
Abstract
Introduction
Medication administration in pediatric and neonatal care is complex and high-risk due to weight-based dosing and rapid physiological changes. Health information technology (HIT) offers promising solutions to enhance safety through tools like dose calculators and clinical decision-support systems. This study explored nurses’ experiences with the medication administration process (MAP) to identify HIT-driven solutions for safer practices.
Methods
As part of a larger project to develop a knowledge-based decision support system, a conventional qualitative content analysis was conducted. Data from interviews and observations of 19 nurses across seven hospital units were analyzed inductively using the Lundman and Graneheim method and validated by expert review.
Results
Analysis identified one main category and four subcategories. Nurses emphasized the complexity of dose calculations, the high risk of medication errors, and a pressing need for structured change. Findings highlighted that technological interventions are crucial to improve workflow efficiency, enhance accuracy, and reduce errors. Integrating digital tools was found to foster better peer collaboration, improve care quality, decrease burnout, and create a safer, more efficient medication process.
Conclusion
Key recommendations emphasized implementing advanced decision support systems for dose calculation and error alerts, integrating intelligent EHR features such as automated double-checks, and adopting a user-centered design approach in developing these digital tools.
Keywords
1. Introduction
The medication management process (MAP) includes the steps of prescribing, transcribing, dispensing, administering, and monitoring. 1 Medication administration (MA), the final step of this process, directly involves nurses and patients in our study setting; however, in other care models, medication administration may also involve other clinicians depending on the location and available resources. 2 In a healthcare environment, MA is a high-risk task for nurses, as they are the final check before a medication is administered.2,3 Effective drug therapy relies on correctly executing all steps related to medication management. Significant challenges include weight-based dosing, rapid growth in weight and height of children and neonates, and the lack of standard pediatric formulations. 4 These challenges are more pronounced in critical care units for neonates and children,5,6 such as neonatal intensive care units (NICUs), where the severity of patients’ medical conditions and the diversity of drugs increase the risk of errors.7-10
In the digital age, information technology (IT) has become integral to nursing practice, with nurses bearing a great responsibility to utilize IT applications.11-13
Identifying users’ needs is the first crucial step before implementing IT in any organization. 14 IT can help solve challenges in pediatric and neonatal medication administration, such as weight-based dosing, rapid growth, and drug errors, by providing precise dose calculation tools and decision support systems that flag potential errors.15,16 However, the effectiveness of such technologies depends on organizational readiness, workflow integration, staffing levels, and nurses’ cognitive workload. Without alignment with clinical context, technology may introduce new challenges rather than resolve existing ones.
Technology adoption in healthcare is therefore a socio-technical process shaped by interactions between human factors, organizational culture, and technical infrastructure. A user-centered approach, as an initial step in developing health-related IT interventions, can enhance meaningful adoption and sustainability. 17
Qualitative methods are particularly useful for assessing information needs, exploring nurses’ experiences, and understanding attitudes toward MAP. 18 While quantitative studies can address many health-related questions, qualitative research is indispensable for examining context-dependent processes and capturing insight into lived professional experiences. 19 Given that MAP structures vary across countries and healthcare systems, assessing the local environment and user needs is essential before technological implementation. Therefore, this study aims to explore nurses’ experiences and attitudes toward MAP in pediatric and neonatal settings, with attention to contextual factors and opportunities for appropriate technological support. The study employed a qualitative approach complemented by observational methods.
2. Methods and Materials
The present study was registered at the Kerman University of Medical Sciences (#403000345). This study adhered to the Consolidated Criteria for Reporting Qualitative Studies (COREQ) 20 (see the Supplemental File, COREQ Statement Checklist).
