
Abstract
The present study investigated the prevalence and co-occurrence of addictions to tobacco, alcohol, other drugs, food/eating, the internet, texting, video games, shopping, love, sex, exercise, work, and gambling among American Indian (AI) youth in California. As with previous work in other cultural groups, the most prevalent addictions were love, internet, and exercise, though prevalence and co-occurrence of these addictions were relatively high among AI youth. A negative life events measure was associated with all the addictions, suggesting that life stressors are associated with high rates of multiple types of addictions among AI youth. There is a need for more research to better understand the relations of life stressors with multiple addictions among AI youth as well as how to remediate these behaviors.
Various substances (e.g., alcohol) and behaviors (e.g., gambling, gaming) meet the criteria for addiction: appetitive effects, satiation, preoccupation, and loss of control (American Psychiatric Association, 2013; Sussman, 2017; Sussman & Sussman, 2011; World Health Organization, 2018). While not formally recognized as such, many other behaviors (e.g., shopping, sex, exercise, internet) meet those criteria for addiction and are gaining in recognition by researchers and practitioners (Sussman et al., 2011). Moreover, addictions tend to co-occur; one review estimated that among U.S. adults, 23% suffered from two or more addictions in the past 12 months (Sussman et al., 2011). The possibility that one may experience multiple addictions at the same time is an important phenomenon, highlighting the complexity of interrelationships among different addictions. It is important to understand whether there are common underlying correlates or predictors of the addictions (Haylett et al., 2004; MacLaren & Best, 2010; Najavits et al., 2014; Sussman, 2017).
Addictions cause a substantial proportion of morbidity and mortality in American Indian (AI) communities (e.g., Jacobs-Wingo et al., 2016; Skewes & Blume, 2019). No previous empirical studies have examined the prevalence or correlates of multiple addictions among AI youth or adults, though one review article highlighted the relatively high prevalence and co-occurrence of alcohol, nicotine, and other drug use among AI adults, compared with four other ethnic groups in the United States (Luczak et al., 2017). Research on addictions among AI youth is important, because they have the highest prevalence of cigarette, alcohol, and marijuana use, relative to other groups (Hilton et al., 2018; Hoffman et al., 2019, Luczak et al., 2017; Skewes & Blume, 2019; Stanley & Swaim, 2015), indicating a dire need for prevention and treatment programs.
Measurement of Multiple Addictions
One barrier to studying multiple addictions is that it is not clear how to measure the presence of multiple addictions at the same time among participants. Several studies have used an “addiction matrix” measure to assess multiple addictions, as opposed to use of extensive measures of separate addictions, to reduce participant burden and redundancy in assessment (i.e., repeatedly using the same type of criteria of addiction, such as preoccupation or loss of control, to assess a large number of potentially addictive behaviors). Several previous studies have examined multiple addictions as a matrix measure (e.g., Alexander & Schweighofer, 1989; Christo et al., 2003; Cook, 1987; Chuang et al., 2017; Greenberg et al., 1999; Haylett et al., 2004; MacLaren & Best, 2010; Najavits et al., 2014; Sussman et al., 2014; Tsai et al., 2016). The matrix measure allows individuals to self-report whether they have been addicted or not addicted within their lifetime or recently (e.g., in the past 30 days) using one item per type of addiction arranged in a matrix format. The definition of addiction is provided to subjects in the instructions for completing the measure and includes mention of recurrent behavior to achieve an appetitive effect, loss of control, and negative consequences to self or others (Sussman, 2017). In summary, the matrix measure is advantageous because it is practical, economical, and can assess several addictions at the same time.
Prevalence of Multiple Addictions Across Cultural Groups
Almost no research has examined the interrelationships of addictive behaviors among ethnic groups in the United States. The few existing studies have focused nearly exclusively on the co-occurrence of substances and gambling behaviors (Luczak et al., 2017). Only a select few studies have assessed the prevalence of multiple addictions among adolescents living in diverse cultural contexts. Sussman et al. (2014, 2015) examined the use of a multiple addiction item matrix among former continuation high school youth in the United States. Tsai et al. (2016) used the same measure among Russian and Spanish high school youth. Their studies examined past 30-day and lifetime prevalence and co-occurrence of 11 addiction items (i.e., cigarettes, alcohol, hard drugs, shopping, gambling, internet, love, sex, eating, work, and exercise; see Sussman, 2017 for details regarding each of these addictions). The most prevalent lifetime and past 30-day addictions were internet, love, and exercise across the three samples (see Table 1). Lifetime co-occurrence of two or more addictions among youth from United States (n = 717; average age = 19.8, SD = 0.8; 66.5% Hispanic), Russia (n = 717; average age = 16.3, SD = 1.0), and Spain (n = 818; average age = 14.9, SD = 0.9) were 61.5%, 40.1%, and 54.8%, respectively.
