
Abstract
This article reports findings from formative research on translating key elements of the National Institute on Alcohol Abuse and Alcoholism (NIAAA) and American Academy of Pediatrics Practitioner’s Guide for pediatric alcohol misuse to a computerized web- and mobile-compatible format with patient risk screening and tailored decision support content. Five practitioners at an urban primary care center used a prototype computerized version of the NIAAA/American Academy of Pediatrics Practitioner’s Guide with 80 adolescent patients during routine health-care visits. Practitioners reported a high level of practitioner and adolescent patient engagement and satisfaction with the prototype. Study findings indicate that computerization of the NIAAA Practitioner’s Guide is feasible and well accepted by providers and adolescent patients and could be useful for addressing alcohol misuse in primary care settings.
Keywords
Introduction
Epidemiological surveys show that nearly a quarter of eighth graders reported alcohol use during their lifetimes (Miech et al., 2019). By 12th grade, approximately 30% drank alcohol during the past 30 days, with nearly 14% reporting recent binge drinking (Miech et al., 2019). Alcohol misuse during adolescence has adverse neurophysiological impacts during a critical time of accelerated brain development (Lubman, Yucel, & Hall, 2007; Squeglia, Jacobus, & Tapert, 2009; Volkow & Li, 2005; White & Hingson, 2019). In the short term, adolescent alcohol misuse is associated with health risk behaviors including unsafe sexual practices and sexual victimization (Fergusson & Lynskey, 1996; Miller, Naimi, Brewer, & Jones, 2007), deteriorating academic performance (Brown et al., 2008; Miller et al., 2007), and in some cases, intensification of mental health problems including suicidality (Duncan, Alpert, Duncan, & Hops, 1997; Windle, 2004). Over the longer term, adolescent alcohol use is associated with a range of negative outcomes, including increased risk of developing substance use disorders in adulthood (Englund, Egeland, Oliva, & Collins, 2008; Hingson, Heeren, & Winter, 2006), aggression, crime, suicidal ideation (Duncan et al., 1997), and mortality (Clark, Martin, & Cornelius, 2008).
The Health-Care System: An Important Opportunity for Early Intervention
Given the magnitude of this problem and its myriad consequences, preventing early initiation of alcohol use and intervening in risky drinking are important public health objectives. Yet, the majority of adolescents with nascent alcohol use problems are not identified, and less than 1 in 10 young people who need alcohol treatment actually receive it (Substance Abuse and Mental Health Administration, 2013). Nevertheless, most adolescents access the health-care system at least annually (Hingson, Zha, Iannotti, & Simons-Morton, 2013). Thus, pediatricians are in a unique position to identify and intervene in risky drinking. A number of studies suggest that even brief interventions delivered in health-care contexts can be effective in reducing risky drinking among young people (Mitchell, Gryczynski, O'Grady, & Schwartz, 2013). As such, the American Academy of Pediatrics (AAP) and the National Institute on Alcohol Abuse and Alcoholism (NIAAA) recommend that pediatricians provide alcohol use screening and intervention as a best practice in adolescent medicine (American Academy of Pediatrics, 2011). Nevertheless, low physician uptake of screening and brief intervention for adolescent alcohol use has been a long-standing problem (Derges et al., 2017; Johnson, Jackson, Guillaume, Meier, & Goyder, 2011).
The NIAAA/AAP Practitioner’s Guide
In order to spur the adoption of screening and intervention in adolescent medicine settings and promote the use of evidence-based strategies, in 2011 the NIAAA and AAP jointly developed a screening tool for youth alcohol misuse using drinking frequency risk cutoffs derived from large-scale epidemiological data (Chung et al., 2012; Levy et al., 2016). These data indicated that drinking frequency and age could be used to efficiently determine whether youth should be categorized into low-, moderate-, or high-risk tiers regarding alcohol-related problems (Chung et al., 2012). Working in partnership, NIAAA and AAP jointly published the screening tool and detailed guidelines for how to use it in a 47-page guidebook entitled Alcohol Screening and Brief Intervention for Youth: A Practitioner’s Guide (National Institute on Alcohol Abuse and Alcoholism, 2011). The purpose of the Practitioner’s Guide, only available in static hardcopy and pdf formats, is to equip pediatricians and other health-care practitioners with information on how to appropriately screen and counsel youth 9 to 18 years of age about their drinking. The Practitioner’s Guide includes decision trees and graphical resources. In a major dissemination effort, high-quality, full color gloss copies were sent to pediatricians across the United States. An abbreviated pocket guide was also developed and widely distributed.