2.1. Study Design
The present study is part of a larger research project that conducted interviews and participant observation to design a knowledge-based decision support system for the MA in pediatrics and neonates. Conventional qualitative content analysis was used to obtain specific information about the attitudes and behavior of nurses in the MAP, which allowed us to obtain rich and complex relevant information. 21
2.2. Study Setting
The study was conducted across seven pediatric and neonatal units in a referral and educational hospital affiliated with Kerman University of Medical Sciences. Kerman. Kerman, the largest city in southeastern Iran, serves as a daily hub for visitors from a 500-kilometer radius. This hospital operates seven active units dedicated to children and neonates, including two general pediatric units, two NICU units, a pediatric intensive care unit (PICU), a pediatric chemotherapy unit, and a pediatric emergency unit. Advanced surgical and medical interventions are performed daily on children and neonates in this hospital. This hospital has been a pioneer in using information technology (IT) in Iran, leveraging it for over 20 years. IT is employed to automate various hospital processes, such as clinical documentation, cost and resource management, medication management (MM), and performance evaluation of nurses and physicians.
The medication management process in this hospital is as follows: During the morning shift, physicians prescribe the required medications for the next 24 hours. Additional medicines may be prescribed during the day in emergencies. The head nurse records the prescribed medicines in a medicine cardex and enters the orders into the medication management module within the hospital information system (HIS). The pharmacy manager delivers the medications to the respective unit, placing them on medicine shelves or in designated rooms. Before storage, medications are labeled in red and yellow to indicate high-alert and look-alike drugs. Nurses retrieve each patient’s medication from the designated shelves or rooms using a drug card specific to the patient. The drug card colors differ in the morning, evening, and night shifts.
2.3. Sample Size and Eligibility Criteria
A total of 19 nurses with different professional specialties were selected using purposive sampling. Nurses who participated in the daily MAP were invited for an interview. Snowball sampling was also used by asking the participants to introduce other colleagues to participate in the study. The sampling process was based on maximum variation to obtain rich and diverse views and experiences from the participants. A diverse group of nurses, including those of different sexes, ages, work experience, education level, positions, and clinical wards, were included in the study. The interviewees had extensive experience in pediatrics and neonatal settings and were familiar with using IT systems such as health information systems (HIS). Additionally, many of them had worked with paper-based systems for several years. Ultimately, interviews were conducted with 19 nurses, and no participants declined to participate. The nurses worked in one pediatric unit (NICU, PICU, pediatric oncology, pediatric emergency, and general pediatric) during the morning, evening, and night shifts. The interviews continued until data saturation.
2.4. Data Collection (Interview Guide and Participant Observation)
In-depth, semi-structured face-to-face interviews were held in a comfortable and quiet room in the target units, from February to April 2021. All interviews were conducted by the first researcher (SN), who was a Ph.D. student of medical informatics and familiar with qualitative studies. To minimize potential power dynamics, the researcher clarified her role as a Ph.D. student and the study purpose, assured participants of confidentiality, and emphasized voluntary participation. Rapport-building and neutral questioning were employed to encourage open and honest responses.
