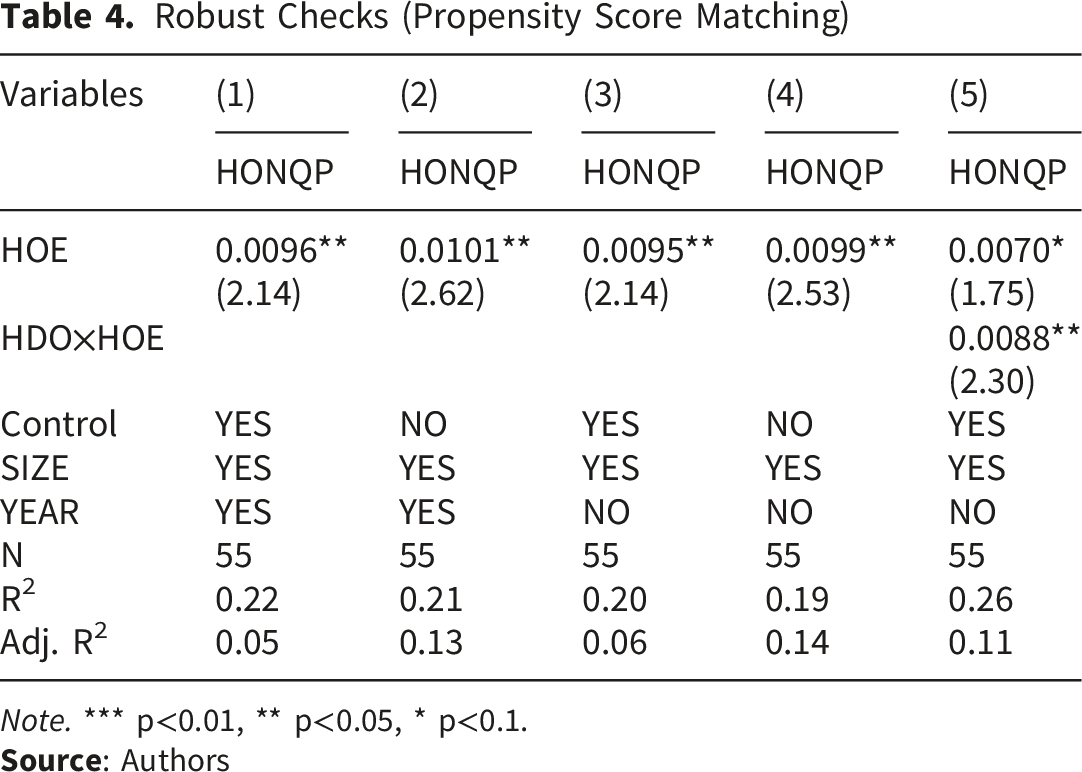
To further enhance the reliability of the results and address potential issues of reverse causality and endogeneity—such as the possibility that more productive hospitals may attract additional resources (reverse causality), or that unobserved variables (e.g., leadership quality, regional policies, and employee morale) may simultaneously influence both operational efficiency and HONQP (omitted variable bias)—we employed three robustness testing methods 77 : the instrumental variable approach (replacing the dependent variable), 78 the sample range method (the random selection of a 60% subsample), 79 and the propensity score matching (PSM). 80
Instrumental Variable Approach
Robust Checks (Instrumental Variable Approach)
Note. *** p<0.01, ** p<0.05, * p<0.1.
Sample Range Method
Robust Checks (Sample Range Method)

Note. *** p<0.01, ** p<0.05, * p<0.1.
Propensity Score Matching
Robust Checks (Propensity Score Matching)
Note. *** p<0.01, ** p<0.05, * p<0.1.