Simple in concept, complex in practice
While straightforward in concept, the screening and intervention resources articulated in the Practitioner’s Guide are, in fact, highly tailored. The screening tool asks questions about alcohol use frequency and drinking patterns by the adolescent patient as well as by the patient’s peer network, but the recommended question ordering is different based on the patient’s age and school status (for younger adolescents, screening begins with questions about the drinking behavior of their peer network; for older adolescents, the initial questions focus on their own behavior). Certain questions are asked only of certain types of patients, with more detailed behavioral assessment depending on their responses. Tailored follow-up probes are applied depending on what patients report. Assessment of binge drinking behavior carries different implications based on gender and age. The tailored questions and sequences triage patients into three distinct tiers of risk (low, moderate, or high) based on a combination of the patient’s frequency of alcohol use and age. For the risk assessment portion, the Guide provides a decision support graphic that plots frequency of alcohol use against age and overlays levels of risk based on empirically derived cutoffs (Chung et al., 2012). Recommended intervention approaches are then conditionally branched by risk level, with further tailoring based on patients’ other risk behaviors and receptivity to changing their behavior.
Different levels of risk have different suggested approaches (e.g., brief advice, motivational interviewing, possible referral to more intensive services), and the Guide provides suggested scripts, practical tips, and exercises to guide practitioners in intervention delivery. The 47-page Guide contains a decision tree algorithm spread across six pages to guide what practitioners are supposed to say and do in different situations. This algorithm merely represents an overview of recommended practitioner actions. The service delivery algorithm consists of several components, each of which are themselves tailored based on patient characteristics and the behaviors they report: (i) screening; (ii) risk assessment; (iii) intervention resources for patients with alcohol risk profiles of (a) abstinence (prevention), (b) low risk, (c) moderate risk, and (d) high risk; and a final component of (iv) tailored follow-up.
Many primary care practices are extremely busy, seeing a high volume of patients with a diverse array of needs. Given the time pressures and competing demands of the modern health-care environment, many recommended preventive services are delivered inconsistently or not at all (Yarnall, Pollak, Ostbye, Krause, & Michener, 2003). Primary care providers need tools that promote efficiency while facilitating the provision of high-quality, patient-centered care.
The Present Study
The present study is a pilot proof-of-concept feasibility study involving practitioners and their adolescent patients. The study was designed to translate and streamline key elements in the NIAAA’s Practitioner’s Guide for pediatric alcohol misuse to a computerized web- and mobile-compatible format and to examine the feasibility and acceptability of the computerized version of the Guide among practitioners in a health-care setting. The study was approved by the Institutional Review Board of Friends Research Institute.
Methods
Setting
The study was conducted at a community-based, federally qualified health center that provides comprehensive behavioral health and primary health-care services to medically underserved and uninsured individuals. This urban health center operates in three locations and has been in operation for more than 40 years.
The Computerized Practitioner’s Guide
The Computerized Practitioner’s Guide (CPG) is a HIPAA-compliant, mobile-friendly, tablet-based software program designed to improve the delivery of high-quality alcohol screenings and appropriate interventions. It was designed to mirror the hardcopy version of the Practitioner’s Guide, while streamlining content delivery and providing multimedia content to enhance its clinical utility and uptake. Automated algorithms were designed to ensure that patients were asked the correct questions at the correct time and in the correct order. Risk-level assessments, which integrated multiple information points to triage patients into low-, moderate-, or high-risk tiers, were handled automatically as a background calculation, with the goal of eliminating errors and minimizing distractions from the clinical encounter. Practitioners were seamlessly guided through the appropriate intervention strategy based on the patient’s risk level using scripts and prompts.