Interview Questions
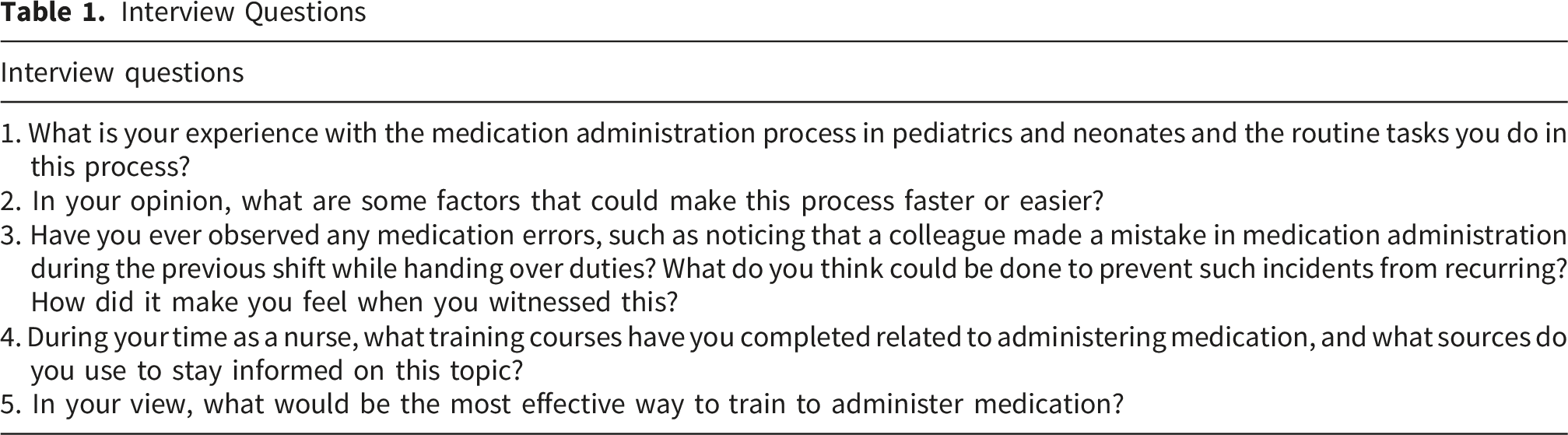
Each interview, lasting between 15 minutes and one hour, was audio-recorded, with additional notes taken during the interview. To gain a deeper understanding of the MAP, observational data were collected along with the interviews. Participants were observed across seven units—NICU, PICU, pediatric chemotherapy, pediatric emergency, and general pediatric—for three weeks between February and April 2021. Observations were conducted during morning, evening, and night shifts, with approximately 4–6 hours of observation per unit per shift, resulting in an average of 45–60 minutes of direct observation per nurse during medication preparation and administration episodes. The observation was semi-structured: it was guided by predefined domains—including medication preparation, administration workflow, communication patterns, environmental factors, and interruptions—while allowing flexibility to capture emergent contextual issues. A detailed observation protocol (see Supplemental A) was followed to ensure consistency and non-interference, and the observer (SN) closely examined nurses’ activities during medication preparation and administration without interrupting their work.
Informal interviews were conducted with the nurses during the medication administration process whenever time allowed. The observations also included examining medicine storage rooms and shelves, a review of emergency trolley contents and drug labels, as well as an assessment of devices, such as peripherally inserted central catheters (PICC), utilized in medication administration.
2.5. Data Analysis
A conventional content analysis was conducted following Graneheim and Lundman. 22 To get to know the data, the first author listened to all interviews multiple times, after which they were transcribed verbatim. To gain an in-depth understanding, semantic units were identified, preliminary codes generated, and the data interpreted. The transcripts were independently read and reread by SN and MN. Using an inductive approach, codes were developed from participants’ statements, descriptions, and observations. Codes with similar content were grouped into sub-subthemes, which were subsequently organized into subthemes. Finally, main themes were derived by comparing the similarity of subthemes. A back-and-forth iterative approach was applied throughout to ensure high internal consistency and minimize external inconsistency.
To minimize potential researcher bias and address power dynamics, coding and interpretation were conducted independently by multiple team members (SN, MN), with disagreements resolved through discussion and consensus (SN, MN, JA, ZS). An external qualitative research expert (LA) reviewed and approved the coding process and thematic categories. Member checks, triangulation of interview and observational data, and peer debriefings further ensured that findings accurately reflected participants’ perspectives and reinforced reflexivity throughout the analysis process. Observational data was carefully compared and integrated with interview data to provide contextual insights into nurses’ workflows and challenges in medication administration. MAXQDA2018 was used to facilitate data organization, coding, and analysis.
2.6. The Rigor of the Study
To ensure the study’s quality, Lincoln and Guba’s criteria (credibility, dependability, confirmability, transferability, and authenticity) were meticulously applied.23-25 To enhance credibility, the researcher (SN) was continuously engaged with the participants and the research environment over an extended period. Member checks were performed after each interview, during which the researcher summarized and shared the overarching interpretations of participants’ descriptions to ensure accuracy. Data collection was enhanced through methodological triangulation, which systematically integrated multiple approaches (interviews and direct observations) to ensure robustness and validity.