A Comparison of Ever and Past 30-Day Self-Reported Addiction to Selected Substances and Behaviors: Proportions of Sample.
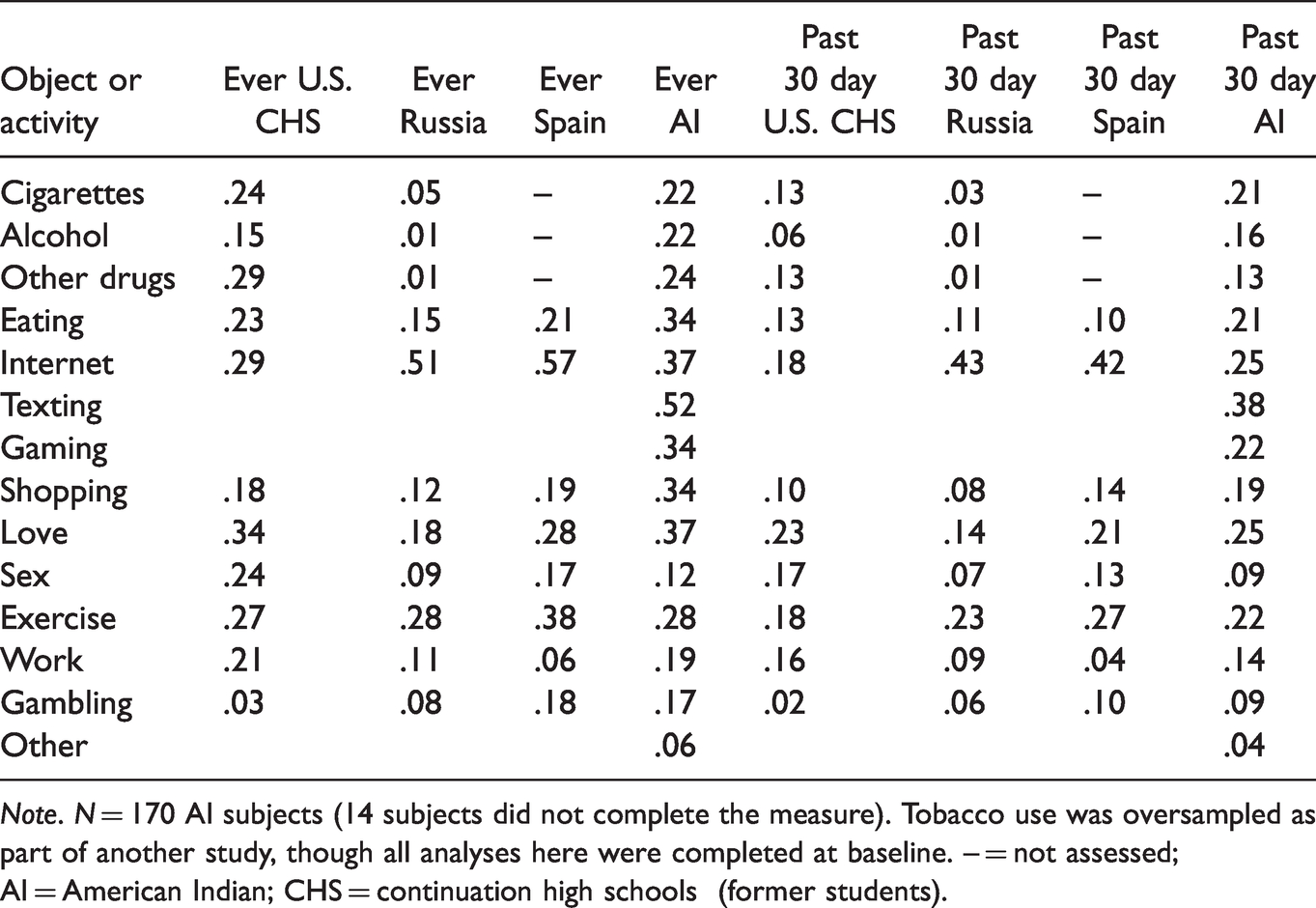
Note. N = 170 AI subjects (14 subjects did not complete the measure). Tobacco use was oversampled as part of another study, though all analyses here were completed at baseline. – = not assessed; AI = American Indian; CHS = continuation high schools (former students).