Study Eligibility Criteria
The study recruited practitioners (pediatricians, family practice physicians, and nurse practitioners) from a health center that serves adolescent patients between 9 and 18 years of age. The adolescent patients who received pediatric services from the practitioners that participated in the study were determined by the Institutional Review Board not to be participants in the research study, since all of the content of the Practitioner’s Guide is recommended as a best practice and data collection focused on the experiences of practitioners.
Participants
Practitioners who met study eligibility criteria (treating patients between 9 and 18 years of age) and provided written informed consent to participate were included in the study. Between February and March of 2018, five practitioners were screened and consented by research staff at the health center.
CPG Orientation
During an initial face-to-face orientation session with practitioners, research staff conducted a brief tutorial and CPG overview. This session occurred in the primary care clinic and lasted 10 to 15 minutes. A subsequent 20- to 30-minute training involving a guided walkthrough of the program including its features and capabilities, login information, and guidance regarding entering adolescent patient demographic information was also provided to each provider immediately prior to launching their delivery of the CPG pilot (necessary because the pilot CPG was not integrated into the clinic’s electronic health record [EHR] system).
CPG Implementation
Practitioners used the resources in the CPG to conduct the alcohol-focused part of their medical visit to help them appropriately counsel youth about their drinking. Practitioners were provided a unique username and password to log into the CPG that was encrypted in the database. All data were encrypted in transit, end to end, and at rest. Log data were also encrypted to mitigate risk of protected health information stored in log files, and the program ran through a HITRUST-certified, HIPAA-compliant cloud hosting environment. Technical support services were available from an outside technology vendor through the use of an 800 number, e-mail, and instant messaging to address potential technology-related issues. During the ensuing feasibility trial, no technology-related issues were reported to research staff nor were any technical support services utilized by participating practitioners.
Results
Feasibility Trial
During the feasibility trial, five practitioners used the computerized prototype with approximately 15 to 17 of their adolescent patients each (n = 80 total; ages 9–18 years, consistent with the age range of the Practitioner’s Guide) during the private confidential portion of their medical visit. Following completion of the trial, practitioners completed a quantitative questionnaire on feasibility and usability (asked in a Likert-scale agreement format) and a semistructured qualitative interview. Interviews were recorded and transcribed. Participant responses were compared and contrasted using a directed content analysis approach (Hsieh & Shannon, 2005).
Participant Characteristics
Three of the five practitioner participants were female, three were Black, one was Hispanic, one was White, two were pediatricians, and three were nurse practitioners. Among the 80 adolescent patients screened by the practitioners using the CPG, 44 (55.0%) were female, 18 (22.5%) were in elementary school, 18 (22.5%) were in middle school, and 44 (55.0%) were in high school. Forty percent reported having friends who drank alcohol, while 18.8% reported drinking alcohol themselves in the past year.
Feasibility and Usability
Table 1 shows the mean responses of practitioner participants to the feasibility questionnaire. The highest mean agreement was found for the statements “My adolescent patients seemed to find the iPad app easy to use” and “Using the iPad app to screen for alcohol use was preferable to using a paper screener.” The highest levels of disagreement were found for the statements “I would not want to use an app like the NIAAA screener in regular clinical practice” and “I thought the app's information for providers had too much text.” Thus, the responses to the positively and negatively framed questions illustrate that the CPG was perceived as feasible and useful. Based on the responses to the negatively framed items, it appears that practitioner participants would be amendable to adopting the CPG into their normal practice and believe that it could potentially be helpful in improving the delivery of high-quality alcohol screenings.
Practitioner’s responses to the feasibility questionnaire (N = 5).