Peer debriefings were also conducted during which research team members systematically discussed and validated emerging themes, reinforcing the methodological rigor and credibility of the findings.
To ensure dependability, interviews were independently coded by research team members (SN, MN, JA, ZS). The coding and analysis process underwent external review and formal approval by a medical informatics expert (LA) proficient in qualitative research. Discrepancies were resolved through team discussions, with results determined by collective consensus among all research members.
Confirmability was ensured through systematic documentation of all aspects of the research process, including comprehensive records of data collection methods and analysis procedures. Research materials—such as notes, transcripts, and audio recordings—were securely archived for long-term accessibility. Additionally, maximum variation sampling was employed to capture a diverse range of participant perspectives and experiences.
Transferability was established by thoroughly documenting participant characteristics, recruitment methods, and research phases. The reasoning behind methodological choices was justified, ensuring transparency.
Finally, authenticity was ensured by transparently representing the diverse realities encountered in the MAP. Direct participant quotes were integrated into the results to substantiate themes, ensuring the findings remained firmly grounded in participants’ authentic voices.
3. Results
The Baseline Characteristics of Participants

Summary of Thematic Analysis Results


An overview of the identified key aspects of the main theme and their sub-themes
3.1. Main Theme: The Need to Use Technology in MAP
3.1.1. Sub-theme 1: The Complexity of MAP in Pediatrics and Neonatal Patients
This subtheme highlights the complexity of MAP in children and neonates. Interviewees consistently emphasized that this process is significantly more intricate than in adults due to weight- and height-based dosage calculations and the absence of pediatric-specific formulations. The need for repeated calculations further complicates medication administration, particularly when determining accurate dosages for dilution. These challenges reflect broader issues in pediatric medication preparation, where multiple dilution steps and the lack of standardized formulations create a demanding process that requires continuous verification to ensure precision and patient safety. For novices, preparing medicines for children and neonates involves precise calculations of multiple ratios and dilutions, which can be particularly difficult and confusing. The inherent complexities of pediatric and neonatal care, including variations in patient age, weight, and medication administration protocols, demand exceptional precision and vigilance, further compounding the difficulties clinicians face in these settings. For example, “I have to make several calculations again and again. I want to make sure whether I calculate things correctly or not. Overall, the dose of medications that need to be diluted is hard to estimate.” (Participant #1)
“In general, it is difficult to prepare medicines for children, especially for novices, e.g., the preparation of a serum and the right number of solutions that should be diluted in it. First, we have to adjust the ratio. These estimations are hard and confusing.” (Participant #5)
3.1.2. Sub-theme 2: The Probability of Making Medical Errors in Specific Conditions
As described by the interviewees, specific conditions in pediatric and neonatal units significantly increase the probability of medical errors, such as overdose and underdose errors. Factors such as high patient loads, the critical nature of patients’ health conditions, the absence of electronic prescription systems contribute to these errors. Similarities in medication names and appearances pose additional risks. Most drugs look alike, and some even have identical names, increasing the possibility of errors. The interviewees emphasized the role of individual and systemic factors in these errors. Fatigue among nursing staff was identified as a frequent contributor, leading to nursing errors and diminished attention to detail. In addition, transcription errors and the absence of sufficient double-check mechanisms amplify the risk of inaccuracies in medication administration. Missed nursing care, resulting from both workload pressures and carelessness, further aggravates the situation, with interviewees reporting cases where vital medications were either improperly dosed or missed entirely. Participants also noted that closer collaboration with the pharmacy department could help prevent many of these errors before they reach the bedside.