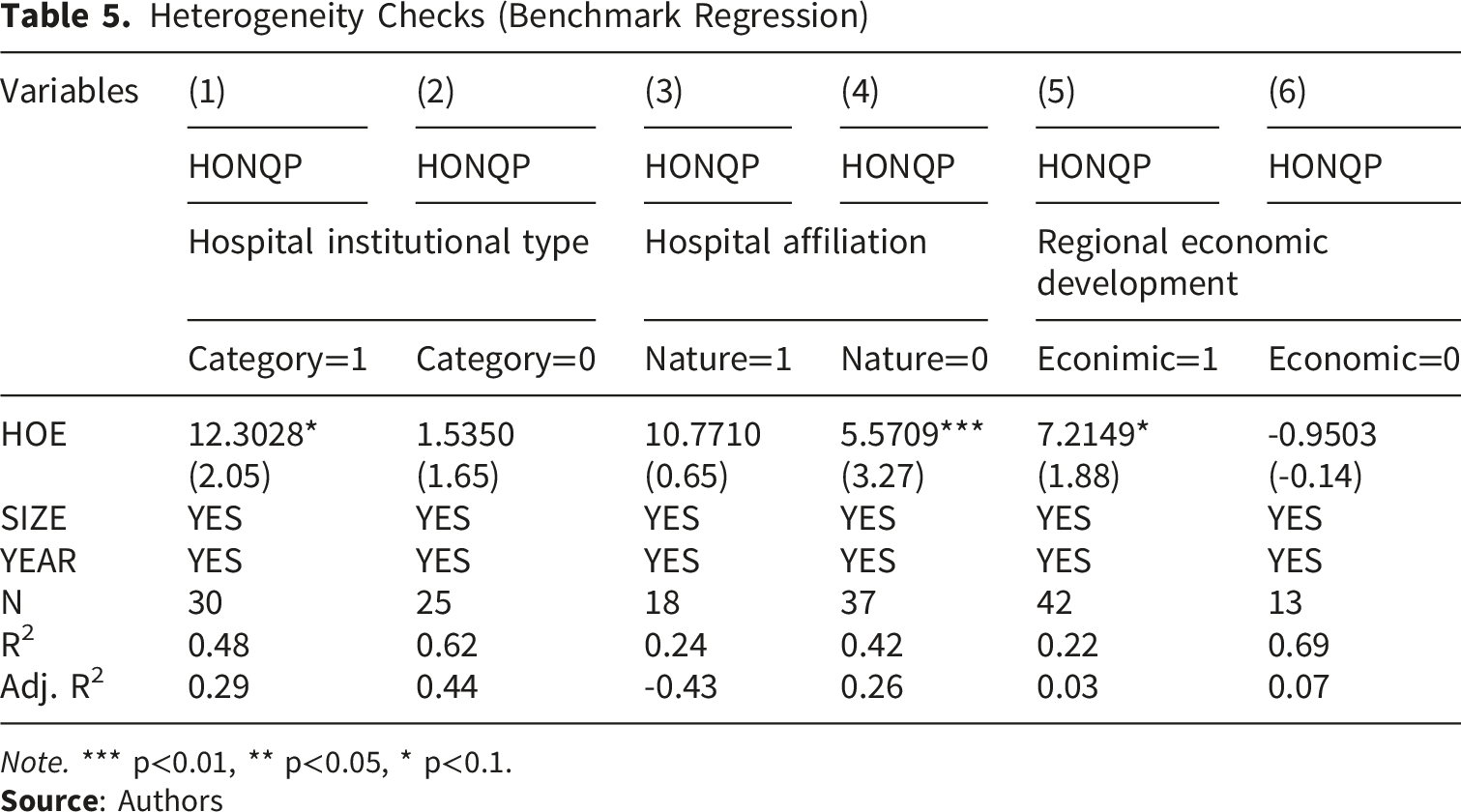
Heterogeneity Checks
Numerous studies have demonstrated that hospital operational efficiency varies depending on factors such as institutional type, affiliation, and regional economic conditions.81-83 Hence, this study employs hospital institutional type, hospital affiliation, and regional economic development as indicators of heterogeneity to examine their impact on hospital operational efficiency and operational new quality productivity in hospitals.
Heterogeneity Checks (Benchmark Regression)
Note. *** p<0.01, ** p<0.05, * p<0.1.