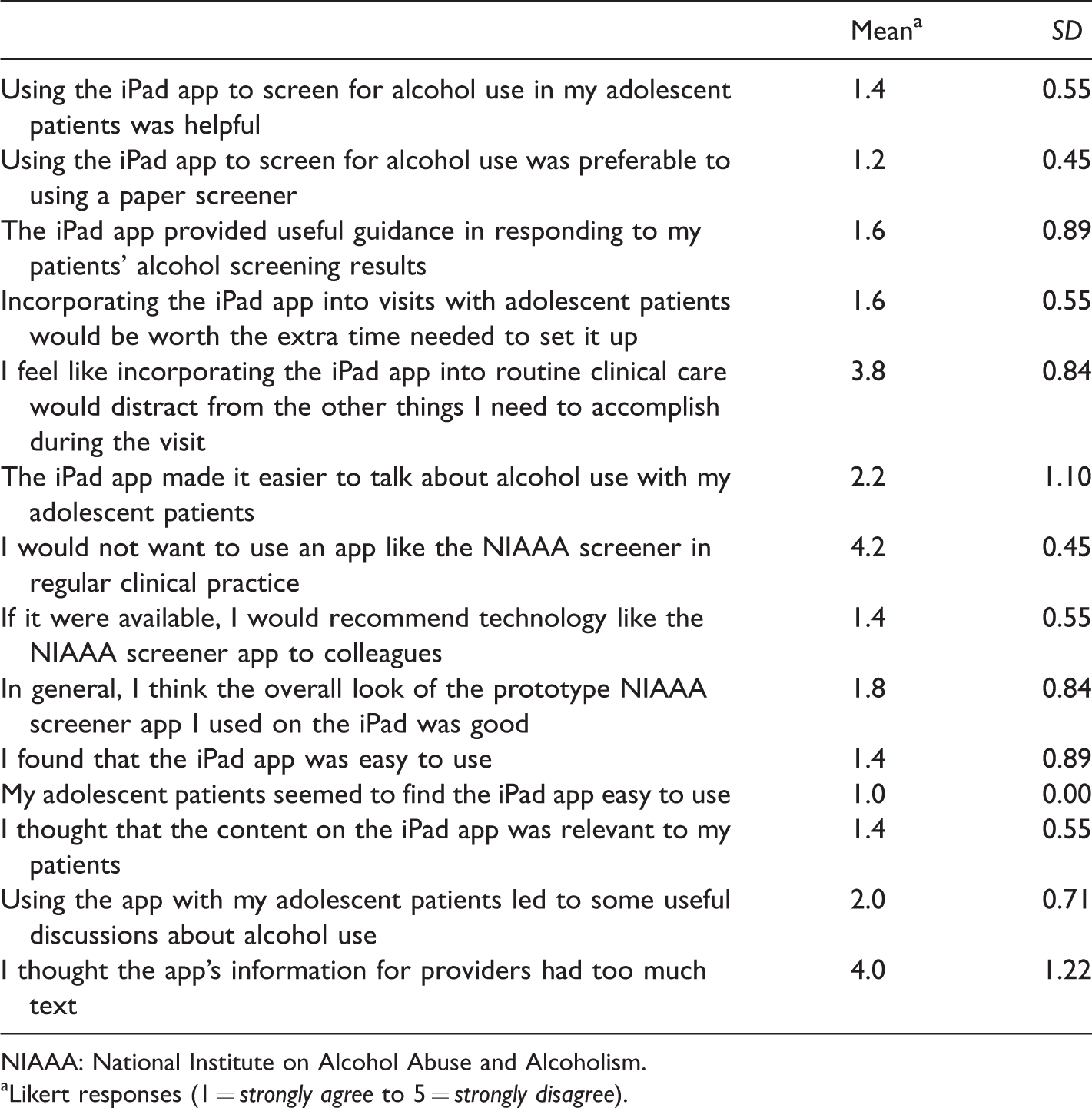
NIAAA: National Institute on Alcohol Abuse and Alcoholism.
aLikert responses (1 = strongly agree to 5 = strongly disagree).
Figure 1 shows practitioner participants quotes in response to several open-ended questions. These responses suggest that the CPG was feasible and promising, comfortable and enjoyable for youth to use, and helpful in terms of increasing youth comfort in discussing alcohol use issues.