For example, “To calculate the dose of medicine, we only need to increase our accuracy. Yet the error occurs and seems inevitable. For example, today, a nurse was tired because there were eight patients, instead of three.”. (Participant # 9)
“After you work for a while, you make fewer mistakes. You are more concentrated on your work but may still make a mistake. I may have some patients in critical condition. In this case, the workload increases, so I have to speed up my work, which can lead to more errors”. (Participant # 7, observation)
“I had the experience of administering amikacin instead of clindamycin to the patient by mistake. These two drugs look alike. From then on, even when I am pretty sure this drug is the right one, I still check the shape and name of the medication carefully. This medication check is very important to decrease errors. Another reason for the imprecision in administering the medications is the high workload of staff. (Participant #3, observation)
3.1.3. Subtheme 3: The Need to Pave the Way for Change
This sub-theme highlights the critical importance of laying the groundwork and fostering an environment that enables and supports transformative changes to the MAP. Participants consistently highlighted that leveraging technology could be a key driver for facilitating these modifications. Implementing such changes requires a two-fold approach: first, restructuring the organization to ensure systems and processes with new technological advancements; second, fostering a cultural shift to adapt individuals’ attitudes toward embracing innovation. The healthcare sector has encountered numerous opportunities to integrate technology into care delivery, indicating that a transition from traditional approaches to modern, technology-driven processes could streamline nursing tasks and reduce procedural complexities. Furthermore, nurses with limited experience in pediatric and neonatal settings exhibited a strong tendency toward adopting technological solutions, indicating that professional exposure may influence attitudes toward the modernization of nursing practices.
For example, “During the COVID-19 pandemic, the training was all virtual, which managed to prepare the healthcare staff for technology use”. (participant #15)
‘The adoption of technology in medication administration is essential for advancing nursing practices. Nurse managers should lead by example, transitioning from traditional methods to modern techniques to foster acceptance among the staff and optimize care delivery.” (participant # 7)
3.1.4. Subtheme 4: Technology to Improve the Quality of Nursing Care
As interviewees highlighted, health information technology plays a crucial role in mitigating job burnout, improving work motivation, and optimizing time management by streamlining nursing workflows. Consequently, the quality of nursing care improves. A commitment to advancing nursing care through technology ensures nurses stay empowered, updated, and equipped with evidence-based resources. Implementing innovative tools that facilitate the MAP guarantees patient safety by increasing accuracy in dosage calculations. Furthermore, integrating digital solutions like e-learning platforms and family-engagement applications enhances both professional knowledge and collaborative care, while also reducing nursing workload pressures and preventing burnout. For example, “Usually, the drug calculations are not completely performed by nurses in NICU. Sometimes they help the physician in the process. If an accurate device is available, it can help too. For example, an advanced and practical application can better prevent errors. Because for example, sometimes a lot of antibiotics are injected into an underweight baby. (Participant # 5)
“Using electronic systems and learning to work with them can increase the self-confidence and mastery of nurses over the care process. It can prevent burnout and assist nurses to focus on daily tasks and duties” (Participant # 1).
Participant number 8 stated: “If some of the currently available budgets are allocated to software designers. E.g., Pharmaceutical mobile applications can be developed to be truly effective. Colleagues can then use these applications effectively rather than the unreliable sources on Google or else”. (Participant #8).
3.1.5. Sub-subtheme 4-1: Technology as a Peer Control
Most participants emphasized the importance of verifying drug dosing, administration routes, and other critical aspects more than once. In the MAP, nurses often rely on peer reviews to minimize errors. Meanwhile, technology can serve as an additional safeguard, providing a double-check mechanism for both physicians and nurses. According to reports, medication management in pediatrics and neonates requires close cooperation and communication among physicians, nurses, and clinical pharmacists to ensure accuracy and patient safety.
For example, “Sometimes the calculated dose was wrong because there were many multiplications and divisions. The nurse colleagues could ask us whether we calculated the dose accurately or not. After a second thought, I could realize to make a mistake” (Participant # 10).
“Errors are often in mill equivalents and cubic centimeters (CC). Interns frequently make such mistakes, but experienced nurses can detect them because they understand that the prescribed dose may not be appropriate for a neonate or pediatric patient” (Participant # 1).
4. Discussion
The present study examined nurses’ experiences and attitudes toward MAP in pediatrics and neonates, with a focus on identifying opportunities for technological solutions. The data analysis was categorized into a main theme, “The need to use technology in MAP,” along with four sub-themes.