Correlates of Addictions Among AI Youth and the Present Study
Explanations for the elevated risk for addiction among AI youth include historical trauma, lack of social support, ongoing oppression, and related depressive symptoms (Hilton et al., 2018; Paul et al., 2017; Skewes & Blume, 2019; Soto et al., 2015). To design effective prevention or cessation programming for addiction-related adverse health outcomes, it is important to understand the prevalence and correlates of multiple addictions among AI youth. However, no study has attempted to examine correlates of both substance and behavioral addictions among AI youth.
The present study examined prevalence and co-occurrence of substance and behavioral addictions among these AI youth in California, comparing them with our previous studies (Sussman et al., 2014, 2015; Tsai et al., 2016). We also examined correlates of these addictions including ethnic identity, social acceptance, depression, and negative life events, after controlling for age, sex, and residence on a reservation. Addictions included an index of lifetime and past 30-day substance addiction, behavioral addiction, or substance + behavioral addiction. We hypothesized that ethnic identity and social acceptance would be protective against substance and behavioral addictions, while depressive symptoms and negative life events would be risk factors.
Method
Sample Recruitment
Participants were 156 AI adolescents at six AI schools and after-school programs on Tribal lands in northern, central, and southern California in March–September 2018. AI investigators who had collaborative relationships with the Tribal agencies and schools recruited the sites. Each site provided formal approval of the protocol, confidentiality, and human subjects protections. The university’s Institutional Review Board approved the study. AI adolescents at the participating sites were eligible to participate if they were 13 to 18 years of age, self-identified as AI, lived in California, and provided written parental/guardian consent and youth assent.
Survey Procedures
The AI project consultant explained the study and distributed the surveys. We provided participants with identification numbers that we place on the front of the survey. Participants completed the paper-and-pencil survey and placed the completed surveys in envelopes to maintain confidentiality. This report details data from the baseline survey, before any health education occurred.
Measures
We assessed ethnic identity with the 12-item Multigroup Ethnic Identity Measure (Roberts et al., 1999), which asks respondents to rate statements on a 4-point scale ranging from strongly disagree to strongly agree. Sample items include, “I have spent time trying to find out more about my ethnic group, such as its history, traditions, and customs” and “I have a clear sense of my ethnic background and what it means for me” (α = .96).
We assessed depressive symptomatology with the Center for Epidemiologic Studies-Depression Scale (Radloff, 1977; 20-item scale; α = .92). For example, we asked subjects to report how often during the past week they felt depressed, on a 4-point Likert scale ranging from rarely or none of the time (less than 1 day) to most or all of the time (5–7 days). This scale has been used previously among adolescents (e.g., Galaif et al., 1998).
We assessed social acceptance through use of four items from a familial acceptance measure (e.g., “How much do you feel that your family understands you?” and “How much do you feel that your parents care about you?” e.g., Fuemmeler et al., 2012) with the addition of four other items (e.g., “How much do you feel cared about by adults outside your family [neighbors, friends’ parents, etc.]?” “How much do you feel cared about by teachers?” “How much do you feel cared about by church leaders?” and “How much do you feel cared about by Tribal leaders?”) to create a more general, social acceptance measure relevant to AI youth (alpha coefficient = .92).
We assessed negative life events in terms of past 1-year occurrence (“Yes” or “No”) of potentially stressful events that may happen in an adolescent’s life. We provided a checklist of eight events, which included events that may have happened directly to the adolescent (e.g., “I got disciplined or suspended from school or work,” “I was a victim of a violent or abusive crime”) or may have occurred at the family level (e.g., “There were a lot of arguments that happened at home,” “A new person joined the household [baby or young child, grandparent, stepbrother, or sister, stepparent, other]).” The checklist was a short version of the Adolescent Life Event Checklist (Newcomb & Harlow, 1986) used in several studies (e.g., Pokhrel et al., 2018). Because the negative life event checklist represents largely independent, discretely occurring events, internal consistency (i.e., Cronbach’s alpha) is not relevant (see Pokhrel et al., 2018)
The addiction matrix measure header for the AI youth questionnaire was “Sometimes people have an ‘addiction’ to a certain drug or other object or activity. An addiction occurs when people experience the following: They do something over and over again to try to feel good, for excitement, or to stop feeling bad; they can’t stop doing this even if they wanted to; bad things happen to them or to people they care about because of what they are doing.” Following the header, we asked subjects, “Have you ever been addicted to the following things?” and “Do you feel you are addicted to them now (in the past 30 days)?” We provided 13 response categories, and a 14th response category allowed participants to indicate any addiction they felt were not addressed in the previous categories by asking, “Any other addiction? Please identify:” The categories included cigarette smoking, alcohol drinking, other drugs (i.e., marijuana, cocaine, stimulants, hallucinogens, inhalants, XTC, opiates, valium, or others); eating (e.g., way too much food each day, binge eating); internet browsing (i.e., surfing the web); texting (i.e., cell phone use); online or offline video games (e.g., PS3, Xbox, Wii); shopping; love; sex; exercise; work; and gambling (as in Chuang et al., 2017). Participants provided only six open-ended responses, which appeared irrelevant (e.g., depression, none), and so were not included in the analysis.