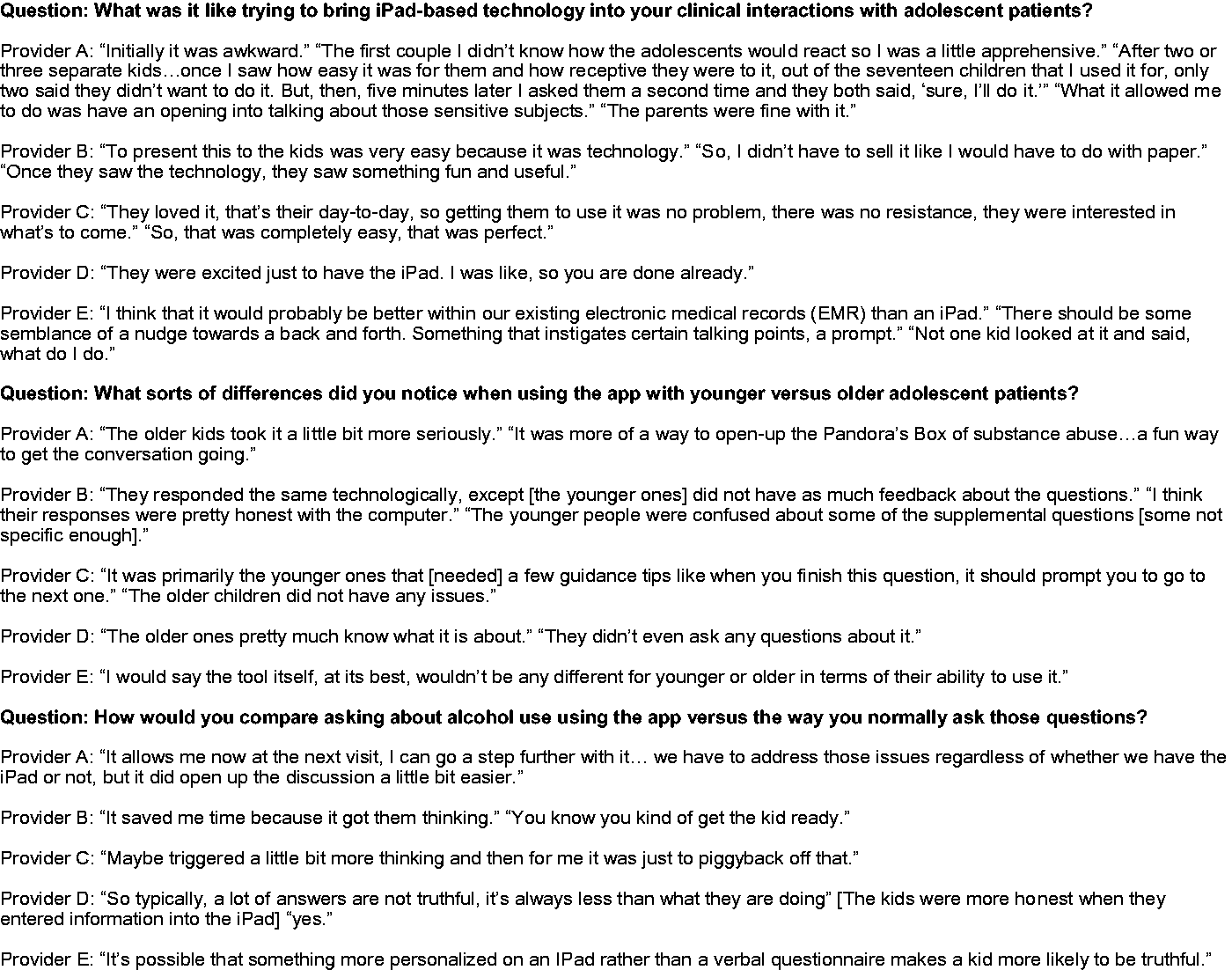
Practitioner’s qualitative interview responses (N = 5).