One subtheme of this study was “The probability of medical errors under specific conditions.” The American Institute of Medicine has reported that human errors are the most common cause of patient safety incidents. 26 The report attributes medication errors to systemic deficiencies in healthcare infrastructure rather than individual human errors. These findings indicate that nurses responsible for MAP may make errors, regardless of their level of expertise. Similar to the American Institute of Medicine report, participants in this study highlighted that medication errors were due to deficiencies in the healthcare system, challenges in the work environment, context-specific conditions, and the role of pharmacy in ensuring safe medication practices. Previous research has demonstrated that these errors can be mitigated through technological interventions such as CDSS.16,27,28
In this study, the most commonly reported medication errors in pediatric and neonatal MAP were overdose and underdose errors. A systematic review on the prevalence of dose errors among pediatric patients supports this finding, showing that six out of twelve studies on medication administration errors (MAE) reported deviations from prescribed dosages. 29
Furthermore, look-alike/sound-alike (LASA) drug errors were identified as another common source of mistakes in these units. However, Ciociano et al conducted a systematic review emphasizing the challenges associated with detecting LASA errors. They noted that reporting issues arise from several barriers, including poor error reporting, inconsistent definitions, time constraints, fear of litigation, difficulty in determining causality, reluctance to admit mistakes, and concerns about costs. 30
Unlike prior studies relying on self-report surveys, this study employed qualitative methods, including interviews and direct observation, allowing for deeper insights into LASA drug errors. One significant advantage of qualitative methods is that they promote closer engagement with participants, which helps identify medication errors that are often underreported. Among the strategies to mitigate LASA errors, clinical decision support systems (CDSS) have been shown to be effective. For instance, a group of researchers in Switzerland developed an application31-34 with alarm functionality for LASA drugs in pediatric emergency units, highlighting its potential to prevent medication errors.
Another critical medication error identified in this study was “Missed nursing care” in MAP. Participants described significant workload pressures, particularly due to limited nurse staffing in pediatric and neonatal units despite high patient volumes. Moreover, many patients were in critical condition, further exacerbating missed nursing care. To address this issue, technology such as electronic nursing reminders can play a valuable role in improving care quality. Schubert et al conducted a review on interventions developed to prevent missed nursing care (MNC) in health institutions. Their findings indicated that IT-based strategies—especially electronic nursing reminders—are effective in reducing missed nursing care when integrated with electronic health records (EHRs). 35
Another sub-theme extracted in this study was “the need to pave the way for change”. Due to the significant impact of the COVID-19 pandemic, online training platforms have become widely used, making the integration of IT tools in MAP more feasible than ever before. As a result, nurses have become more accustomed to online training, and this shift provides an opportunity to incorporate technology-driven solutions into MAP practices. A body of research supports that nurses maintain a positive attitude toward IT implementation in healthcare.36-38
In the target settings, the MAP included multiple stages, each requiring the active participation of nurses beyond merely administering medications. One critical aspect of MAP was peer control, wherein nurses and physicians collaborated to prevent medication errors. Nurses could identify physician errors, while physicians also helped verify nurses’ calculations. Technology presents an alternative approach to this peer control system. In this regard, Elliset et al developed a high-alert drug administration system that automated double-checks to support nurses in error detection. Their study demonstrated that nurses performed equally well in error identification whether using the system or traditional peer control, but the system reduced detection time, making medication administration more efficient.
Beyond peer control, team-based collaboration plays a crucial role in MAP due to its complexity. Parry et al conducted a narrative review identifying teamwork and communication as key factors influencing nurses’ MAEs. 39 Their study indicated that poor collaboration between nurses and physicians increases the risk of medication errors. Participants in this research also acknowledged the importance of teamwork, highlighting its critical role in reducing medication errors and ensuring patient safety.