Main Regression
Heterogeneity Checks (Moderating Effect)
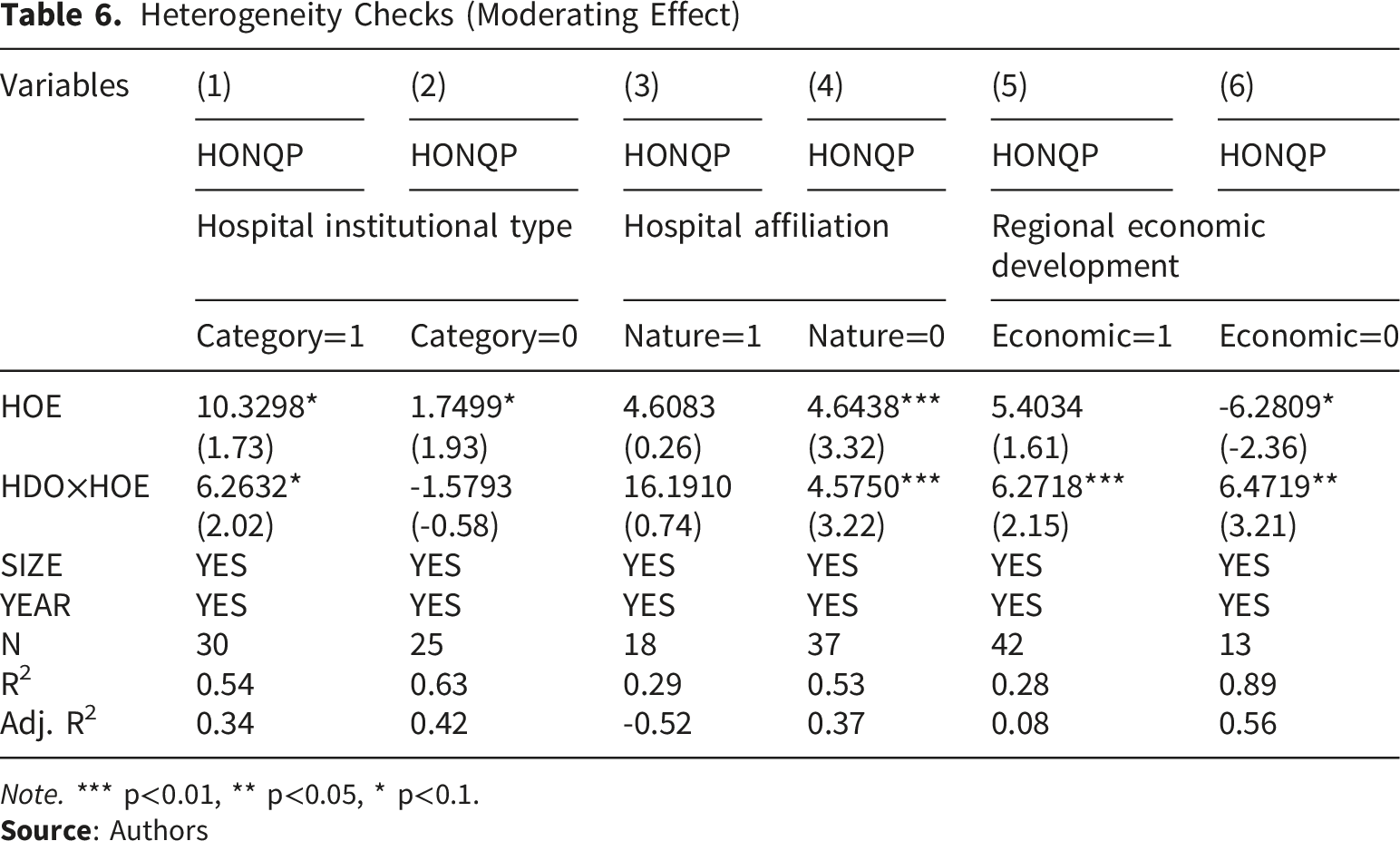
Note. *** p<0.01, ** p<0.05, * p<0.1.
Moderating Effect of HDO
Table 6 demonstrates the results of the heterogeneity analysis of hospital operational efficiency and operational new quality productivity in hospitals, incorporating the moderating variable of hospital dean overconfidence. The regression results in columns (1) to (6) of Table 5 indicate that, under the moderating effect of hospital dean overconfidence, hospital operational efficiency significantly enhances operational new quality productivity in general hospitals compared to specialized hospitals and traditional Chinese medicine hospitals. Similarly, in district hospitals compared to municipal hospitals, hospital operational efficiency significantly promotes operational new quality productivity in hospitals. Moreover, in regions with better economic development, hospital operational efficiency shows a stronger positive correlation with operational new quality productivity in hospitals than in regions with poorer economic development levels.