In addition to the information provided in Figure 1, practitioner participants expressed satisfaction with the length of the CPG process and indicated that it worked well with the flow and was sufficiently short that their adolescent patients did not get bored. However, practitioners also noted that in some cases the guidance provided was too detailed and required additional time to review in order to provide appropriate feedback to patients.
Overall, however, these results indicate a high level of practitioner and adolescent engagement, comfort, and satisfaction using the CPG.
Suggestions for Future Enhancements
During the qualitative interviews, practitioners also offered suggestions for improving the prototype, including (a) clarifying screener questions and enhancing interactive content including improved visuals and (b) integration with EHR systems in order to increase the usability of the platform.
Discussion
Overall, the feasibility trial demonstrated proof of concept for the CPG with practitioners reporting that their adolescent patients indicated a high level of engagement and satisfaction using the platform. Practitioners indicated prototype utility with respect to (a) a preference for using the CPG compared to the standard hardcopy format and (b) increased comfort in discussing alcohol use with adolescents using the prototype. Practitioners also offered useful feedback on how to improve subsequent iterations of the prototype.
A cautious interpretation of study findings is recommended in light of study limitations. First, the study consisted of a small convenience sample derived from a health center that agreed to use the CPG in a proof-of-concept feasibility study. The feasibility trial did not have a comparison group and did not track practitioner screening and intervention practices prior to implementing the CPG. In addition, the small sample size of five practitioners may not provide sufficient data to make firm conclusions regarding the acceptability and usability of this prototype technology. Despite these limitations, this small study provided proof of concept for the CPG indicating that implementation of the technology in a primary care setting was feasible.
Computerization offers a number of potential advantages for empowering practitioners to deliver best practice alcohol screening and intervention services more consistently. By streamlining practitioners’ ability to screen for and intervene in youth alcohol use, the CPG may have clinical utility and build upon the existing NIAAA/AAP hardcopy resources. In addition, further development of the technological architecture to support integration of the software into EHRs could make the CPG uniquely responsive to workflow considerations in modern primary care, potentially improving uptake by practitioners. Finally, the CPG may be particularly appealing to specific patient populations, especially younger people with an affinity for technology (Marsch, 2011; Marsch, Carroll, & Kiluk, 2014; Ondersma, Grekin, & Svikis, 2011; VanDeMark et al., 2010), potentially increasing the appeal, comfort, and widespread dissemination and adoption of this type of computerized screening tool.
There are a number of directions for future research with the CPG. Future research should further develop and enhance intervention resources within the CPG, integrate the CPG with EHR systems, evaluate its clinical uptake on a larger scale, establish the reliability and validity of screening via the CPG against alternative self-report approaches as well as alcohol use biomarkers, and investigate the effectiveness of using the CPG in primary care to reduce risky drinking among adolescents.
Supplemental Material
DRE894960 Supplemental Material - Supplemental material for Computerizing NIAAA’s Best Practices for Youth Screening and Brief Intervention: A Proof-of-Concept Pilot Study of an Automated Alcohol Screening and Intervention Resource Tool
Supplemental material, DRE894960 Supplemental Material for Computerizing NIAAA’s Best Practices for Youth Screening and Brief Intervention: A Proof-of-Concept Pilot Study of an Automated Alcohol Screening and Intervention Resource Tool by Steven B. Carswell, Shannon G. Mitchell, Jan Gryczynski and Elizabeth Lertch in Journal of Drug Education
Footnotes
Acknowledgments
We wish to thank Dr. Beverly Ruffin, our NIAAA Program Official. We would also like to thank the staff at the participating health center for their assistance with this project. Finally, we wish to thank our project staff for their efforts related to this study and Ms. Carly Bickel for manuscript preparation and assistance regarding journal submission.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Two of the authors, Drs. Carswell and Gryczynski, are co-owners of the small business to whom the award was made. The other authors, Dr. Mitchell and Ms. Lertch, do not have any declarations of interest to report. The authors alone are responsible for the content and writing of this paper.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the National Institute on Alcohol Abuse and Alcoholism (NIAAA), Grant Number 1R41 AA 024354-01A1 (PI: Mitchell). The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIAAA.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.