Another sub-theme extracted in this study was “Technology to improve nursing care quality.” One significant benefit of IT integration is its potential to reduce nurse burnout. Interviews in this study suggested that HIT could enhance motivation and decrease workload stress. Although research on this topic varies, 40 Bakken argued in an editorial that HIT innovations alone cannot mitigate clinician burnout without organizational support, a robust technology infrastructure, and national policies. 41 Participants in this study perceived technology as an ideal solution to various challenges, although this optimism may be linked to its limited use in their current settings.
This study provides valuable insights for policymakers regarding IT integration in pediatric and neonatal MAP. Developing a HIT intervention based on qualitative findings can improve acceptance among nurses. Additionally, this study employed a combination of qualitative methods, including interviews, observation, and informal discussions. Multi-method approaches are recommended in workflow analysis to capture a broader and more accurate understanding of work practices and overcome limitations of single-method designs, especially when participants may not fully articulate workarounds or hidden practices in interviews alone.28,42,43 This study has strengthened its findings by including direct observations.
Although this study was qualitative, and qualitative research is inherently not generalizable, it provides an in-depth exploration of MAP complexities and the role of IT in pediatric and neonatal care within a developing country context. As qualitative studies are at the lowest level of the evidence pyramid, future research should expand upon these findings using additional methodological approaches.
Several limitations should be considered when interpreting these findings. First, although the use of interviews, observations, and informal discussions enriched the data, the presence of an observer may have influenced nurse behavior (Hawthorne effect), potentially leading to under-reporting of medication errors or workarounds during observed periods. Second, self-reported experiences and attitudes are subject to social desirability bias; participants may have overstated their support for technology or underreported unsafe practices. Third, this study was conducted in a single developing-country context, and findings may not transfer directly to healthcare systems with different resources, staffing ratios, or technological infrastructure. Fourth, while nurses identified specific medication error types (overdose, underdose, LASA, missed care), we did not independently verify error rates through incident reports or direct clinical outcome measures, limiting the ability to quantify actual error prevalence. Fifth, the study captured perceptions of potential technological solutions, but it did not implement or test any technology; therefore, claims about technology’s effectiveness in reducing errors remain hypothetical in this context. Finally, data saturation was sought, but the sample size and setting may not capture the full range of MAP challenges present in other pediatric or neonatal units, such as those with fully integrated electronic prescribing or automated dispensing cabinets.
Despite these limitations, this study provides an in-depth, multi-method exploration of MAP complexities and the perceived role of IT in pediatric and neonatal care within a developing country context. As qualitative findings occupy a lower level of the evidence pyramid, future research should expand upon these results using quantitative methods, including error-tracking systems, pre-post technology implementation studies, and multi-center trials.
5. Conclusion
Understanding nurses’ experiences and attitudes toward the challenges of the Medication Administration Process (MAP) helps healthcare organizations and policymakers implement effective solutions. Integrating information technology into MAP can mitigate existing barriers and support strategic interventions, particularly in pediatric and neonatal care. Encouraging technological adaptation can foster IT acceptance and improve medication safety. This study offers policymakers and healthcare providers valuable insights into MAP challenges, guiding the integration of IT solutions in pediatric and neonatal settings.
6. Practice Implications
The findings from this qualitative study suggest several technology opportunities for improving the MAP in pediatric and neonatal settings: 1. Implement advanced clinical decision support systems:
Developing and integrating targeted CDSS tools that automate weight-based dose calculations and provide instant alerts for potential overdoses, underdoses, and Look-Alike/Sound-Alike (LASA) drug errors. This addresses the most common error types identified and moves error prevention from reliance on human vigilance to a systemic, technology-supported safeguard. 2. Integrate intelligent EHR Features:
This study highlighted enhancing existing EHR systems with embedded functionalities such as electronic nursing reminders to reduce missed nursing care and automated double-check systems for high-alert medications. This can streamline workflow, improve efficiency, and replicate the safety benefits of peer control without the same time investment. 3. Adopt a user-centered design approach for technological development:
This study recommends involving frontline nurses, physicians, and other end-users in the entire lifecycle of health IT design, implementation, and evaluation. Their direct input is crucial for creating intuitive and efficient tools tailored to the specific complexities and high-pressure dynamics of pediatric and neonatal care, thereby increasing adoption and effectiveness. 4. Strengthening organizational infrastructure and support:
This study recognized that technology alone is insufficient. To prevent burnout and ensure success, health systems must concurrently invest in adequate nurse staffing, provide comprehensive training on new systems, and foster a culture of safety that encourages error reporting without fear of blame. This aligns with the study’s finding that errors are often systemic. 5. Leverage established online platforms for training:
This study highlighted that the post-COVID-19 familiarity with online platforms presented an opportunity to roll out accessible, continuous education on new technology protocols, safe medication practices, and LASA drug recognition.