Discussion
Based on the theoretical frameworks of Marx’s productivity theory, upper echelons theory, and hospital governance theory, combining the concepts from the international literature on total factor productivity, green productivity, and smart healthcare transformation, this study developed a theoretical model of hospital operational efficiency and operational new quality productivity in hospitals. Using the economic indicator database of tertiary public hospitals from 2022 to 2025 and the personal characteristics database of hospital deans obtained by web crawler technology, we constructed a research sample to examine the relationship between hospital operational efficiency and operational new quality productivity in city A’s tertiary public hospitals in China.
To begin with, the empirical findings show that hospital operational efficiency (HOE) is positively related to operational new quality productivity in hospitals (HONQP). Additionally, hospital dean overconfidence (HDO) positively moderates the relationship between HOE and HONQP. These results align with the findings of hospital governance theory,23,27,31 Marx’s productivity theory, 32 and upper echelons theory.33,34,37
This indicates that, under the moderating effect of managerial overconfidence, the relationship between operational efficiency and operational new quality productivity in city A’s tertiary public hospitals is consistent with the conclusions drawn from enterprise research.84-87 This suggests a degree of commonality between corporate governance and hospital management, allowing for mutual learning from their respective research results. Furthermore, the findings corroborate previous scholars’ conclusions, emphasizing that hospital deans, as the highest managers and decision-makers of hospital operations, are crucial factors influencing hospital management.35,88,89
Secondly, the heterogeneity analysis revealed that the impact of hospital operational efficiency on new quality productivity varied by hospital institutional type, hospital affiliation, and regional economic developments. Specifically, heterogeneity was observed across all these factors, with hospital affiliation showing the most significant variation. When incorporating the moderating effect of hospital dean overconfidence, the differences in heterogeneity remained, with hospital affiliation continuing to exhibit the most pronounced effects. This study is the first to employ heterogeneity analysis to examine the relationship between hospital operational efficiency and operational new quality productivity in hospitals.
Building upon these findings, our research has practical and managerial significance.. The findings inform medical policymakers, hospital managers, and practitioners of the need to prioritize talent capital, enhance technological innovation, continuously optimize operational processes, and leverage big data and artificial intelligence to build new quality productivity for hospital development. These steps will improve hospital management and promote high-quality development. Hospital practitioners must recognize the importance of operational efficiency in fostering operational new quality productivity in hospitals, strengthen their clinical and managerial skills through continuous learning, and contribute effectively to their roles. Hospital managers should cultivate a people-oriented culture, and create a supportive work environment through psychological counseling, performance reform, skills training, and job promotions to motivate employees and develop intellectual capital. By focusing on productivity elements such as laborers, labor tools, and labor objects, managers can establish a new quality productivity system to sustain hospital development. Medical policymakers should consider hospital operational efficiency’s role in enhancing operational new quality productivity in hospitals from the perspective of spatial health resource allocation. They should conduct in-depth research, formulate health policies based on actual conditions, and promote the scientific development of medical resources regionally. Furthermore, when selecting public hospital deans, overconfidence as a personality trait should be considered to harness its positive moderating effect on the relationship between hospital operational efficiency and operational new quality productivity in hospitals. It is particularly important to recognize that while moderate managerial overconfidence can enhance decision-making effectiveness and organizational resilience, excessive overconfidence may lead to resource misallocation, diminished collaboration, and ethical blind spots. Hospital administrators should strive to balance individual psychological traits with institutional checks and collaborative governance structures. Moreover, performance-driven reforms influenced by managerial behavioral traits must be implemented with careful consideration of their ethical implications, especially within public healthcare institutions. Policy frameworks should include safeguards to prevent the emergence of misaligned incentives or inequities in resource allocation.