Analysis
We calculated the sample prevalence proportion of lifetime and past 30-day items for the 13 addictions and the co-occurrence of two or more lifetime and past 30-day addictions. Next, we created six indices. These consisted of the sums of combinations of the addictions (lifetime and past 30-day total addiction with the sum of 13 items, each; lifetime and past 30-day substance addiction with a sum of four items each [cigarettes, alcohol, other drugs, and food]; and lifetime and past 30-day behavioral addictions with a sum of nine items, each). Six multiple regression models examined the associations between the hypothesized predictor variables of ethnic identity, depressive symptoms, social acceptance, and negative life events with the six addiction indices (lifetime and past 30-day combination, substance, and behavioral addictions), controlling for covariates (age, sex, and whether or not the youth lived on a reservation). The analyses did not include multilevel models because the intraclass correlations were less than 0.1.
Results
The mean age of the AI youth was 15.3 years (SD = 1.69); 55% were female, and 53% lived on a reservation. Respondents reported affiliations with more than 30 Tribes (names omitted for confidentiality). The four most prevalent lifetime addictions were texting (52%), internet (37%), love (36%), and shopping (33%). The four most prevalent past-month addictions were texting (39%), internet (26%), love (26%), and cigarettes (23%). This pattern of prevalence of the addictions was similar with that in previous U.S., Russia, and Spain studies (see Table 1). If a participant experienced one addiction, the co-occurrence of a second or more lifetime and past 30-day addictions was 73.72% and 55.13%, respectively.
All multiple regression models except one were significant—Fs(7, 149) ranged from 2.47 to 7.49. The model predicting lifetime behavioral addictions was nonsignificant (F = 1.39). Significant effects are shown in Table 2. Age was a significant covariate in five of six models. The older the youth (ages ranged from 13 to 18 years), the more likely the youth exhibited a substance or a behavioral addiction, or both. Ethnic identity failed to predict addictions in any model. Social acceptance significantly predicted lifetime substance addictions. The greater the perceived social acceptance, the fewer the lifetime number of substance addictions. The depressive symptoms measure was only associated with the past 30 days behavioral addiction model. The more depressed the participant, the more addictions that were reported. Finally, the negative life events measure was a significant predictor in five of six models (marginal on the sixth). Negative life events were associated with more substance or behavioral addictions, or both.
Multiple Regression Predicting Number of Total, Substance, and Behavioral Addictions.
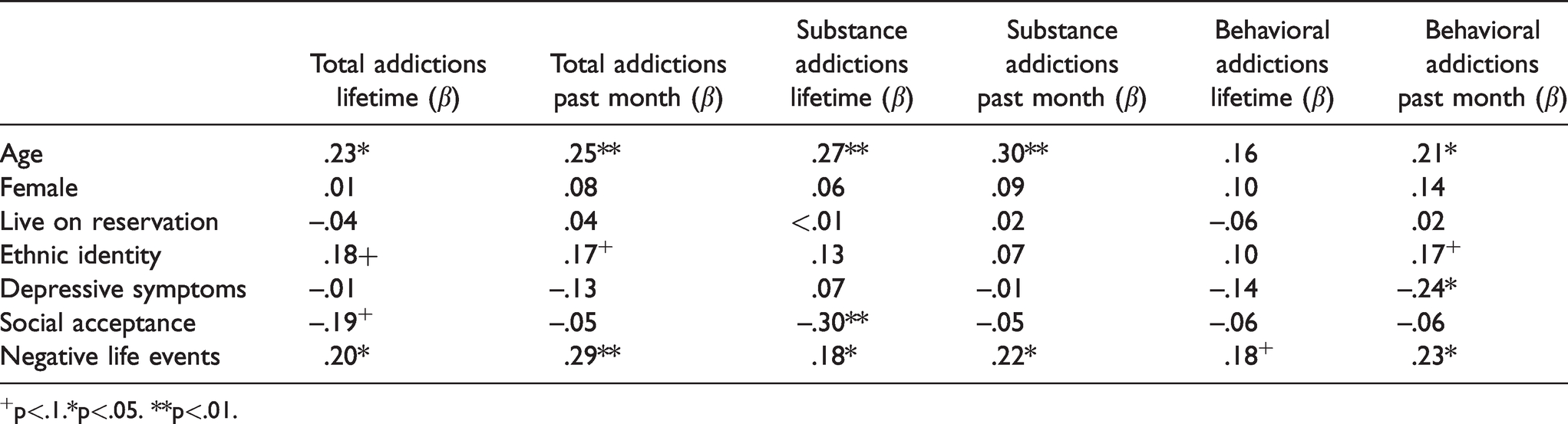
+p<.1.*p<.05. **p<.01.