In summary, this study implied that the most effective path to modernizing MAP is not simply to adopt technology, but to implement thoughtfully designed, nurse-informed IT solutions within a supportive organizational framework that together address the root causes of medication errors.
Supplemental Material
Supplemental material - Exploring the Need for Health Information Technology Adoption in the Pediatric and Neonatal Medication Administration Process: A Qualitative Study
Supplemental material for Exploring the Need for Health Information Technology Adoption in the Pediatric and Neonatal Medication Administration Process: A Qualitative Study by Somaye Norouzi, Jila Agah, Zahra Sarkohi, Monir Sadat Nematollahi, Leila Ahmadian in The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
Supplemental material - Exploring the Need for Health Information Technology Adoption in the Pediatric and Neonatal Medication Administration Process: A Qualitative Study
Supplemental material for Exploring the Need for Health Information Technology Adoption in the Pediatric and Neonatal Medication Administration Process: A Qualitative Study by Somaye Norouzi, Jila Agah, Zahra Sarkohi, Monir Sadat Nematollahi, Leila Ahmadian in The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
Supplemental material - Exploring the Need for Health Information Technology Adoption in the Pediatric and Neonatal Medication Administration Process: A Qualitative Study
Supplemental material for Exploring the Need for Health Information Technology Adoption in the Pediatric and Neonatal Medication Administration Process: A Qualitative Study by Somaye Norouzi, Jila Agah, Zahra Sarkohi, Monir Sadat Nematollahi, Leila Ahmadian in The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
Supplemental material - Exploring the Need for Health Information Technology Adoption in the Pediatric and Neonatal Medication Administration Process: A Qualitative Study
Supplemental material for Exploring the Need for Health Information Technology Adoption in the Pediatric and Neonatal Medication Administration Process: A Qualitative Study by Somaye Norouzi, Jila Agah, Zahra Sarkohi, Monir Sadat Nematollahi, Leila Ahmadian in The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgments
The results described in this paper formed the first part of a thesis submitted by the first author for a Ph.D. degree in Medical Informatics. The authors would like to gratefully acknowledge the contribution of the participants.
Ethical Considerations
The study was conducted in accordance with the Declaration of Helsinki and the Committee on Publication Ethics (COPE) guidelines. In addition, the present study was approved by the research ethics committee of the Kerman University of Medical Sciences (see the supplemental materials B, C, and D). Before conducting and recording the interviews, the researcher introduced himself as the interviewer to the participants and explained the study’s objectives.
Consent to Participate
Verbal and written informed consent were obtained from all participants. The nurses volunteered to participate in the study and were assured that the data they gathered would be analyzed only by the researchers. In addition, the participants could withdraw from the study whenever they wanted. The rules and regulations developed by the ethics committee for observation and interview were followed.
Authors’ Contribution
SN, JA, ZR, MN, and LA conceptualized, designed, and conducted the study. SN drafted the manuscript with significant intellectual input from ZR, JA, MN, and LA assisted with revising the manuscript. Analysis and interpretation were done by SN, JA, ZR, MN, and LA. All authors approved the final version of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Vice Chancellor for Research at Kerman University of Medical Sciences provided support for this study but has not been involved in the study design, data collection, analysis, or interpretation of the results (# 403000345).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets used and analyzed during the current study are available from the corresponding author upon reasonable request.
Declaration of generative AI and AI-assisted technologies in the writing process
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.