Furthermore, in light of these research findings, our study also offers several significant contributions to the literature. First, it develops a more comprehensive theoretical understanding of the relationship between hospital operational efficiency (HOE) and operational new quality productivity in hospitals (HONQP), thereby extending existing research on hospital governance and hospital productivity transformation. Compared with existing productivity measures in the healthcare literature, such as TFP, DEA efficiency, and Lean metrics, HONQP distinguishes itself by emphasizing innovation-driven, technology-enabled, and quality-oriented operational upgrading, dimensions that are often underrepresented in conventional measures. In this sense, the study not only provides a contextually relevant conceptualization of hospital productivity transformation, but also broadens the theoretical basis for explaining how operational efficiency contributes to hospital modernization. Second, the study enriches the application of upper echelons theory and Marx’s productivity theory in the hospital context by showing that hospital operational upgrading is shaped not only by structural and resource conditions, but also by managerial cognition and behavioral traits. In doing so, it strengthens the interdisciplinary connection among hospital management, psychology, and behavioral economics, and contributes to a more behaviorally informed understanding of hospital governance. Third, by introducing hospital dean overconfidence (HDO) as a moderating variable, this study further explains how managerial characteristics influence the relationship between HOE and HONQP, thereby advancing hospital governance theory at a deeper level. At the same time, it is important to note that overconfidence may not always produce beneficial outcomes. In some cases, it may lead to overestimation, strategic miscalculations, or inadequate risk assessment. Accordingly, the present findings suggest that managerial cognition should be understood as a contingent factor in hospital operational upgrading rather than as a uniformly positive force. Future studies should explore the non-linear or conditional effects of overconfidence in greater depth. Fourth, by analyzing heterogeneity across hospital institutional type, affiliation, and regional economic development, this study provides more fine-grained evidence on how the relationship between HOE and HONQP varies across institutional settings. This not only supplements the main findings with contextually grounded insights from a single-city sample, but also highlights the importance of institutional environment in shaping hospital operational transformation. As such, the study offers exploratory evidence that may inform future comparative research across regions, ownership structures, and healthcare systems.
Finally, we must acknowledge the limitations of this study and suggest directions for future research. First of all, our operational new quality productivity in hospitals (HONQP) scale considered only a few key factors. According to Marx’s productivity theory and the concept of new quality productivity, numerous factors contribute to HONQP. This study did not account for all of these factors, which should be further examined in future research to enhance the reliability of our conclusions. Second, we acknowledge that this study focuses exclusively on hospital dean overconfidence (HDO) as a psychological trait, while omitting other relevant managerial characteristics such as risk tolerance, narcissism, and decision-making style. This narrow focus may limit the explanatory power of the findings and introduce omitted variable bias. Moreover, although this study examines the moderating effect of HDO on the relationship between hospital operational efficiency (HOE) and HONQP, other managerial behavioral traits—such as narcissism, hubris, and risk propensity—may also exert significant moderating effects. Future research should incorporate a broader set of psychological constructs and explore their potential roles in hospital performance models to improve both theoretical depth and empirical robustness. Third, although the model includes control variables such as Length, Usage, Turnover, Number_OEA, Number_MDP, SIZE, and YEAR, it omits several critical contextual determinants of hospital productivity—such as personnel skill levels, equipment adequacy, funding streams, and patient complexity. The exclusion of these confounding factors may bias the estimated effects of managerial traits. Future research should adopt a more comprehensive control strategy or employ additional instrumental variables to address endogeneity concerns. Fourth, the current study employs demographic proxies (e.g., age, gender, and dual-role status) to measure overconfidence. While practical, these proxies may not fully capture the cognitive-emotional dimensions of HDO. Future studies should consider using validated psychometric scales or behavioral assessment methods to enhance construct validity. Fifth, the study is based on 55 tertiary public hospitals from a single-city setting. Although this sample represents the full set of eligible tertiary public hospitals within the study context, the institutionally bounded sample size may still limit the broader generalizability of the findings. In addition, no formal a priori sample size or statistical power analysis was conducted, as the study adopted a context-specific full-sample design rather than a sample-based design. Future research should test the proposed relationships using larger and more diverse multi-city or multi-region samples to further assess the robustness and external validity of the findings. Sixth, this study is limited to City A, China, which may affect the generalizability of the findings beyond the local institutional and policy environment. Future research should incorporate data from public hospitals across other provinces and cities in China to improve external validity. Additionally, this study focuses solely on public hospitals, excluding private institutions. Whether similar relationships exist in China’s private hospital sector remains unclear. Future research should examine private hospitals to extend theoretical insights and inform the high-quality development of the broader healthcare system. Finally, due to the unique characteristics of China’s healthcare governance and data limitations, public hospitals in other countries were not included in this analysis. Further research is needed to determine whether the study’s findings are applicable in international contexts. Cross-national comparisons and collaborative research are encouraged to advance global healthcare management theory.