Discussion
AI youth reported a pattern of prevalence of substance and behavioral addictions very similar to previous samples of a similar age range (e.g., love, internet), despite living in very different cultural contexts. However, recent (past 30 day) prevalence of multiple addictions, and their co-occurrence, tended to be higher than other groups. While previous work has identified alcohol, tobacco, and other drug use (ATOD) addictions as being relatively high among AIs, this is the first study to identify current behavioral addictions as also being relatively high.
The negative life events measure was the most consistent predictor of multiple addictions. This is consistent with previous studies that focused on single, substance addictions (Skewes & Blume, 2019). This study extends previous findings by showing that negative life events can manifest in multiple addictions. Contrary to expectations, ethnic identity was not protective against multiple addictions. AI identity can fluctuate throughout the life course; adolescents may reject AI identity in the effort to “fit in” with non-AI peers but revisit cultural traditions later in life (Brown et al., 2016). With the burden of hundreds of years of institutional oppression and racism, AI youth may find it challenging to gain a sense of belonging and ethnic identity at this stage in life. Resilience is typically protective against substance use (Stumblingbear-Riddle & Romans, 2012; Weiland et al., 2012; Wingo et al., 2014). It is important to understand addiction and related protective and risk factors to support substance use prevention programs for AI youth, including how to impart resilience (Kelley et al., 2019; Stumblingbear-Riddle & Romans, 2012).
While there is a paucity of evidence-based ATOD prevention and cessation programs for indigenous peoples (e.g., Soto et al., 2018), there are some promising substance abuse prevention programs that specifically target AI urban and Tribal youth and young adults, with approaches to improve refusal skills, increase self-efficacy, address drug-related attitudes and beliefs, and increase spiritual well-being (see Kelley et al., 2019). For example, to address alcohol and drug use prevention among urban AI youth, a culturally appropriate program called “Motivational Interviewing and Culture for Urban Native American Youth (MICUNAY)” integrates motivational interviewing with the use of traditional AI practices (Dickerson et al., 2016). In particular, this program integrates motivational interviewing with use of the Medicine Wheel, the latter which focuses on emotional, mental, physical, and spiritual aspects of well-being. Other promising programs include the Wellbriety Movement (Coyhis & Simonelli, 2008), which is a process of taking the participant through a culturally focused form of intervention, treatment, and the eventual wellness formed around recovery; Cultural Immersion Camp (Gone & Calf Looking, 2011); and of Healing the Canoe (Thomas et al., 2011), both of which integrate cultural traditions, norms, and activities to support the sobriety of participants. Each of these programs offer community-based drug abuse prevention material immersed in AI cultural tenants and spiritual revitalization, along with evidence-based life skills instruction. Literature reviews by Greenfield and Venner (2012) and Walsh and Baldwin (2015) assert that AI youth engaged in cultural practices, such as use of talking circles, involvement of the Tribal community, and engagement in ceremonial traditions reported greater positive outcomes than those who were not afforded such opportunities.
Limitations and Conclusions
This was a convenience sample of AI youth who attended AI schools or after-school programs in California. Findings might not generalize to AI youth in other geographic areas. This cross-sectional study does not permit temporal or causal inferences. Still, the results are novel and suggest needed research directions. AI youth reported a relatively high prevalence of substance and behavioral addictions. Clearly, more research with larger representative samples is needed. Negative life events appear to be correlated with many of the addictions reported by the participants. Attention to historical trauma as a potential root cause of negative coping mechanisms of addictive behaviors among AI youth and young adults is essential. Programming for AI youth may need to incorporate methods to alleviate posttraumatic symptoms, as well as instruction in life skills, and might target both substance and behavioral addictions.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the California Tobacco Related Disease Research Program Grant #26IR-0031 (Claradina Soto, PI).