Conclusion
This study investigates the relationship between hospital operational efficiency (HOE) and operational new quality productivity (HONQP) in the context of Chinese public healthcare reform, incorporating hospital dean overconfidence (HDO) as a moderating variable. Drawing from Marxist productivity theory, upper echelons theory, and hospital governance theory, we conceptualize HONQP as a transformation-oriented productivity framework that integrates talent capital, technological innovation, and expanded operational scope within hospitals. Using data from 55 tertiary public hospitals in City A, China, from 2022 to 2025, we empirically demonstrate that HOE significantly enhances HONQP. Furthermore, we find that HDO positively moderates this relationship, reinforcing the idea that managerial cognitive traits influence organizational outcomes. These findings are robust across multiple empirical strategies, including instrumental variable analysis, propensity score matching, and subsample testing, and hold true across different hospital types, affiliations, and regional economic contexts. The study makes several key contributions. Theoretically, it introduces a context-specific productivity framework tailored to healthcare, advancing both Marxist and behavioral productivity models in hospital settings. It also extends upper echelons theory by highlighting the nuanced role of overconfidence in complex institutional environments like public hospitals. Practically, the findings provide actionable insights for policymakers and hospital administrators, emphasizing the need to improve operational efficiency, recognize behavioral traits in leadership selection, and design systems that balance innovation with ethical safeguards. Nonetheless, limitations persist, including reliance on proxy measures for overconfidence, exclusion of critical contextual factors, and limited geographic generalizability. Future research should incorporate longitudinal, multisite, and international data, while also employing validated psychometric tools to refine behavioral variable measurement.
Supplemental Material
Supplemental Material - Nexus Between Operational Efficiency and New Quality Productivity in Hospitals: Does Dean Overconfidence Matter
Supplemental Material for Nexus Between Operational Efficiency and New Quality Productivity in Hospitals: Does Dean Overconfidence Matter? by Jackie Zhanbiao Li, Yingqian Lao, Xin Li, Qianhui Ting, Qiwen Jiang in Inquiry: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgements
We would like to express our sincere gratitude to all members of our research team for their hard work and dedication.
Ethical Considerations
The data used in this study are secondary data, all of which are sourced from publicly available and legally authorized databases, with no direct or indirect human involvement. The data collection process adhered to relevant legal regulations to ensure the protection of individual privacy and other legal rights. Therefore, ethical approval from an ethics committee is not required for this study.
Author Contributions
Jackie Zhanbiao Li analyzed data and drafted the manuscript.
Qianhui Ting and Xin Li designed the study and performed the data collection.Yingqian Lao and Qiwen Jiang made substantive intellectual contributions to the conception of the work and the interpretation of the data and revised the manuscript.
These authors contributed equally to this work.
Funding
This study represents a phased research achievement of the project “Design and Practical Research on Hospital Internal Performance Products under DRG,” funded by the 2022 Guilin Science and Technology Plan of the Guilin Science and Technology Bureau, Contract No. 20220139-8. Yingqian Lao was associated with this research project.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data will be made available upon request by contacting the primary corresponding author.
Declaration of AI Use
The authors declare that Artificial Intelligence (AI) tools were used solely for language refinement and editing to improve the clarity, readability, and overall presentation of the manuscript. No AI tools were used in the design of the study, data collection, data analysis, or interpretation of results. The authors further confirm that no scientific data, results, or conclusions reported in this study were generated or modified using AI. All content remains the original intellectual work of the authors, who take full responsibility for the accuracy, originality, and integrity of the manuscript.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.